
Abstract
This was a cross-sectional study using an online survey to evaluate the provision of nurse-led and delivered services within genitourinary medicine in the UK. Results showed that such services are being widely utilised and are generally well supported by medical staff. The delivery of nurse-led and delivered services appears to be quite variable. Clinical guidelines and standards may help to ensure a more uniform approach to these services and help to maintain high standards of care.
Introduction
In 2006, the Department of Health published 10 ‘High Impact Changes’ 1 to optimise patient’s access to genitourinary medicine (GUM) services within 48 h of self-referral. One suggested change was to ‘analyse and improve utilisation of the multidisciplinary teams in GUM’. 1 It recognised that nursing roles had already expanded but that there was scope to take this even further. Other suggested changes included triaging patients so that uncomplicated patients could be managed by more junior staff, and matching patient demand for services with opening hours and appropriate levels of staffing.
Over the past 10 years we have seen a great expansion in the role of nurses working within sexual health. There have been particular developments in nurse-led and delivered services. A study from central London in 2002 showed that ‘trained, experienced specialist nurses supported within the multidisciplinary team are at least as effective in the assessment and management of female patients as senior house officers’. 2 These changes are supported by Department of Health ‘Framework for Sexual Health Improvement’ in England published in 2013. 3 These guidelines acknowledge the diversity of staff working within GUM and that ‘safe, efficient, cost-effective and high quality care relies on the right mix of staff with the right mix of skills’. 3 This report also highlighted that to ensure clinical excellence is maintained there should be appropriate arrangements for continuing professional development (CPD) and staff should be supported to undertake appropriate training.
Although there is established guidance to suggest that the development of advanced roles for nurses within GUM is important and cost-efficient there is little guidance on how to implement this and ensure standards of clinical governance are maintained. The British Co-operative Clinical Group (BCCG) has devised a study to investigate how such clinics are being implemented, managed and received across the United Kingdom.
Methods
This cross-sectional study used an online survey to assess the provision of nurse-led and delivered services within GUM in the UK. The questionnaire was developed by the members of BCCG and three GUM nurses. The questionnaire was distributed to sexual health services across the United Kingdom using an established online survey software platform. 4 A copy of the questionnaire is available in supplementary file A.
Ninety-two sexual health clinics and linked family planning clinics across the UK were identified by the regional representatives of BCCG and the survey was distributed to these clinics in 2013. Lead consultants and nurses of sexual health clinics were sent an electronic invite to complete the online self-administered survey. Respondents were encouraged to seek the opinion of the multidisciplinary team prior to completion.
Important clinic characteristics were assessed, including: clinic design, clinical setting (for example acute site, community setting, or specific location), annual attendance and method of service delivery. Participants were asked about the proportion of clinics that are nurse-led or delivered and the medical support provided for these. Other areas included in this survey were: training, funding for training, clinical governance, arrangements for prescriptions and any concerns or issues raised regarding nurse-led or delivered services.
Results
A total of 64 (70%) clinics completed the survey. Of these 55 (86% of responders) completed the survey in full. Although 14 clinics did not respond to the survey in full, their answers to questions they did complete were still considered. Results were therefore calculated based on the response rate per question rather than survey response as a whole.
Clinic settings
These clinics were based in a variety of settings. A significant proportion (30, 47%) were within acute hospital Trusts, however, there were also many respondents from community settings (n = 22, 34%). There was also one social enterprise clinic, one was based in the third sector and nine were based in a variety of more specific settings including schools, mental health Trusts, councils and youth groups.
Clinic activities
Annual attendance was provided by 81% (52/64) of clinics responding to this survey. The median total annual attendance for contraception as the primary reason for consultation was 3750 (range 0–22,400). Attendance for GUM services was 10,034.5 (range 0–64,000) and 12,995.5 (range 0–106,000) for integrated services.
Summary of the method of delivery of services within the participating clinics.

Clinical governance
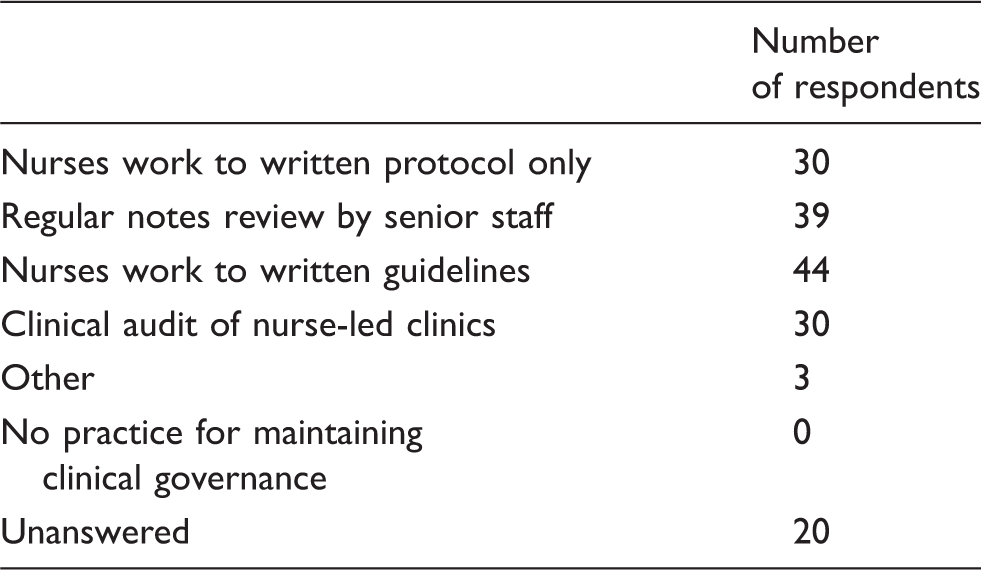
Methods for maintaining clinical governance.
Level of training of nurses providing nurse-led and delivered services.

The majority of clinics utilised patient group directions (PGD) for provision of medications (52/55, 95%). In 60% of cases (33/55) independent non-medical prescribers were available in clinic. In just four clinics (7%) nurses were reliant on doctors for all prescriptions.
The proportions of nurses trained in either GUM or contraception working within services varied amongst clinics. Clinics were asked what percentage of their clinic nurses had been trained in GUM and/or contraception. The median responses were as follows: 39.7% were trained in contraception only, 45.0% were trained in GU medicine only and 69.8% were trained in GU medicine and contraception. The survey also asked respondents what bands of nurses or health-care assistants (HCAs) were providing different kinds of services within clinics. With regard to asymptomatic screening the bands of nurses and HCAs reviewing these patients ranged from band two to five, although the majority were band five or above (89% 122/137). In all but one clinic, band five nurses and above were managing symptomatic GU patients and genital warts. The remaining clinic also utilised band four HCAs for this service. In all clinics, band five nurses and above were providing basic contraception. Advanced contraception in all but one clinic was provided by band six nurses (one clinic utilised band five nurses).
Funding for training appeared to be quite variable across clinics. A large proportion reported receiving some allocated funding from their Trusts (39/52, 75%). Many nurses had to rely on other methods of funding, which included: departmental charitable funds (18/52, 35%), sponsors (6/52, 12%), funding raised through educational activities (16/52, 31%) and self-funding (12/52, 23%). One clinic received some funding from the Strategic Health Authority and two had discretionary finding from their trusts.
An open-ended question was included at the end of the survey asking respondents if they had any concerns regarding nurse-led or delivered services. Forty-eight clinics responded to this question. Of these, 56% (n = 27) raised no concerns. Eight percent (n = 4) reported no concerns providing adequate support, training and robust clinical governance. Thirty-five percent (n = 17) raised some concerns. For those who reported concerns or made additional comments, the general themes were as follows:
Adequate supervision and support (n = 5), training, protected CPD time and upkeep of skills (n = 6). Management of complicated patients, including under 16s (n = 5). Presentation of problems outside competency of assessing nurse (n = 3). Triage (n = 3). Cost effectiveness (n = 1). Maintaining clinical governance and high standards of care throughout (n = 4) and efficiency (n = 2).
Other specific issues raised were: the impact of tendering on training and development; lack of scope for development of nurse-led coil services without a doctor present (due to potential need for intravenous atropine); and the possibility of increases in the number of follow-up patients seen by doctors due to problems not resolved within a nurse-led clinic.
Discussion
The results of this national survey show that nurse-led and delivered services are being widely utilised across the United Kingdom. They are well supported by medical staff and the majority of respondents to the questionnaire had no concerns regarding the safety and efficacy of these clinics.
Where concerns were raised these were mostly related to clinical governance, maintenance of training and skills and the potential for nurses to encounter problems beyond their competence. Reassuringly, all respondents who reported nurse-led or delivered services also reported some method of maintaining clinical governance, and in 91% (48/53) of cases this involved nurses working to written guidelines or protocols or both. This may help to alleviate concerns raised by clinicians regarding clinical governance.
There is wide variability in the way different services have developed and support their nurse-led clinics. These differences are highlighted particularly in the responses to training, supported and clinical governance. The development of national, clinical guidelines may help to reduce the variability in these areas and help services to feel supported in maintaining training and clinical governance. This may in turn help to eliminate concerns raised regarding these clinics. This is particularly relevant in the current climate where clinics are going through huge changes, with many going through the tendering process and being redeveloped.
Only 12 clinics who reported band two or three HCAs were reviewing asymptomatic patients within their service. With the widespread use of dual nucleic acid amplification tests for gonorrhoea and chlamydia and the development of asymptomatic pathways, where often no examination or microscopy is taking place, it is likely we will also see expansion in the roles of HCAs within GUM services. Written guidelines and protocols would assist in the development of these services and clinic pathways and help to ensure that high standards of clinical care are maintained across the board.
In order for nurses to develop and maintain skills required to provide nurse-led and delivered services it is imperative that there is appropriate access to funding for appropriate training. The method of access to funding varied significantly between Trusts, although in the majority (75%, 39/52) of cases this was accessed through the Trust. A recommendation would be that a clear, established and accessible funding pathway provided by the Trust is required to enable nurses to develop and maintain these clinical skills and is essential for the continued support and development of nurse-led and delivered services.
There are several limitations in this clinical survey. A large number of surveys returned were incomplete and some clinics submitted results more than once, which made some of the data difficult to analyse. Thirty percent of clinics failed to respond to the survey; however, due to the large number of responses (64/92) it is felt that this survey is likely to be representative of most clinics across the United Kingdom. Some questions included in the original survey were worded in a manner that was open to interpretation, and it was evident from the results that multiple respondents had misunderstood and therefore these were eliminated from the analysis. These included the following two questions:
In a routine day across the service, what is the proportion of nurse-delivered clinics per week?.
a) GUM, b) Integrated GUM/contraception, c) Contraception, d) HIV.
What is the number of senior doctor (consultant/specialist grade doctor)-led clinics per week?.
a) GUM, b) Integrated GUM/contraception, c) Contraception, d) HIV.
Invitations to complete the survey were distributed to lead clinicians and nurses of the selected GU services. Although respondents were encouraged to seek the opinions of the multidisciplinary team prior to completion, bias may have been introduced into the results if these wider views were not sought. This is particularly relevant to certain aspects of the survey, such as those addressing funding, training and the degree of medical support available to nursing staff.
Conclusions
Overall, the survey results are positive regarding nurse-led and delivered services. These services are being widely utilised across the United Kingdom. Clinical guidelines and standards may help to ensure a more uniform approach to training, support and delivery to ensure high standards of clinical care are maintained across the board.
Footnotes
Acknowledgements
The authors thank the British Co-operative Clinical Group.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.