
Abstract
Numerous studies suggest that herpes simplex virus type 2 (HSV-2) increases the risk of HIV-1 infection but recent clinical trials of HSV-2 suppressive therapy failed to show an effect. We assessed the putative association between HSV-2 and HIV-1 in a population of HIV-concordant-negative, HIV-1-discordant and HIV-1-concordant-positive married couples from Dakar, Senegal. In agreement with previous studies, we observed a strong overall association between HSV-2 and HIV-1 (odds ratio 4.61; P < 0.001). However, this association was mainly determined by a low HSV-2 prevalence in HIV-concordant-negative couples compared with HIV-1-discordant and HIV-1-concordant-positive couples (23% versus 59% and 66%, respectively; P < 0.001). We observed no further differences in HSV-2 prevalence between HIV-1-discordant and HIV-1-concordant-positive couples (59% and 66%, respectively; P = 0.483). Neither the index (59% versus 62%, P = 1.000) nor recipient partners (41% versus 63%, P = 0.131) in HIV-1-discordant and HIV-1-concordant-positive couples showed significant differences in HSV-2 prevalence. HSV-2 does not constitute a clear risk factor for HIV-1 infection in this population.
Keywords
INTRODUCTION
Herpes simplex virus type 2 (HSV-2) is thought to play an important role in the spread of HIV-1 infection. 1,2 Cohort studies found that HSV-2 infection increases the risk of HIV-1 acquisition by two- to three-fold. 3,4 Functional studies showed that HSV-2 can facilitate HIV-1 acquisition by disrupting the epithelial barrier of the genital tract and by increasing the number of target cells for HIV-1 in the genital submucosa. 5,6 Other studies reported a higher risk of onward HIV-1 transmission from individuals co-infected with HIV-1 and HSV-2. 7,8 This was related to increased HIV-1 levels in genital secretions and plasma from such patients. 9,10
Despite strong epidemiological and biological evidence, randomized controlled trials of HSV-2 suppressive therapy failed to show an effect on HIV-1 infection. 11–13 Two large trials testing HSV-2 suppressive acyclovir treatment in HSV-2-positive/HIV-negative participants failed to show an impact on HIV-1 acquisition. 11,12 Another trial testing acyclovir treatment in HIV-1/HSV-2 co-infected patients failed to reduce onward HIV-1 transmission to the uninfected partners. 13 These data cast doubt on the causal nature of the observed HIV-1/HSV-2 assocations. 14,15
In the present study, we tested the putative association between HSV-2 and HIV-1 infection in a well-characterized population of HIV-concordant-negative, HIV-1-discordant and HIV-1-concordant-positive couples from Dakar, Senegal. For all included HIV-1-concordant-positive couples we confirmed viral linkage between spouses and determined the internal direction of transmission by molecular and epidemiological analyses. 16 In this way, we were able to compare HSV-2 prevalences between HIV-1-discordant and HIV-1-concordant-positive couples in general as well as between the index and recipient partners of these couples specifically. In populations with high prevalences of both HIV-1 and HSV-2, correlations between the two viruses can be expected simply because of their shared route of transmission. 17,18 Senegal has very low prevalences of both HIV-1 (<1%) 19 and HSV-2 (∼20%) 20,21 compared with other sub-Saharan African countries, allowing greater specificity for the detection of a biological association.
METHODS
Study population
HIV-concordant-negative, HIV-1-discordant and HIV-1-concordant-positive couples were recruited at the outpatient clinic of Fann Hospital in Dakar, Senegal. Blood samples and standard questionnaires with information on sociodemographics and sexual behaviour were collected. Husbands and wives were interviewed separately by a trained social assistant. All HIV-1-concordant-positive couples were previously shown to harbour genetically linked viruses by phylogenetic analysis of HIV-1 env gp41. 16 Twenty-nine HIV-1-concordant-positive couples provided sufficient epidemiological information to deduce the direction of HIV-1 transmission within the couple. 16 The study was approved by the Internal Review Board of the Institute of Tropical Medicine (Antwerp, Belgium) and by the Ethics Committees of the Senegalese Ministry of Health (Dakar, Senegal) and the University Hospital of Antwerp (Belgium). All study subjects gave written informed consent prior to enrolment.
Laboratory methods for HIV and HSV-2 diagnosis
Whole blood was drawn into EDTA tubes (Becton, Dickinson & Co., Sparks, MD, USA). Plasma was separated by centrifugation and stored at −80°C. HIV status was evaluated in plasma by current serological testing combining enzyme-linked immunosorbent assay and Western blotting assays. HSV-2 status was detected in plasma by HSV-2 enzyme immunoassay (EIA; Kalon Biological, Aldershot, UK) according to the manufacturer's instructions.
Statistical analysis
Differences in continuous and categorical variables between groups were analysed with non-parametric Mann-Whitney U or Kruskal–Wallis H, and Fisher's exact or chi-squared tests, respectively. Correlation analyses were performed with the non-parametric Spearman rank correlation test. The level of significance for all statistical tests was set at P < 0.05. Statistical analyses were performed with GraphPad Prism (version 5.01; GraphPad Software, Inc., La Jolla, CA, USA) and SPSS (version 16.0; SPSS Inc., Chicago, IL, USA) software.
RESULTS
Epidemiological and clinical characteristics of HIV-concordant-negative, HIV-1-discordant and HIV-1-concordant-positive couples
ARV = antiretroviral; HSV-2 = herpes simplex virus type 2
Data are median (interquartile range) values or n (%) when indicated. Differences in continuous and categorical variables were analysed with Kruskal–Wallis H and chi-squared or Fisher's exact tests, respectively. P values below 0.05 are in bold
*Data available for 29 of 35 HIV-1-concordant-positive couples
First we correlated HSV-2 and HIV-1 serostatus in the total study population (Figure 1a). HSV-2 and HIV-1 infections were significantly associated (odds ratio [OR] 4.61; 95% confidence interval [CI] 2.55–8.34; P < 0.001). Sixty-eight percent showed a concordant HIV-1/HSV-2 status: 75% of HIV-seronegative subjects were also HSV-2-seronegative, and 61% of HIV-1-seropositive patients were also HSV-2-seropositive. However, an important proportion of the subjects (32%) showed discordant HIV-1/HSV-2 results.
Association between herpes simplex virus type 2 (HSV-2) and HIV-1 among HIV-concordant-negative, HIV-1-discordant and HIV-1-concordant-positive couples. (a) HSV-2 prevalences of HIV-negative and HIV-1-positive subjects in the total study population. (b) HSV-2 prevalences of HIV-concordant-negative, HIV-1-discordant and HIV-1-concordant-positive couples. Couples are considered HSV-2 positive when at least one partner in the couple is HSV-2 seropositive. (c) HSV-2 prevalences of index and recipient partners in HIV-1-discordant and HIV-1-concordant-positive couples. (d) Same as panel (c) but restricted to male index and female recipient partners in HIV-1-discordant and HIV-1-concordant-positive couples. (e) Proportions of HSV-2-concordant-positive couples among HIV-concordant-negative, HIV-1-discordant and HIV-1-concordant-positive couples with at least one HSV-2 seropositive partner. (f) Same as panel (e) but restricted to HIV-1-discordant and HIV-1-concordant-positive couples with male index and female recipient partners. P values are calculated with Fisher's exact tests (two groups) or chi-squared tests (three groups)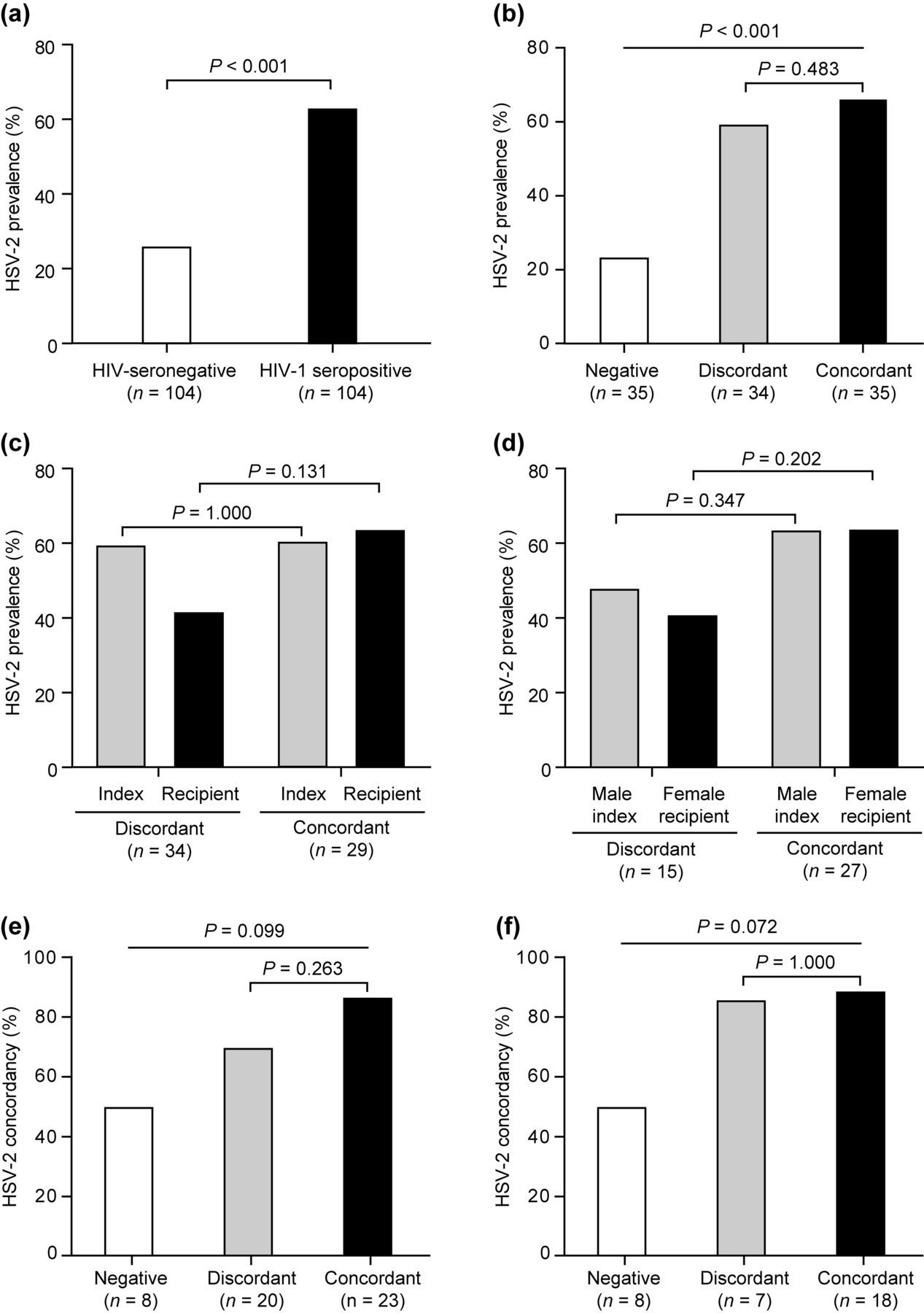
Next, we investigated whether HSV-2 infection was differently associated with the HIV-concordant-negative, HIV-1-discordant or HIV-1-concordant-positive status of the couples. In a first general analysis, couples were considered HSV-2-positive when at least one partner in the couple was HSV-2-seropositive (Figure 1b). In comparison with HIV-concordant-negative couples, HIV-1-discordant and HIV-1-concordant-positive couples showed a significantly higher proportion of HSV-2-positive couples (23% versus 59% and 66%, respectively; P < 0.001). However, no further difference was found between HIV-1-discordant and HIV-1-concordant-positive couples (P = 0.483).
Then we analysed whether HSV-2 was differently associated with index or recipient partners in HIV-1-discordant and HIV-1-concordant-positive couples (Figures 1c and d). This analysis was done for all HIV-1-discordant couples in comparison with the 29 HIV-1-concordant-positive couples with known index and recipient partners (Figure 1c), as well as for the 15 HIV-1-discordant and 27 HIV-1-concordant-positive couples with male index and female recipient partners (Figure 1d). Index partners in HIV-1-discordant and HIV-1-concordant-positive couples showed comparable HSV-2 seroprevalences (all index partners: 59% versus 62%, respectively, P = 1.000; male index partners: 47% versus 63%, respectively, P = 0.347). Recipient partners in HIV-1-concordant-positive couples showed a trend towards higher HSV-2 seroprevalence than those in HIV-1-discordant couples (all recipient partners: 63% versus 41%, respectively, P = 0.131; female recipient partners: 63% versus 40%, respectively, P = 0.202). However, this latter comparison is likely biased by the difference in HIV-1 status between the two groups.
Finally, we investigated whether HIV-1 status has an effect on the HSV-2-discordant or HSV-2-concordant status of the couples instead. To test this, we analysed the proportions of couples with a HSV-2-concordant-positive status among couples with at least one HSV-2-positive partner (Figures 1e and f). HIV-concordant-negative couples were less frequently HSV-2-concordant-positive than HIV-1-discordant couples or HIV-1-concordant-positive couples (50% versus 70% and 87%, respectively, P = 0.099; Figure 1e), but again there were no marked differences between HIV-1-discordant couples and HIV-1-concordant-positive couples (P = 0.263; Figure 1e). Similar results were obtained when this analysis was restricted to HIV-1-discordant and HIV-1-concordant-positive couples with male index and female recipient partners (50% versus 86% and 89%, respectively, P = 0.072; 86% versus 89%, respectively, P = 1.000; Figure 1f).
DISCUSSION
In this study, we found that HIV-1-seropositive subjects showed a markedly higher HSV-2 prevalence than HIV-seronegative subjects, confirming the multitude of studies reporting an association between HSV-2 and HIV-1. However, in our study, this association appeared to be mainly determined by the low HSV-2 prevalence in HIV-concordant-negative couples, and we found no further differences in HSV-2 prevalence between HIV-1-discordant and HIV-1-concordant-positive couples. Thus overall, HSV-2 infection did not constitute a clear risk factor for the acquisition or transmission of HIV-1 in our population of HIV-1-discordant and HIV-1-concordant-positive couples.
A large proportion of couples in our study were HSV-2-concordant-positive, which is in agreement with the high infectivity of HSV-2. Interestingly however, HSV-2-positive concordance was more pronounced for HIV-1-discordant and HIV-1-concordant-positive couples than for HIV-concordant-negative couples, suggesting that HIV-1 also enhances HSV-2 infection. Indeed, in addition to the increased HIV-1 incidence among HSV-2-infected subjects, several studies also observed an important increase in HSV-2 incidence among HIV-1-infected subjects. 22–24 In fact, recent studies suggest that the risk of acquiring HSV-2 upon prevalent HIV-1 infection is actually higher than the other way around and that the risk is highest for acquiring both viruses during the same follow-up interval. 25–27 Such mutual HIV-1/HSV-2 effects will contribute to the association seen at a population level, but at the same time hinder the observation of the individual effects such as attempted in the present study. Thus, understanding the relative contributions of HIV-1 and HSV-2 to their overall association will be crucial for the interpretation of observational studies and clinical trials. To achieve this, precise longitudinal studies with shorter follow-up intervals will be needed to obtain better detail on the sequence of acquisition events for both viruses.
Alternatively, our data could support the hypothesis that HSV-2 infection has no causal effect on the acquisition or transmission of HIV-1. Some authors have raised this possibility following the failure of the acyclovir clinical trials. 11–13 They suggested that the association between HSV-2 and HIV-1 primarily reflects their shared route of transmission and the effect that, for example, high-risk sexual behaviour has on the incidence of both viruses. 14,15 Indeed, given that HSV-2 is substantially more infectious than HIV-1, individuals engaging in high-risk sexual behaviour are more likely to acquire HSV-2 before they acquire HIV-1, without this necessarily reflecting a causal relationship. 17,18 This hypothesis could explain why in Senegal, a country with very low HIV-1 and HSV-2 prevalences compared with other sub-Saharan African countries, HIV-1 and HSV-2 were significantly associated in a population of high-risk female sex workers but not in a population of low-risk pregnant women. 28 This is also consistent with the high HSV-2 prevalence noted among HIV-negative female sex workers in Kenya. 29 In this population, HSV-2 serostatus was associated with a longer duration of high-risk sexual behaviour but not with increased susceptibility to HIV-1 infection, 29 which is in agreement with our findings.
The sample size of our study was relatively small and as a result it is possible that we have missed potentially weak effects of HSV-2 on HIV-1 transmission in our study population. For instance, we lacked sufficient statistical power (<70%) to refute the link between HSV-2 and HIV-1 transmission if we considered differences in HSV-2 prevalence between study groups of less than 25% to be biologically relevant. On the other hand, differences in HSV-2 prevalence between study groups were generally much lower than 25%, which supports our conclusions. Nevertheless, confirmatory studies in larger study populations of HIV-1-discordant and HIV-1-concordant-positive couples remain warranted.
In summary, HSV-2 infection did not constitute a clear risk factor for HIV-1 infection in our population of HIV-1-discordant and HIV-1-concordant-positive couples in Dakar, Senegal. Our data could suggest that the interaction between HIV-1 and HSV-2 is more complex than previously thought. Detailed longitudinal studies will be required to dissect the exact temporal relationship between HIV-1 and HSV-2 acquisition.
Footnotes
ACKNOWLEDGEMENTS
We thank Abdoul Aziz Diallo and Marema Fall for technical assistance; Ndeye Fatou Ngom Gueye, Ibrahima Ndiaye, Khady Ba Fall, Marianne Ndiaye for the recruitment, counselling and follow-up of the participants; Aïssatou Gaye Ndiaye, Tania Crucitti and Bénédicte De Deken for HIV and HSV-2 serological testing. This work was supported by the Belgian Fund for Scientific Research (FWO-Vlaanderen, grant G.0660.06) and the Belgian Directorate-General for Development Cooperation.