
Abstract
Workforce planning is an inexact science. Specialty and Associate Specialist (SAS) doctors are rarely included in workforce analyses. Past studies have shown that SAS doctors are significant contributors to the work in genitourinary (GU) medicine clinics. This survey confirms the large amount of clinical work undertaken by SAS doctors. It appears that 51% of SAS doctors in GU plan to retire in the next 15 years and it is uncertain what effect the 2008 SAS contract will have on SAS recruitment. This information should be taken into consideration in future GUM workforce planning.
INTRODUCTION
The importance of workforce planning is well recognized and there are national recommendations for the number of consultants according to the population size being served.1,2 However, medical workforce planning is an inexact science partly because of multiple unquantifiable factors such as the reconfiguration of services, changing workforce roles and expectations, new commissioning arrangements and consultant retirement, but also because of lack of accurate and timely data. The difficulties in planning are further complicated by the current economic climate, uncertainty about how sexual health services will operate in the future and by lack of information on the activities of Specialty and Associate Specialist (SAS) doctors. In the past workforce surveys in genitourinary (GU) medicine have concentrated on consultant 1 and trainee numbers. 3 Activities and numbers of SAS doctors are difficult to quantify as they are not monitored by the Royal College of Physicians (RCP) or included in their census. SAS doctors were recognized over a decade ago as being significant contributors to the GU medicine medical workforce. It was estimated that 592 SAS doctors, including clinical assistants, were conducting 1685 GU medicine clinics per week and were referred to as ‘a reliable silent backbone of the specialty’. 4
Despite the difficulties it is essential that data are obtained in order to facilitate accurate workforce planning. The Centre for Workforce Intelligence (CfWFI) obtains data from various sources, again involving estimates, to inform its reports. In order to enhance this information the British Association for Sexual Health and HIV (BASHH) commissioned a survey of SAS doctors.
METHODS
The survey was devised using the Survey Monkey tool and was publicized by BASHH with email prompts to everyone on the BASHH database and through the SAS doctors’ committee database. The survey was open for completion for three months starting in March 2011.
RESULTS
Gender, contract and area of work responses

GU=genitourinary; SAS=Specialty and Associate Specialist
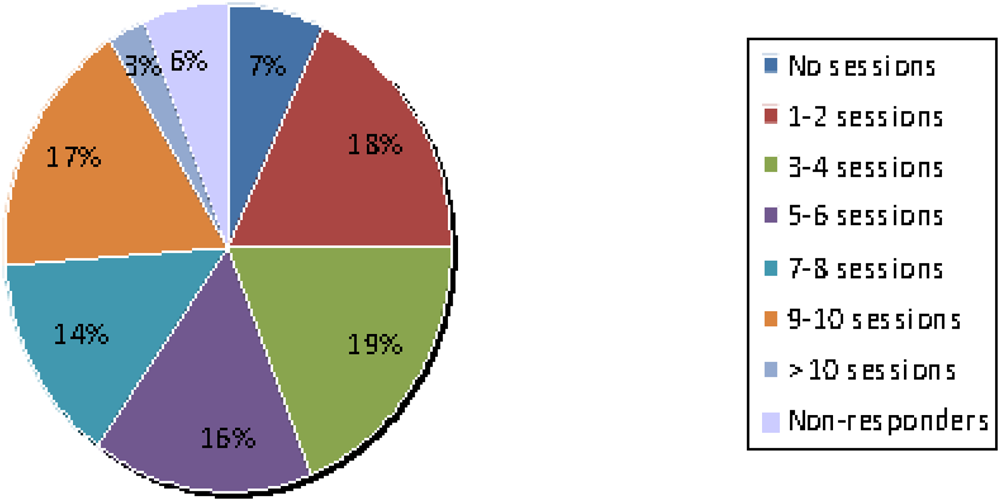
Percentage of Specialty and Associate Specialist respondents working sessions in Level 3 genitourinary medicine clinics
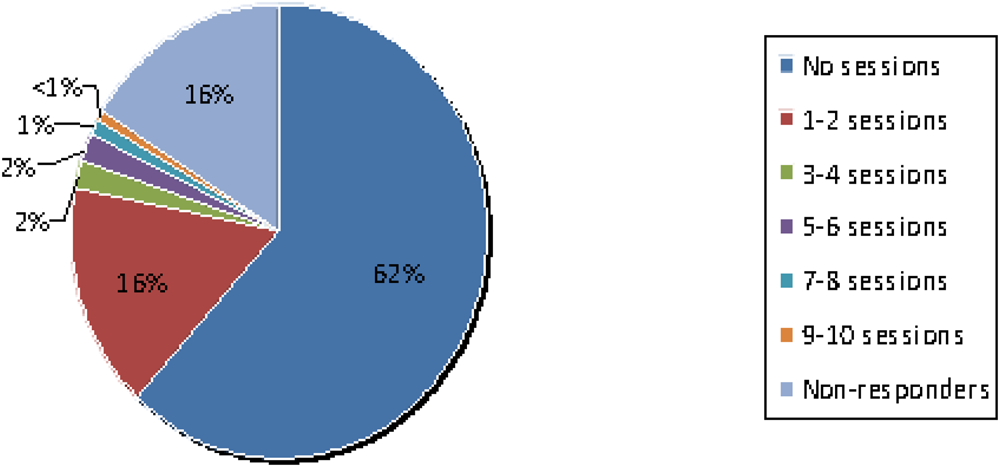
Percentage of Specialty and Associate Specialist respondents working sessions in Level 3 HIV clinics
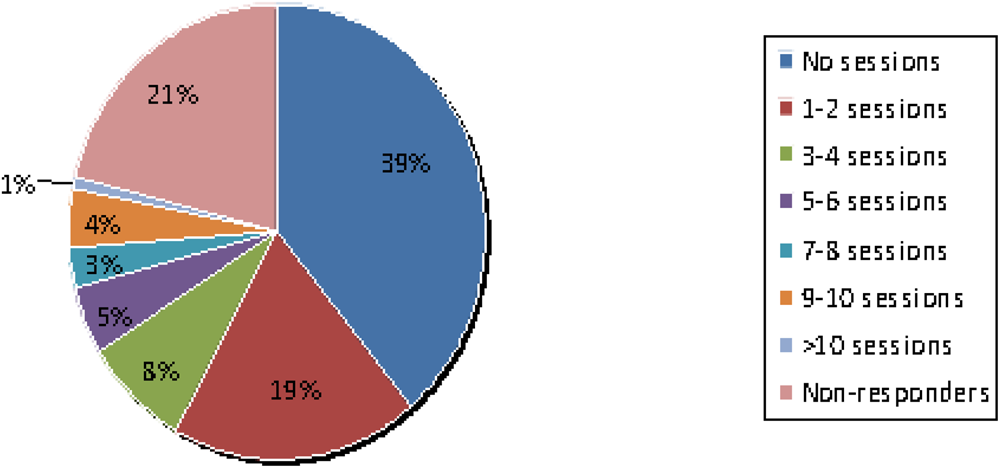
Percentage of Specialty and Associate Specialist respondents working sessions in Level 3 sexual and reproductive health clinics
Of those on the ‘new’ 2008 SAS contract, 44% of all respondents were specialty doctors and 30% were associate specialists (AS). Of those on the ‘old’ contract, 4% of all respondents were staff grade doctors, 7% were AS doctors and 13% described themselves as ‘other’.
In total, 60% were BASHH members, 25% were working in the London area, almost 12% were in Scotland and the rest were evenly spread across England and Wales.
Overall, 7% of respondents worked no sessions per week in Level 3 GU medicine, 18% 1–2, 19% 3–4 sessions, 16% 5–6 sessions, 14% 7–8 sessions, 17% 9–10 sessions and 3% more than 10 sessions. The non-responder rate was 6%. See Figure 1.
In respect of HIV Level 3 work, 62% did no HIV Level 3 sessions, 16% 1–2 sessions, 2% 3–4 sessions, 2% 5–6 sessions, 1% 7–8 sessions, <1% 9–10 sessions and none worked more than 10 sessions. The non-responder rate was 16%. See Figure 2.
In respect of sexual and reproductive health (SRH) at Level 3, 39% did no sessions, 19% did 1–2 sessions, 8% 3–4 sessions, 5% 5–6 sessions, 3% 7–8 sessions, 4% 9–10 sessions and 1% did more than 10 sessions. The non-responder rate was 21%. See Figure 3.
It should be noted that a further 21% of respondents reported doing some SRH work at Level 2.
In total, 44% of respondents indicated that they worked exclusively in GU medicine/HIV/SRH while 29% of respondents reported undertaking some sessions in other specialties including general practice, psychosexual medicine, forensic medicine, tuberculosis medicine and addiction psychiatry. The remainder, 27%, did not respond to this question.
In terms of retirement over the next 15 years, 51% of respondents planned to retire within this period; of these, 7% by 2013, 13% between 2014 and 2016, 13% between 2017 and 2021, 14% between 2022 and 2026. Nineteen percent of respondents were unsure exactly when in the next 15 years they would retire and 34% did not respond to this question.
Overall, 80% of respondents had undergone formal appraisal within the last year for their HIV/GU medicine work; 79% were appraised by a GU medicine/HIV physician.
DISCUSSION
In the survey, the SAS doctors were asked for the actual number of Level 3 GU medicine clinics and Level 3 HIV clinics per week that they delivered. Therefore, the total absolute number of clinics delivered by the 230 SAS doctors responding to the survey was obtained. If these figures are extrapolated, using an estimated response rate of 40%, and if all SAS doctors work similarly they would conduct 2770 Level 3 GU medicine clinics per week and 317 Level 3 HIV clinics per week. This is a significant contribution to the overall workload of Level 3 services. In addition, the number of sexually transmitted infections diagnosed, including HIV, continues to rise. 5
In the survey, 51% of the SAS doctors doing sessions indicated that they intend to retire within the next 15 years and it is uncertain what effect the new SAS contract will have on SAS recruitment, given that the AS grade is closed to new entrants.
It is difficult to assess exactly the validity of our estimate of a 40% response rate to the questionnaire. In addition, there is increasing integration of GU medicine with SRH, meaning that some SAS doctors primarily trained in SRH will be doing GU medicine work supported by GU medicine colleagues and vice versa. As joint working and integration of GU medicine and SRH teams becomes more common, accurate human resources predictions become even more complex and challenging.
Despite these limitations, it is clear that SAS doctors provide a major input to sexual health service work and as 51% plan to retire over the next 15 years this is a crisis in waiting. Inclusion of SAS data in workforce planning is essential to avoid the crisis becoming a reality.
These data will be used to inform CfWFI to better estimate requirements for the specialty.
Footnotes
ACKNOWLEDGEMENTS
The authors are grateful to all the SAS doctors who completed the online survey.