
Abstract
This paper describes the sex work characteristics and factors associated with syphilis among female sex workers (FSWs) in Dimapur district of high HIV prevalence Indian state, Nagaland. The study recruited 426 FSWs in 2006 using respondent-driven sampling. The prevalence of syphilis was 21.1% and HIV prevalence was 11.7%. Approximately half were under 25 years of age. Clients were solicited mainly in public places (32.7%), while hotels/lodges/rented rooms were the most common places of entertainment (57.2%). Condom use during the last sex was 36.5% with occasional and 27% with regular clients. Being married, being widowed/divorced/separated, being illiterate or having a history of drug use increased the likelihood of syphilis infection. Entertaining clients in bars/booze joints decreased the probability of syphilis. FSWs who moved between soliciting in public places or bars/booze joints and then entertaining in hotels/lodges/rented rooms had a higher vulnerability to syphilis. In summary, we found that the vulnerability to syphilis among mostly young FSWs in Dimapur varied according to their sex work characteristics, marital and educational status and drug use habits. They may be more vulnerable to HIV and sexually transmitted infections (HIV/STIs) due to the low rate of condom use. The findings have direct implications for HIV/STI prevention programmes in Northeast India.
Keywords
Background
Due to its adverse clinical consequences as well as the possibility of prenatal transmission, syphilis is a sexually transmitted infection (STI) of epidemiological importance, especially as some infected people remain asymptomatic and therefore not seek treatment. If left untreated, syphilis can result in both short-term (e.g. genital lesions, lymphadenopathy and alopecia) and long-term (e.g. cardiovascular and neurological complications) morbidity. 1 Additionally, people with syphilis have an increased risk of acquiring and transmitting human immunodeficiency virus (HIV) infection. According to combined estimates positive syphilis serology is associated with 2.5-fold increased risk of HIV acquisition. 2
The prevalence of syphilis varies widely in India depending on the group tested. 3 Overall it has been reported that syphilis occurs more frequently in marginalized and vulnerable groups with limited access to STI testing and health facilities. 4
Female sex workers (FSWs) are a core risk group for infection with and transmission of STIs such as syphilis. Not only is this group at a higher risk of infection due to frequent exposure, they, along with their clients, are a ‘bridge group’ to the general population.5–6 Female sex work has a very long history in India and remains a largely clandestine activity. An unfavourable legal environment as well as discrimination faced by sex workers has resulted in variations in the practice of sex work. 7 Factors such as the organization and nature of sex work networks, and the place of solicitation and sex vary across the country. 7 While the characteristics of sex work in South India have been well reported in the literature,7–9 there are few studies describing the nature and practice of sex work in Northeast India. Understanding female sex work practice and factors related to the prevalence of STIs in the northeast is especially important considering the high prevalence of HIV reported from this region. According to the latest sentinel surveillance data collected in 2008, in Nagaland, HIV prevalence was 14.1% among FSWs and >1% among ante-natal clinic (ANC) attendees National AIDS Control Organization. HIV Sentinel Surveillance 2002–08, personal communication, July 2010.
There are an estimated 1800–3500 FSWs in Dimapur, 10 a commercial hub in the northeast state of Nagaland. In Dimapur, the FSWs do not work in brothel-based venues, but rather they work from hotels, ‘booze joints’ (illegal bars), at home and on the street. While there are known hotspots for sex-work, there is no ‘red light’ district as such. Consequently, these women remain a hidden and hard to reach population and have not yet been effectively mobilized as a community.
This paper presents analysis of data collected during the first round of the Integrated Biological and Behavioural Assessment (IBBA) survey among FSWs based in Dimapur in 2006. The objectives of the analysis are: (1) to describe the FSW population with regard to demographics, drug use, sex work characteristics, knowledge of STIs and reported STI symptoms in order to assess their vulnerability to syphilis; and (2) to identify factors associated with syphilis infection among the FSWs.
Methods
Study design
IBBA is a cross-sectional survey that collects both behavioural data via an interviewer-administered questionnaire and biological data from blood specimens that has been well-described elsewhere. 11
Sampling method
Respondent-driven sampling (RDS) was used to recruit FSWs from Dimapur, Nagaland. RDS builds on conventional snowball sampling and is a validated probability-based sampling method devised for use with hidden populations such as FSWs and injection drug users. 12 It is based on social network theory and utilizes FSW peer networks for the recruitment of participants and involves financial compensation to purposively recruited ‘seed’ participants who provide referral of other participants. A sample size of 400 was estimated for the study which is described elsewhere. 11
Data collection
Clearance for the IBBA survey was obtained from the Health Ministry Screening Committee (HMSC), Government of India. The study was also approved by the Ethical Committees of National AIDS Research Institute (NARI), Regional Medical Research Centre and Family Health International. 10 Written informed consent was obtained from each participant for administering the behaviour questionnaire as well as biological tests. The data were anonymized and behavioural and biological data were linked through study ID numbers.
To be eligible for participation in the study, FSWs needed to be 18 years of age or older, and have had sex with men in exchange for money at least once in the past one month. Participants responded to an extensive interviewer-administered questionnaire that gathered information on sociodemographics, drug use, sex work characteristics, condom use and knowledge of HIV.10,11
Venous blood and urine specimens were collected from all consenting participants. Standard operational guidelines were followed in carrying out all the laboratory procedures including sample collection, storage and transportation, processing, and testing of samples. The biological samples were tested for antibodies to HIV (Microlisa HIV, J. Mitra & Co. Pvt Ltd, New Delhi, India and the confirmatory test Genedia HIV 1/2 ELISA 3.0, by Greencross life Sciences Corp., Kyunggi-do, South Korea), syphilis (Rapid Plasma Reagin [RPR], Span Diagnostics Ltd, Surat, Gujarat, India and the confirmatory test Treponema pallidum Haemagglutination Assay [TPHA], Biokit, Barcelona, Spain). Neisseria gonorrhoeae and Chlamydia trachomatis infections were diagnosed by nucleic acid amplification tests (NAATs) (Gen Probe APTIMA Combo-2, Gen Probe Inc., San Diego, CA, USA).
Data analysis
Descriptive analysis was undertaken using RDSAT (version 6.0, Cornell University, Ithaca, NY, USA) to generate adjusted proportion estimates with 95% confidence intervals (CIs). This software package generates sample weights to take into account the variations in participants’ network sizes (degree weight) and differential recruitment and homophily (recruitment weight). Logistic regression analyses were conducted using STATA version 10.0 (Stata Corp., College Station, TX, USA) to estimate the strength of association between various FSW characteristics and the odds of testing positive for syphilis. The dependent variable was weighted with individualized weights generated by RDSAT 6.0. Crude and adjusted odds ratios (ORs) were calculated with their respective 95% CIs. The multivariate regression model was constructed to test the strength of associations; co-variates with unadjusted P values less than 0.1 were considered eligible for the multivariate model.
Results
A total of 426 FSWs participated in the study. The prevalences of syphilis and HIV among the participants were 21.1% and 11.7%, respectively. The prevalences of N. gonorrhoeae and C. trachomatis were 4.6% and 22.6%, respectively (data not shown). Approximately half of the participants were under 25 years of age, one-third were currently married and living with their husbands and about two-thirds of the participants were literate (Table 1).
Participant sociodemographic and sex work characteristics

Place of entertainment refers to the place where sexual services are provided and includes park, street, vehicles, cinema hall, bus stand, railway station, etc.
Among those who had regular non-paying male partners (n = 378). 95% CI = 95% confidence interval
One-fifth reported sexual debut before the age of 15 (Table 1). The majority of them had a regular (non-paying) male sexual partner. The most common place of solicitation was public places (32.7%), with the remainder spread evenly among bars/booze joints (23.8%), hotels/lodges (23.1%) and the home (20.3%). More than half (57.2%) reported that they entertained (i.e. provided sexual services) their clients in hotels/lodges, and the second most common place for entertaining clients was in the home (27.5%).
The percentage of FSWs using condoms during the last sex act with all types of partners was very low (occasional clients 36.5%; regular client 27%; regular non-paying partner 13.4%), and very few FSWs used condoms consistently (i.e. every time) with any type of sexual partner (Table 1). Approximately three-quarters (73.3%) had heard of STIs and the majority (88.2%) had heard about HIV (Table 2).
Knowledge of STIs/HIV and reported STI symptoms
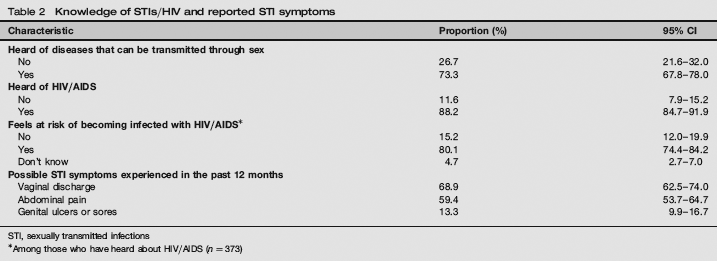
STI, sexually transmitted infections
Among those who have heard about HIV/AIDS (n = 373)
Logistic regression results for syphilis infection are presented in Table 3. The likelihood of being infected with syphilis was doubled for FSWs who were either currently married or were widowed/divorced/separated, compared with FSWs who had never been married. Those who were illiterate and those who had consumed drugs for non-medical purposes were approximately twice as likely to test positive for syphilis. Those FSWs who reported using a condom with their last occasional client were twice as likely to test positive for syphilis. Those FSWs who entertained their clients in bars and booze joints had approximately one-third the likelihood of testing positive for syphilis infection, compared with FSWs who entertained their clients in the home. In the additional subgroup analysis, FSWs who were ever married (i.e. either currently married or were widowed/divorced/separated), compared with the never married group, were significantly more likely to be older in age, illiterate and users of drugs. The average numbers of clients entertained in the last working week and average duration of sex work was also higher among ever married FSWs compared with never married (results not shown).
Predictors of testing positive for syphilis infection among FSWs in Nagaland
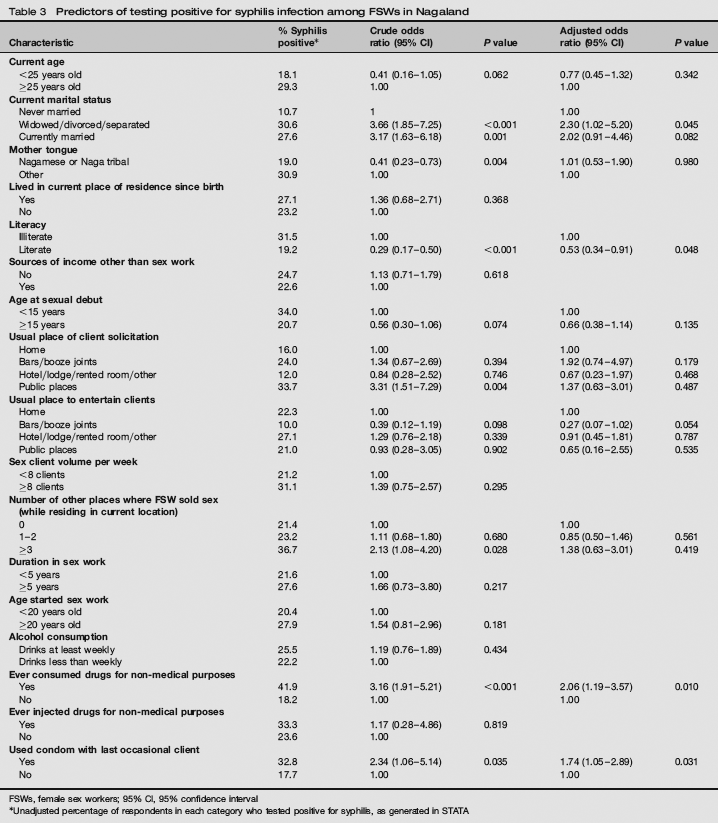
FSWs, female sex workers; 95% CI, 95% confidence interval
Unadjusted percentage of respondents in each category who tested positive for syphilis, as generated in STATA
Post hoc descriptive analysis was undertaken to further explore the finding that FSWs who entertained clients in bars and booze joints had lower odds of testing positive for syphilis, with an interest in the pattern of movement between place of solicitation and place of entertainment. Analysis revealed that among the sample of FSWs who usually entertained clients in bars and booze joints, a large majority (82.5%) also typically solicited their clients in bars and booze joints (presumably the same place). In contrast, 70.5% of FSWs who usually solicited clients in public places subsequently entertained them in hotels/lodges/rented rooms, and 51.0% of those who usually solicited in bars/booze joints entertained in hotels/lodges/rented rooms.
Table 4 presents unadjusted data on the prevalence of syphilis among various combinations of place of solicitation and place of entertainment. Syphilis prevalence was relatively lower for those FSWs who solicited in bars and booze joints and also entertained in bars and booze joints (12.1%), and for those who both solicited and entertained in hotels/lodges/rented rooms (13.3%). However, the prevalence of syphilis was relatively high among those who usually solicited in public places and then entertained in hotels/lodges/rented rooms (38.5%) or the home (26.5%), and among those who solicited in bar/booze joints and then entertained in hotels/lodges/rented rooms (26.5%).
Prevalence of syphilis infection, by place of solicitation and place of entertainment
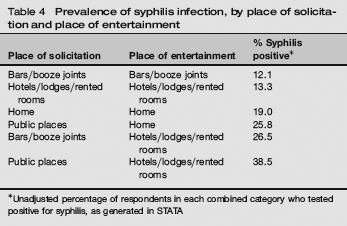
Unadjusted percentage of respondents in each combined category who tested positive for syphilis, as generated in STATA
Discussion
These sample of FSWs from Dimapur, Nagaland were found to have a high prevalence of STIs, especially syphilis (22.1%) amplifying the risk of subsequent HIV infection compared with other states.
Even though the majority of FSWs had heard of STIs and HIV, and perceived themselves to be at risk of infection, they reported very low levels of condom use with all types of sexual partners. The use of condoms at last sex was substantially lower than among FSWs in other parts of India.10,13 While the lack of condom use with regular non-paying partners can in part be understood as a desire for greater intimacy with a partner, 14 the low level of condom usage with both occasional and regular clients raises concerns regarding risk perception and/or difficulties in negotiating the use of condoms. Moreover, the sizeable proportion of FSWs reporting STI symptoms, higher than that reported by FSWs in other parts of India,8–13 appears consistent with the low level of condom use.
More than half the FSWs were under 25 years of age, compared with IBBA findings from the southern states of India where just 18% of FSWs were under the age of 25. 9 Additionally, one-fifth had an early age of sexual debut (i.e. before the age of 15) and more than half were less than 20 years of age when they first entered sex work. Many of these women are entering sex work during their adolescent years and this raises substantial policy and programming challenges, some of which may be sensitive in this very conservative context. These findings indicate the need for existing programmes to adopt a youth and equity lens, 15 to ensure that the sexual and reproductive health services are ‘youth-friendly’, i.e. they engage with and respond to the information and treatment needs of young people.
For many women selling sex in Dimapur, sex work is the only source of income. These findings echo those of previous research on pathways into sex work among FSWs in Dimapur 16 which highlight that the most common pathway to sex work was the economic pathway. Many FSWs were entering sex work due to financial insecurity. As pointed out by Devine et al., 16 there is a need to focus on strategies that support opportunities for FSWs to transition out of sex work.
Syphilis infection was more likely among FSWs with a history of consuming drugs for non-medical purposes. Previous research has also found similar independent associations between drug use and both sexual risk behaviours and STI infection.17,18 FSWs who consume illicit drugs, particularly while soliciting clients, are more likely to take greater risks and have a reduced capacity to negotiate safe sex practices with clients. FSWs in Dimapur who have entered sex work to earn money to support their drug habit are at increased vulnerability to STIs. 16 Their need for drugs possibly outweighs their need to protect themselves from infection. Our findings suggest the need for existing harm reduction programmes to emphasize the importance of STI testing and treatment.
Having a current partner, or being widowed or separated, increased the likelihood of syphilis infection among FSWs in Dimapur. This finding is likely to be influenced by several factors. The greater vulnerability to syphilis infection among ever married, compared with never married group could be linked to unprotected sex with their regular non-paying partners, as opposed to clients, given that the rate of consistent condom use with regular partners was even lower than that with clients, particularly occasional clients. The higher rate of drug use among married FSWs may also partially explain their greater vulnerability to syphilis and other STIs. 17 Women with a current partner may be financially supporting both themselves and their partner, who may have a drug habit, resulting in the need to entertain an increased number of clients and take greater risks (e.g. higher payments for sex without condoms) to gain sufficient income to support themselves. The findings of subgroup analysis in fact suggest that average number of clients entertained by the married group was significantly higher in the last working week compared with never married FSWs. Because of their relatively older age and longer duration in sex work, FSWs who were currently married or widowed/separated may have also been more vulnerable to acquire STIs due to longer duration of exposure than never married FSWs. Finally, the social, economic and STI vulnerability of women who are widowed or divorced in Indian society is widely recognized,9,19 but programmes rarely target this group specifically. However, further in depth studies should be carried out to better explain the STI-related vulnerability in relation to marital status among FSWs in this region.
Those FSWs who were illiterate had a greater likelihood of testing positive for syphilis infection. This result is consistent with findings from a previous study in China on predictors of syphilis, which reported that FSWs with less education are at a greater risk of infection. 20 Being illiterate is a plausible risk factor for a number of reasons including increased socioeconomic vulnerability, less access to knowledge about STIs (and STI prevention) and potentially a lower capacity to negotiate safe sex practices with clients.
Those FSWs who usually entertain their clients in bars and booze joints were less likely to be infected with syphilis compared with those FSWs who typically entertained at home. Several studies have highlighted the relationship between STI vulnerability for sex workers and the place where they solicit and entertain (have sex with) their clients.8,9,21 In Dimapur, there is a pattern of movement for some FSWs who move from soliciting in public places and bars/booze joints to entertaining in hotels/lodges and their home. Our post hoc analysis highlights that those FSWs who solicit and entertain in bars and booze joints, or solicit and entertain at hotels/lodges, are the least vulnerable to syphilis infection. Those FSWs who solicit clients in public places, bars or booze joints and then move to hotels/lodges for sex are the group most vulnerable to syphilis infection, followed by those who move from soliciting in public places to entertaining in their home. Another study in Karnataka, South India similarly identified FSWs who solicited in the street and then moved to a lodge for sex as being more likely to be infected with HIV and syphilis. 8 Further qualitative research is needed to explore this dynamic further; for instance, to examine whether it is the process of moving location that creates vulnerability or whether moving locations is an act undertaken by FSWs who are more vulnerable to syphilis infection for a variety of other reasons.
We observed that FSWs who reported using condoms with their last occasional client had a greater likelihood of testing positive for syphilis. This unexpected result may be because of our cross-sectional nature of the study. This might be possible that they were infected before they began to use condoms. The cross-sectional nature of this study means that we are only getting information from respondents at one point in time. If we followed a cohort over time we would expect to find that the use of condoms would be a protective factor against acquisition of syphilis infection.
Our findings are subject to several limitations. The use of RDS methods contains limitations for multivariate analysis; guidelines for multivariate analysis of RDS data are still under development and require further validation. Despite this limitation, RDS proves effective in producing probability-based estimates of the prevalence of STIs and various FSW characteristics. Individual recollection and reporting of behaviour may have been influenced by recall and social desirability bias, whereby less socially desirable behaviours may be under-reported leading to potential underestimation of associations between these behaviours and syphilis infection. As with all cross-sectional study designs causal relationships cannot be proven due to the difficulty in determining the temporal relationship between the predictors and the outcomes. However, the multivariate analysis in this paper highlights significant correlates of syphilis infection among FSWs that have important programming implications and improves our understanding of STIs in this high-risk group.
In summary, FSWs in Dimapur are a young population, many of whom have no other form of income outside selling sex. The worryingly low rates of condom use combined with high prevalence of STIs including syphilis, indicate that FSWs in Dimapur are vulnerable to an escalating HIV epidemic, and alludes to the important contribution that sexual transmission could possibly be making to the HIV epidemic in Nagaland. We found that FSWs who were married (or had a history of marriage), illiterate, or had consumed illicit drugs were more likely to test positive for syphilis infection, as were FSWs who moved between soliciting in public places or bars/booze joints and entertaining in hotels/lodges. Investigation of these themes will have direct implications for STI/HIV prevention policies and programmes in this complex region of Northeast India.
Footnotes
Acknowledgement
We are grateful to Dr Michelle Kermode who read over the final manuscript and provided comments on the interpretation of the analysis.