
Abstract
Negotiation for condom use by female sex workers with their male clients can enhance condom use. A cross-sectional study was conducted among 1395 female sex workers; 439 from two brothels, 442 from 30 hotels, and 514 from streets of two cities in Bangladesh to determine the predictors of condom use negotiation. Consistent condom use rates in the 7 days prior to interview were reported to be 16.2%, 21.7%, and 4.5% among the brothel, hotel, and street-based female sex workers, respectively. Overall, 28.1% of female sex workers negotiated for condom use with their clients. Participation in behaviour change communication (BCC) programmes (AOR, 1.5; 95% CI, 1.2–2.0) and self-perceived risk of human immunodeficiency virus infection (AOR, 1.8 95% CI, 1.6–2.1) were positive predictors for condom negotiation. Compared to the hotel-based female sex workers, street (AOR, 0.6; 95% CI, 0.4–0.9) and brothel-based female sex workers (AOR, 0.7; 95% CI, 0.5–0.9) were less likely to negotiate for condom use. Female sex workers in Bangladesh are at high risk for sexually transmitted infection / human immunodeficiency virus infection because of low overall negotiation for condom use. Participation in BCC programmes had positive effect on condom negotiation by female sex workers, and should be strengthened in commercial sex venues.
Keywords
Introduction
Female sex workers (FSWs) are vulnerable to human immunodeficiency virus (HIV) infection and sexually transmitted infections (STIs) because of frequent unprotected sex acts with multiple partners.1–3 Commercial sex takes different forms in South and Southeast Asian countries based on the venues where FSWs entertain their clients such as in brothels, hotels, rented apartments, streets, bars, and beauty salons.4,5 Similarly, in Bangladesh, FSWs are broadly categorized as street-based, brothel-based, hotel/residence-based although it has been well documented that FSWs often exchange their venues.6,7 In Bangladesh, prevalence of HIV among FSWs is still below 1%, but risk behaviours such as low condom use, high client turn over, and high rates of other STIs make them vulnerable to HIV.7,8 National serological surveillance and other special studies among FSWs confirm high prevalence of STIs among FSWs in Bangladesh ranging from 8% to 64% for syphilis, gonorrhoea, chlamydia, and herpes simplex virus 2 (HSV2).9,10 According to the latest round of Bangladesh Behavioural Surveillance Survey (2006–07), 13% and 28% of the brothel- and hotel-based FSWs used condom consistently with their regular clients, respectively.7,11,12
Globally an accepted strategy to enhance condom use in commercial sex is to improve the skills of FSWs in condom use negotiation with their male clients. Condom use self‐efficacy and confidence in negotiation with clients have been found to enhance consistent condom use among FSWs.7,13,14 Initiation of condom use by FSWs themselves and improving their ability to refuse clients who do not want to use condoms are critical steps for condom use negotiation. On the other hand, condom use negotiation by FSWs is negatively influenced by a range of factors including poverty, inequitable power structures in the commercial sex settings, restrictive laws, gender dynamics, and other socio-cultural factors. 13 Harassment and violence faced by FSWs from clients, law enforcement agencies, and power structures is a key factor that deters condom use negotiation.7,15 Law enforcement personnel often consider possession of condoms to be grounds for arrest and harassment of FSWs; this diminishes the likelihood of FSWs to carry condoms, a necessary step towards successful condom negotiation.16,17
In Bangladesh, several studies have highlighted the factors associated with condom use in commercial sex. Qualitative studies describe various issues related to cultural beliefs and norms as well as pleasure. 18 Secondary analysis of existing data has shown that facilitating factors for condom use among clients of FSWs include requesting clients to use condoms, availability of condoms, better knowledge on HIV prevention, while deterring factors include multiple sex partners and forced sex. 7 However, none of these studies have investigated condom negotiation directly as they did not document the extent to which FSWs negotiate for condom use with their partners or the factors that determine condom use negotiation. This study addresses this gap as it measures the level of condom use negotiation by hotel-, street-, and brothel-based FSWs in Bangladesh and identifies the factors that influence condom use negotiation. The results can help to guide HIV prevention interventions in order to increase condom use by FSWs.
Methodology
This project is part of a larger cross-sectional study that was conducted in 2006 among FSWs from selected brothels, hotels, and streets in Bangladesh and their clients to understand barriers of condom use in commercial sex settings. Street- and hotel-based FSWs were recruited in this study from Dhaka and Chittagong city corporation area, the two major cities in Bangladesh. Brothel-based FSWs were recruited from Daulatdia and Tangail, the two largest brothels in Bangladesh. The study subjects were selected using multi-stage sampling technique for brothels, hotels, and streets as appropriate.
For brothels, a mapping exercise was done to enumerate the number of rooms and number of FSWs in each room. Each brothel in the two areas was divided into segments of 30 rooms resulting in 27 segments in Tangail and 23 in Daulatdia. Fifteen segments were randomly selected from Tangail and Daulatdia. There were 40 FSWs per segment on an average; 15 from each segment were randomly selected for recruitment in the study. For street-based FSWs, 81 cruising spots where at least five FSWs gathered per day on an average of 3 consecutive days were identified with 54 in Dhaka and 27 in Chittagong metropolitan city. From this list, 30 cruising spots were selected by simple random sampling method and FSWs were recruited in each selected cruising spot using probability proportional to size (PPS) method. For identification of hotel-based sex workers, residential hotels in Dhaka and Chittagong city corporation area were listed if they had at least five FSWs available every day for the last 7 days. From the list of 74 such hotels in Dhaka and 7 in Chittagong, 30 hotels were selected by simple random sampling method and FSWs were randomly sampled and recruited in each selected hotel using PPS method. Sample size was calculated separately for each of the different types of FSWs using the variable ‘major reasons for not using condoms in last sex.’ The sample sizes were calculated to be 487, 520, and 487 for brothel-, hotel-, and street-based FSWs, respectively.
Data collection was done by trained female interviewers using a structured questionnaire adapted for the three types of FSWs. The questionnaire was pilot tested and translated in local language for final administration. In addition to asking questions on socio-demographic characteristics, STI/HIV knowledge, and sexual behaviour, information on condom use for different types of sexual acts (e.g. vaginal, anal, oral) with both new and regular clients were collected. The study was approved by the Ethical Review Committee (ERC) of the International Centre for Diarrhoeal Diseases Research, Bangladesh (icddr,b).
Data were entered in Fox-pro database system (Microsoft Visual FoxPro 6.0, Microsoft Press Redmond, Wash. Microsoft Press, ©1998); any discrepancies were resolved by checking the hard copy questionnaire. Comparisons were made for socio-demographic, sexual behaviour, and condom use–related information among the three types of FSWs. To examine crude associations, chi square test was used for categorical data and Student’s t-test was used for continuous variables. We used two variables to define ‘condom negotiation’: (1) whether an FSW herself initiated dialogue and her client agreed to use a condom in last sex act and (2) whether an FSW refused any client in last 6 months of interview for not being willing to use condoms. We categorized ‘condom negotiation’ as ‘no,’ ‘partial,’ and ‘full.’ ‘No condom negotiation’ was determined if FSWs neither initiated condom use nor refused any clients in the previous 6 months for not using condoms, ‘partial condom negotiation’ was determined if FSWs reported ‘Yes’ to either of the two questions, and ‘full condom negotiation’ was determined if FSWs reported ‘Yes’ to both questions. In order to accommodate the ordinal nature of the computed outcome variable, we used bivariate and multivariate cumulative logit model to evaluate the factors associated with condom negotiation. In the multivariate model, we included the variables with p value ≤ 0.1 in bivariate regression model. p Value ≤ 0.05 was considered as statistically significant for all two-sided tests. We checked the test of parallel lines to assess the proportional odds assumption of ordinal regression model. We used SPSS (version 15.0, SPSS, Inc., Chicago, Illinois) for all statistical analyses.
Results
Of the total 1418 FSWs approached, 1395 completed the interview after providing verbal informed consent; 439, 442, and 514 FSWs from brothel, hotel, and street settings, respectively. Data collection could not be completed for 23 FSWs because they were unwilling to respond to some of the questions, or they had clients arrive at that time and were not available afterwards.
Socio-demographic and other characteristics by three different types of sex workers.

FSW: female sex worker; HIV: human immunodeficiency virus; STI: sexually transmitted infection.
Knowledge is based on key questions including knowledge about HIV transmission, HIV prevention, and symptoms of common STIs other than HIV.
Violence included physical beating, rape, not paying money after having sex.
Illicit substances including alcohol and cannabis.
Sexual and condom use behaviours by three different types of sex workers.
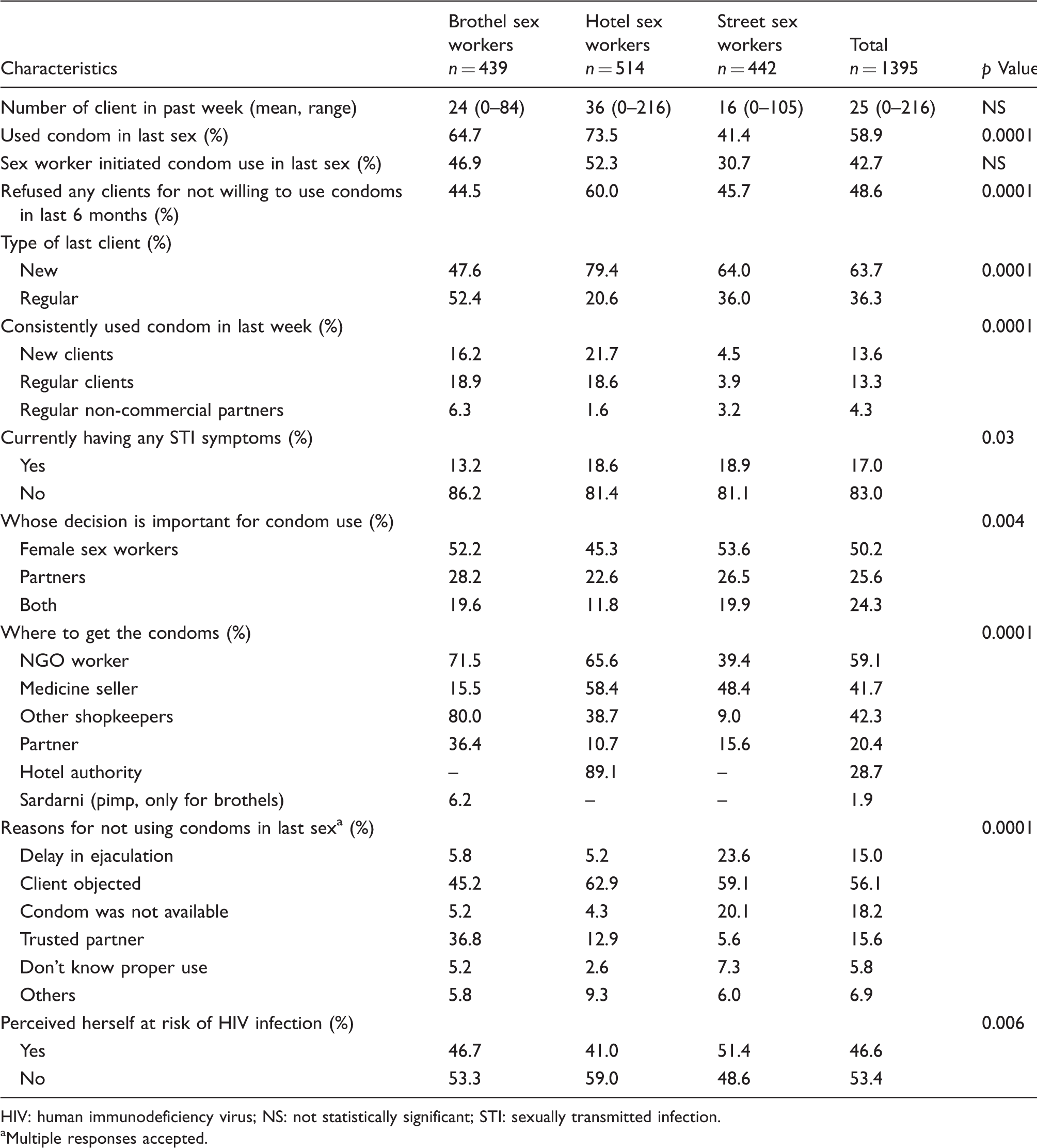
HIV: human immunodeficiency virus; NS: not statistically significant; STI: sexually transmitted infection.
Multiple responses accepted.
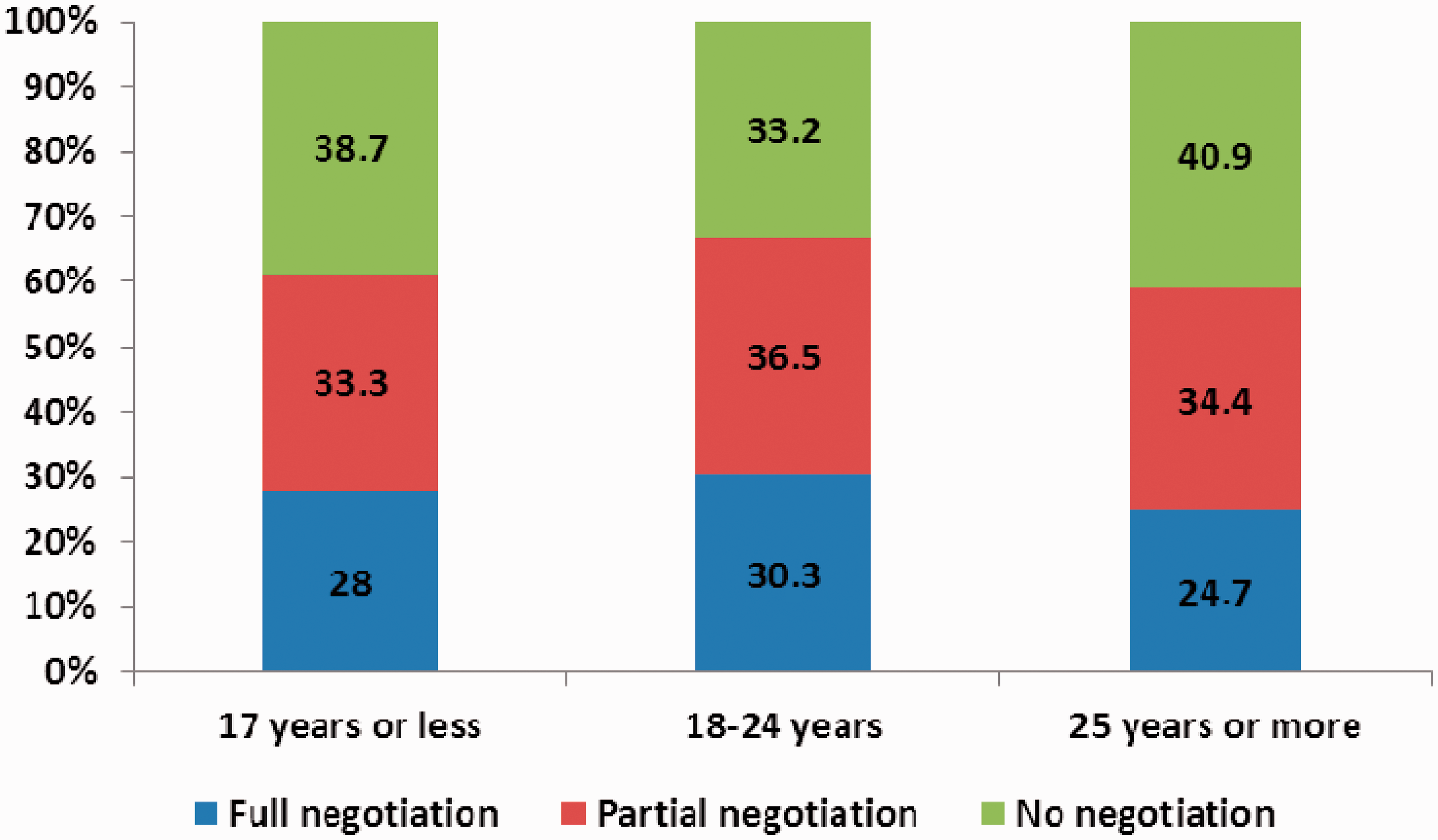
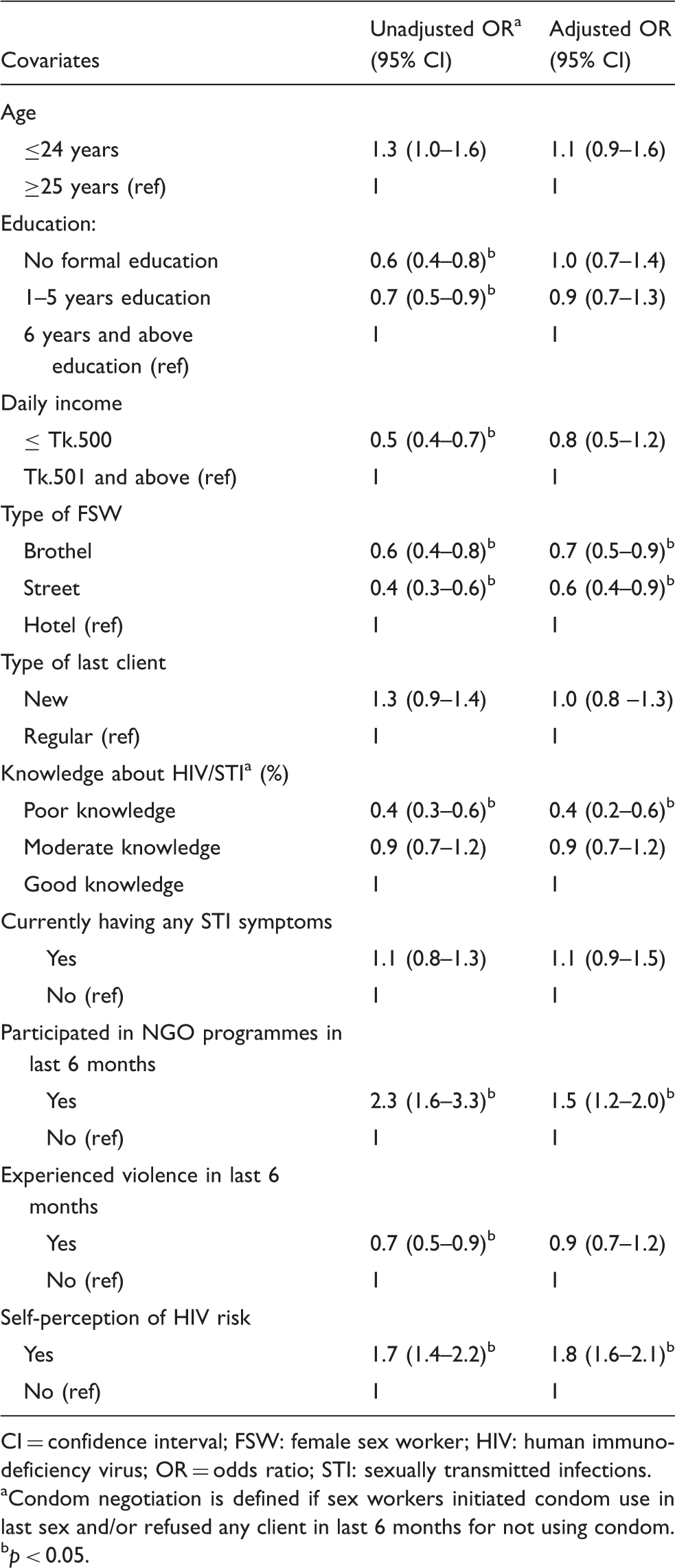
Of all FSWs, 28.1% had ‘full negotiation’ and another 35.2% had ‘partial negotiation’ (Figure 1). Fewer street-based FSWs reported full negotiation for condom use (22.1%) compared to hotel- (36.9%) and brothel (26.1%)-based FSWs. Figure 2 shows that 28.0% FSWs of age 13–17 years had ‘full negotiation’ for condom use compared to 30.3% of age 18–24 years and 24.7% of age 25 years and above, but these differences were not statistically significant. In bivariate cumulative logit models, negotiation for condom use was significantly associated with literacy, income, type of FSW, knowledge about HIV/AIDS, participation in NGO-operated education sessions, past experience of harassment, and HIV risk perception. In the multivariate model, negotiation for condom use was significantly associated with type of FSW, knowledge about HIV/AIDS, participation in NGO-led behaviour change communication (BCC) programmes, and risk perception for HIV/AIDS (Table 3). Street-based FSWs (OR 0.6, 95% CI 0.4–0.9), brothel-based FSWs (OR 0.7, 95% CI 0.5–0.9), and FSW with poor knowledge of HIV/AIDS (OR 0.4, 95% CI 0.2–0.6) were significantly less likely to negotiate for condom use compared to the hotel-based FSWs. On the other hand, FSWs who reported participation in any NGO-led BCC programmes (OR 1.5, 95% CI 1.2–2.0) and those who reported considering themselves to be at risk for HIV infection (OR 1.8, 95% CI 1.6–2.1) were significantly more likely to negotiate for condom use with their clients.
Condom negotiation by types of female sex workers. Condom negotiation by age group showing below 18 years group. Multivariate ordinal logistic regression analysis to understand determinants of condom negotiation among sex workers in Bangladesh. CI = confidence interval; FSW: female sex worker; HIV: human immunodeficiency virus; OR = odds ratio; STI: sexually transmitted infections. Condom negotiation is defined if sex workers initiated condom use in last sex and/or refused any client in last 6 months for not using condom. p < 0.05.
Discussion
This study highlights that negotiating for condom use was low among all the FSWs, while street-based FSWs were less likely to negotiate for condoms compared to hotel- and brothel-based FSWs. The study also shows that participation in NGO-led BCC programmes helped the FSWs to negotiate better for condom use with their clients.
The current didactic approach to encouraging condom use is unlikely to enhance FSWs’ ability to negotiate with clients because negotiation of condom use is influenced by a range of factors including economic vulnerability of FSWs, their negotiation skills, gender, and power relations.19,20 Some of these factors may be improved by involving FSWs in intervention programmes that provide them more knowledge about STI/HIV/AIDS and better skills to negotiate for condoms with their clients.21,22 However, for others factors, such as underlying gender and power-related issues, interventions need to take into account the societal and contextual reality that determines the vulnerability of FSWs.18,19 This study showed that client’s objection was the leading reason for not using condoms and was reported consistently across the three different groups of FSWs. The clients who are not willing to use condoms often offer more money for not using a condom or become violent towards the FSWs. Earlier studies have shown that the client’s objection to condom use is often related to the perceived belief that condoms reduce sexual pleasure or sometimes it is grounded in deeper issues related to gender and ideas about masculinity.18,23 Thus, rather than focusing solely on FSWs’ individual knowledge and attributes, it is important to contextualize safer sex promotion efforts within FSWs’ ground reality.
It is important for interventions to recognize the differences in negotiation ability and practice across the different types of FSWs. Street-based FSWs were less likely to negotiate for condom use with their clients compared to other types of FSWs, which may be correlated with their lower income, lower literacy, less knowledge about STI/HIV/AIDS, and the fact that street-based FSWs are more exposed to violence in their workplace compared to other types of FSWs. Providing skills for alternative income generation is a recognized intervention for sex workers to improve their status and negotiation for safer sex.24,25 In Bangladesh, many programmes offer alternate income generation activities but few of them have demonstrated the desired outcomes. One challenge for these programmes is that the earnings from alternative sources, especially for younger FSWs, are much lower than from selling sex. Well-designed prospective studies with realistic alternatives of livelihood options should be introduced, along with strong evaluation components to demonstrate the role of alternative income generation on improving FSW’s status in Bangladesh. To increase condom use negotiation, sex workers also need the support of the power structure in which they operate.
This study underscores that participation in NGO-run BCC programmes helped the FSWs to negotiate better for condom use with their clients. NGO-run BCC programmes contribute to increasing knowledge on HIV/STI transmission and prevention, learning negotiation skills, and gaining confidence that condom use is a socially deserving behaviour. 26 NGOs and community-based organizations (CBOs) also help FSWs to organize themselves by forming self-help groups as a means of empowering them to negotiate for condom use with their clients 27 and also facilitate FSWs to share their feelings, thoughts, and experiences regarding condom use with fellow FSWs. Most of the NGO-run interventions in Bangladesh work with group counselling sessions to increase knowledge and awareness about STI/HIV infection and prevention, improving skills on condom use, and more importantly, improving distribution and availability of condoms at sex work venues to promote condom use and negotiation by the FSWs.
FSWs aged 13–17 years were recruited in this study to understand sexual risk behaviours and other vulnerabilities. Several studies in Asia reported that teenaged FSWs pose high levels of risky behaviour in terms of HIV/STI.28,29 Initially, the ERC of icddr,b expressed a strong preference to limit the age group of study participants to 18 years and above. However, after discussion, the ERC was convinced that in employing this inclusion criterion, we would miss the large number of FSWs who are below the age of 18 years. The ERC also agreed that collection of information on risk behaviours among these FSWs would have important programmatic implications. The option of taking parental assent was dropped considering that the parents may be ignorant of those FSW’s involvement in selling sex. We did not find any significant difference in condom use negotiation among FSWs in this group compared to the older groups unlike the studies reported from Philippines and Thailand.28,29
Several limitations of the study should be taken into account. First, self-reported information collected from FSWs in this cross-sectional survey may suffer from social desirability bias to report favourably for condom negotiation and that we did not collect any biological data to report STI/HIV status to correlate with condom negotiation practices. Second, the study was conducted in two selected brothels and two major cities in Bangladesh for street-based and hotel-based FSWs, thus the findings may not be generalisable. However, we recruited FSWs randomly within their categories, thus improving the potential to generalize the findings to other FSWs in Bangladesh. Third, our condom negotiation outcome relied on two indicators, whether FSW initiated condom use herself during last sex and whether an FSW refused any client for not being willing to use condoms in the last 6 months. While these two indicators are most vital, other elements of condom use negotiation, including steps taken to resist client’s pressure not to use condoms and possession of condoms, may have better explained condom use negotiation as used in another study to define condom negotiation. 30
Based on the findings from this study, we conclude that FSWs in Bangladesh are at higher risk for STI/HIV because of low consistent condom use and overall low negotiation for condom use. As expected, low-income FSWs including those who are street-based are less likely to negotiate with their clients for condom use. Exposure to behaviour change intervention had a positive impact on FSWs to better negotiate for condom use with their clients. We recommend that behaviour change interventions with particular focus on improving condom use negotiation skills should be strengthened to cover all types of FSWs, especially street-based FSWs.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research project was funded by Australian Agency for International Development (AusAID). Nazmul Alam is supported by NIH Research Training Grant # D43 TW001035 funded by the Fogarty International Center, the National Institute on Drug Abuse, and the Office of Research on Women's Health and Santé-CAP, a strategic training programme in Global Health Research, a partnership of the Canadian Institutes of Health Research (CIHR) and the Québec Population Health Research Network (QPHRN). icddr,b acknowledges with gratitude the commitment of AusAID, NIH, and CIHR to its research efforts.