
Abstract
Summary
Herpes simplex virus type 2 (HSV-2) can contribute to the spread of HIV. From March 2006 to November 2009, female sex workers (FSWs) in Yunnan, China were recruited into an open cohort study to determine incidence and risk factors for HSV-2 acquisition. Participants were interviewed and tested for HSV-2 and other sexually transmitted infections (STIs) every six months. A multivariate Cox proportional hazards regression model with time-dependent variables was used to measure associations with HSV-2 acquisition. In 3.5 years, 83 incident cases of HSV-2 infection were diagnosed, yielding an overall incidence of 21.9 per 100 person years (PY) (95% confidence interval [CI], 17.8–26.3). Working in higher risk commercial sex venues, current Neisseria gonorrhoeae infection, age of sexual debut <18 years and lack of a regular sex partner were independent factors associated with HSV-2 acquisition. The high incidence of HSV-2 suggests that prevention methods for HIV/STI control are urgently needed.
Keywords
INTRODUCTION
Herpes simplex virus type 2 (HSV-2) is one of the most common sexually transmitted infections (STIs) and the most frequent cause of genital ulcers. 1,2 Sexual transmission has become the primary mode of HIV transmission in China. 3 HSV-2 may contribute substantially to the spread of HIV since HSV-2 infection has been associated with increased risk for HIV infection. 4 –8
In China, HIV prevalence is highest in Yunnan Province, an area in close proximity to the major drug trafficking routes of the Golden Triangle, near the borders with Vietnam, Thailand and Myanmar. 9 Since the beginning of the epidemic, sexual transmission has played an increasingly greater role in this region. 10 Female sex workers (FSWs), who are not only at high risk for HIV infection, but also a core group for secondary transmission to general population along with their clients, 11,12 may be responsible for a large proportion of HIV transmission in China. 3 Of the estimated 780,000 people living with HIV/AIDS in 2011, 46.5% were infected through heterosexual transmission; of those infected through heterosexual transmission, approximately two-thirds were infected through non-spousal transmission. 3 HSV-2 seroprevalence rates as high as 65–70% have been observed among Yunnan FSWs; 13,14 however, there are limited data about HSV-2 incidence and associated risk factors. The aim of this study was to determine the incidence and risk factors for HSV-2 acquisition among FSWs in Yunnan Province, China. This study was conducted in Kaiyuan City, Yunnan, a moderately-sized city with a population of 292,000 and large numbers of sex workers. 15
METHODS
Study participants
From March 2006 to November 2009, cross-sectional studies were conducted biannually (8 surveys total) in Kaiyuan City, Yunnan Province by the Chinese Center for Disease Control and Prevention (China CDC) with provincial and local staff. Local CDC outreach workers recruited potential study subjects directly at sex work venues and through venue-owner outreach. Outreach workers explained the study purpose, procedures, and the risks and benefits of participation. The inclusion criteria were women aged ≥16 years, self-reported to have sold sex for money within the previous three months, willing to provide written informed consent, and agreed to be tested and counselled for HIV and STIs. All women who met the inclusion criteria were invited to participate in the research study and were compensated 50 RMB ($8 USD) upon each survey completion. This study received approval from both the China CDC National Center for AIDS/STD (NCAIDS) and the Yunnan Provincial CDC institutional review boards.
Data collection
Specialists from the China CDC and the Yunnan Provincial CDC trained local staff members from the Kaiyuan CDC on the protection of human subjects, obtaining informed consent, safeguarding confidentiality, and HIV/STI pre- and post-test counselling.
After providing written informed consent, participants were asked a series of questions regarding their demographics, basic medical history, alcohol use and sexual and illegal drug use behaviour (including history of illegal drug use, types of illegal drugs used, illegal drug use methods, duration of illegal drug use and needle sharing). In order to maximize participant retention, the study schedule was thoroughly explained and was re-emphasized at subsequent follow-up surveys and attempts were made to contact all study participants through provided contact information which was collected and confirmed at each study visit one month in advance to remind them to return for follow-up surveys.
Blood was collected and tested for HSV-2 antibodies (HSV-2, HerpeSelect-2 ELISA IgG, Focus Diagnostics, Cypress, CA, USA), HIV-1 antibodies (enzyme-linked immunosorbent assay [ELISA], Vironostika HIV Uni-Form plus O, bioMerieux, Boxtel, Holland) and syphilis (rapid plasma reagin [RPR] test, Diagnosis Kit, Xindi Company, Urumqi, Xinjiang, China). Positive HIV-1 ELISAs were confirmed by Western blot (Diagnostics HIV Blot 2.2, Genelabs, Redwood City, CA, USA) and positive RPR tests for syphilis were confirmed by the Treponema pallidum particle assay (TPPA) test (Serodia-P PA-Fujirebio, Fuji, Tokyo, Japan). Endocervical swabs were collected and tested for Neisseria gonorrhoeae and Chlamydia trachomatis by polymerase chain reaction (PCR, AMPLICOR, Roche, Indianapolis, IN, USA). Vaginal swabs were collected and a wet mount was prepared to detect Trichomonas vaginalis (TV). Urine was collected for opiate screening (MOP One Step Opiate Test Device, ACON Laboratories, Inc., San Diego, CA, USA). Participants were classified as using illegal drugs if they self-reported ever illegal drug use or tested positive for opiates through urine screening; illegal drug users who self-reported ever injecting illegal drug were classified as injection drug users (IDUs), otherwise they were classified as non-injection illegal drug users. The determination of alcohol use was based on self-report, and subjects who reported alcohol consumption in past six months were classified as drinking alcohol.
Subjects were scheduled for follow-up visits 4–6 weeks after the initial visit to receive test results and post-test counselling. FSW participants with STIs were referred to the Kaiyuan Dermatology Hospital, where participants were entitled to receive a 60% discount on STI treatment. Those who tested HIV-positive were referred to the Kaiyuan People's Hospital, where antiretroviral therapy was offered (when applicable) through the support of the Clinton Foundation. Special efforts were made to contact and notify all subjects who tested positive for HIV and STIs, but did not return at the 4–6 week follow-up by calling these FSWs or going to their work location using the contact information provided during the study by the participant.
Statistical analysis
Statistical tests were performed using SAS 9.1 software (SAS Institute Inc., Cary, NC, USA). Those who were HSV-2 positive at baseline were excluded from the analysis, and subjects who were initially HSV-2 negative and completed two or more surveys constituted an open cohort. Chi-square tests were used to compare demographic and behavioural characteristics of participants who returned for follow-up and subjects who did not return. HSV-2 incidence density was calculated for subjects with an initial HSV-2 seronegative result who completed at least two surveys, dividing the number of events of HSV-2 seroconversion by the number of person years of follow-up. The follow-up time for each FSW was calculated as the time between her first negative HSV-2 test and the most recent negative HSV-2 test or incident HSV-2 infection if she seroconverted. Overall incidence density was calculated with 95% confidence intervals (CI).
The exact date of seroconversion was unknown, so the probability of seroconversion was assumed to occur uniformly along the interval between the date of last HSV-2 negative test and the first HSV-2 positive test. HSV-2 infection was not assumed to take place on the midway of the interval, which may produce artificial fluctuations as many of these intervals were quite long. For subjects who seroconverted, the contribution of person-years to the denominator was proportional to the amount of time remaining until the end of that interval. 16
Univariate Cox proportional hazards regression models with time-dependent variables were used to measure the associations between independent variables and HSV-2 acquisition. Factors that could change during follow-up were treated as time-dependent variables. Characteristics, such as education level, nationality and age at initiation of sex work, were treated as time-independent variables. Factors that were significantly associated in univariate analysis or risk factors identified in previous research (such as condom use and number of clients) were included in a stepwise Cox proportional hazards multiple regression model with entry criteria of P < 0.2 and exit criteria of P > 0.05.
Higher risk venues were defined as locations where FSWs generally charge less than 100 RMB (about $16 USD) per sexual service, including beauty salons, temporary sublets and streets. Lower risk venues were defined as locations where FSWs generally charged 100 RMB or more per sexual service, including karaoke clubs, nightclubs, saunas and hotels.
RESULTS
Characteristics of study participants
By the end of the eighth survey in November 2009, there were 2282 FSWs cumulatively recruited in the study cohort. A total of 853 (37.4%) participants were HSV-2 negative at baseline and of these 853 participants, 334 (39.2%) FSWs returned for at least one follow-up visit.
Comparison of demographic and behavioural characteristics of FSWs in the cohort and lost to follow-up
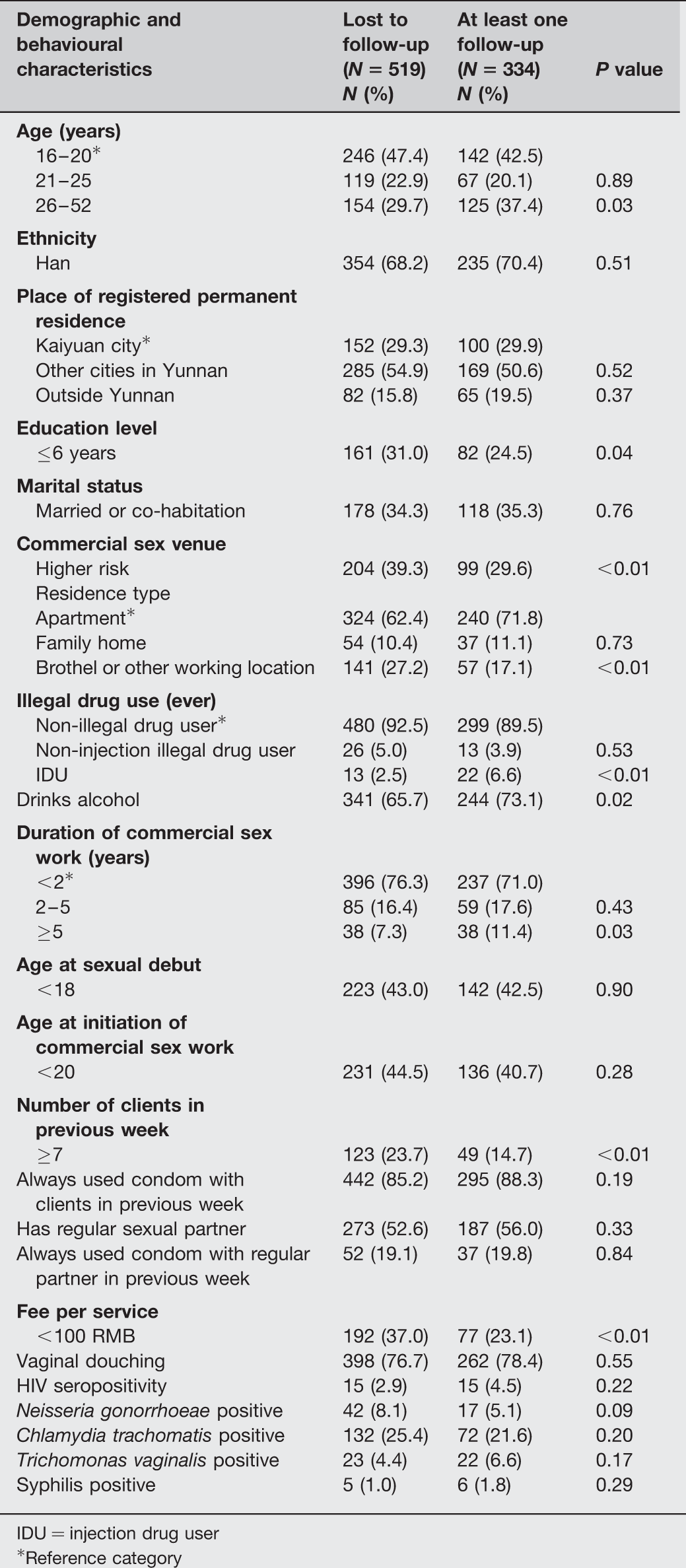
IDU = injection drug user
*Reference category
For those who were retained in the cohort, the majority were of Han ethnicity (70.4%), had registered residence in other cities in Yunnan (50.6%), worked out of low-risk commercial sex venues (70.4%) and reported that they had always used condoms with the previous week's clients (88.3%). Although reported condom use was high, STI prevalence was also high: 4.5% were HIV seropositive, 5.1% were N. gonorrhoeae positive, 21.6% were C. trachomatis positive, 6.6% were TV positive and 1.8% were syphilis positive.
HSV-2 incidence and associated risk factors
The mean duration of follow-up for those 334 FSWs who were HSV-2 negative at enrollment and returned for at least one follow-up visit was 1.14 ± 0.39 years. During the three and a half years of the study, 83 incident cases of HSV-2 infection were diagnosed, yielding an overall incidence 21.9 per 100 person years (PY) (95% CI: 17.8–26.3).
Factors associated with HSV-2 incidence in univariate analysis
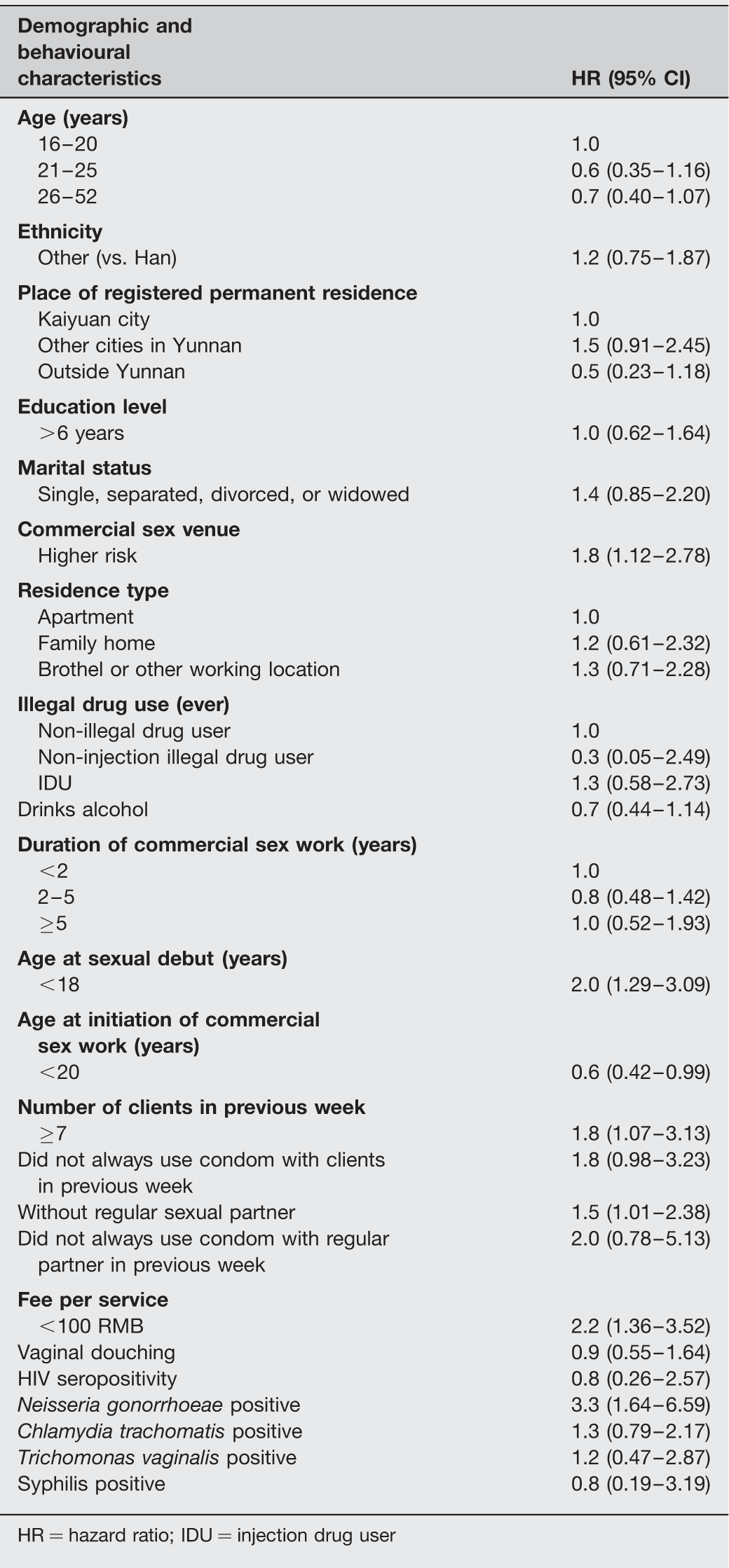
HR = hazard ratio; IDU = injection drug user
Factors associated with HSV-2 infection in multivariate analysis
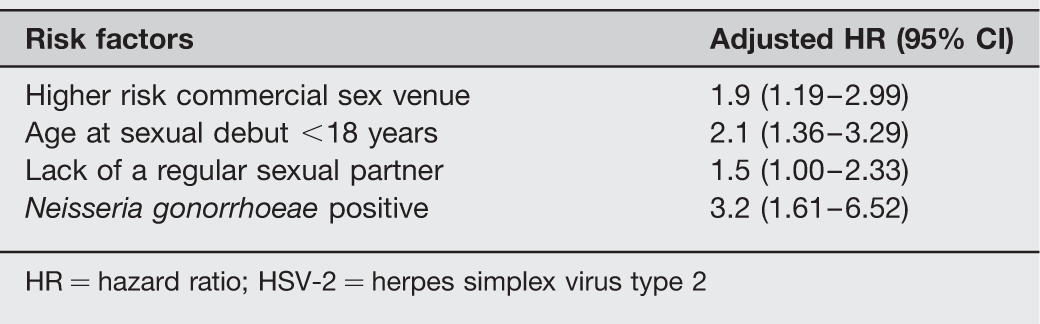
HR = hazard ratio; HSV-2 = herpes simplex virus type 2
DISCUSSION
This study found a relatively high incidence of HSV-2 infection of 21.9 per 100 PY (95% CI: 17.8–26.4) among those who were initially seronegative. HSV-2 incidence identified in our study is close to other studies (14.2–23 per 100 PY). 17 –19 A study among HIV-seronegative FSWs in Kenya found an overall HSV-2 incidence of 23 cases per 100 PY. 18 The high incidence among FSWs identified in our study is an important public health concern as HSV-2 may facilitate HIV transmission; 6 in addition, there is no cure for HSV-2 and in China there is little access to suppressive therapy. Understanding the prevalence and incidence of STIs, including HSV-2, is key to characterizing the Chinese HIV/AIDS epidemic and will aid in informing policy and prevention efforts that can help to protect and treat at-risk populations.
In this cohort of FSWs in Yunnan Province, a higher risk of acquiring HSV-2 was found among women working in higher risk commercial sex venues. This is consistent with previously reported findings of risk factors for syphilis infection in a cross-sectional study of FSWs in Xichang city, Sichuan Provice. 20 FSWs working in higher risk venues had more clients per week, with higher HIV prevalence. 15 Those FSWs who work at higher risk venues may have less education and access to health care; the clients who patronize high-risk FSW venues may also be at greater risk for infection due to similar risk factors. Intervention efforts should target FSWs working in higher risk commercial sex venues as they are more likely to acquire and be infected with HSV-2 and HIV and may transmit these viruses to their clients.
Multivariate analysis revealed that N. gonorrhoeae infection increased the risk of HSV-2 acquisition in this study population. There are several possible explanations for the relationship between the two infections. Firstly, FSWs infected with STIs, including N. gonorrhoeae and HSV-2, have the same behavioural risk factors, for example, inconsistent or incorrect condom use and frequency of sexual intercourse. However, N. gonorrhoeae infection was associated with HSV-2 acquisition after adjusting for other risk factors. Secondly, biological factors may help explain the association between HSV-2 and N. gonorrhoeae infections. N. gonorrhoeae can cause pelvic inflammatory disease, cervical inflammation and other chronic inflammation of the urogenital tract 21 –23 and chronic urogenital tract inflammation can contribute to the susceptibility of other microbial pathogens, including HSV-2. 24 However, Kaul et al. 25 found that prevalent HSV-2 infection was significantly associated with an increased incidence of N. gonorrhoeae infection. The interaction of co-infections is of particular concern in the context of disease control because STIs are known to be important co-factors in the transmission of HIV.
Notably, there was a strong association between age of sexual debut and HSV-2 acquisition, as was observed in previous findings. 17,26 Age at sexual debut could be a proxy for a number of unmeasured factors that may be associated with increased risk of HSV-2 acquisition. Early age of sexual debut may be associated with riskier sexual behaviour 27,28 and choice of sex partners with high-risk behaviour. 26 Participants with early sexual debut may be more vulnerable later in life to exploitative sexual behaviour, which may increase their contact with infected partners. 26 A study in Zimbabwe found that women with early sexual debut had a higher risk profile, including multiple lifetime partners and not completing high school. 29 Strategies to reduce HSV-2 incidence should include delaying the age of first coitus and should address the barriers that may prevent young women from doing so.
After adjusting for other risk factors, having regular sex partners was associated with decreased risk of HSV-2 acquisition. The direction of the association between HSV-2 infection and having regular sex partners is contrary to what may be expected as FSWs are more likely to have unprotected sex with their regular sex partners than their clients. There are two possible explanations for this association. First, considering the high transmission of HSV-2, FSWs with potential risk of acquiring HSV-2 from their regular sex partners could have been infected with HSV-2 before participating in the study and therefore be ineligible to participate. Second, FSWs with regular sex partners may be more conscientious of their behaviour than single women, which may contribute to the practice of less risky sexual behaviours with clients, such as being more inclined to use condoms correctly and consistently with the clients. Another study among FSWs in the Philippines also found that having regular sex partners was associated with decreased risk of having an STI and repeat infection. 30 The findings of the current study imply that intervention strategies targeting FSWs should address sexual partnerships and networks. More research should be conducted to better understand the relationship between HSV-2 infection and regular sex partners.
Nearly 10% of FSWs used illegal drugs in our cohort; illegal drug use is a serious public health concern as it can facilitate the spread of HIV. Previous research has identified illegal drug use to be associated with high-risk behaviours and HIV/STIs. Edlin et al. 31 have highlighted some FSWs may compromise safe sexual practice or may take on a riskier client base in order to earn more money to support their illegal drug use habits. In the first cross-sectional survey of our study, high HIV infection rates were found among IDUs (49.3% positive) and non-injection illegal drug users (19.6% positive), and IDU and non-injection illegal drug users had a respective 9.1- and 3.3-fold greater risk of HIV infection than FSWs who did not use illegal drugs. 15 This study has several limitations. Over 60% of eligible FSWs were lost to follow-up despite efforts by study staff to contact study participants. Chinese FSWs are a highly mobile group and there were significant differences between subjects retained in the cohort and those lost to follow-up. Participants in the cohort generally worked in lower risk commercial sex venues, had higher education, had fewer clients in the previous week and charged a higher fee per service; incidence density of HSV-2 acquisition may, therefore, be underestimated. Many of the risk factors were self-reported variables such as condom use and illegal drug use, which could be affected by social desirability and/or recall biases. However, to mitigate these biases, questions were asked about recent events, such as condom use in the previous week, and biological indicators were used to evaluate illegal drug use. Finally, this study was conducted in a cohort of FSWs in Kaiyuan County and the results of this research may not be applicable to FSWs in other parts of China.
In summary, this study determined the HSV-2 incidence among FSWs in a prospective cohort with three and a half years follow up. The high incidence of infections indicates that prevention methods are urgently needed for this vulnerable population. The results of this study have significant implications for future research and health interventions. Intervention efforts should focus on FSWs working in high-risk commercial sex venues as they are at higher risk for HSV-2 infection and transmission. Future intervention strategies should consider providing treatment for co-infections in addition to promoting safe sex behaviours as the presence of STIs may facilitate the acquisition of new infections. 15,32,33 Future research should be conducted to better understand the association between HSV-2 acquisition and regular sex partners.
Footnotes
ACKNOWLEDGEMENTS
The authors thank the staff members at the National Center for AIDS/STD Control and Prevention (NCAIDS) for their help with data management and quality control of laboratory testing. We also thank Westat, Inc. (Rockville, MD, USA) for their important role in the study design development and questionnaire revision. Finally, we also thank the staff of the Kaiyuan and Yunnan CDCs for all of their time and effort spent in helping conduct this study.