
Abstract
This case report describes two severe antiretroviral drug adverse reactions that occurred in the same patient. A 55-year-old HIV-positive African woman received a single epidural triamcinolone injection for pain relief of postherpetic neuralgia. Forty-one days later, she developed severe iatrogenic Cushing’s syndrome due to the drug–drug interaction between triamcinolone and her boosted protease inhibitor therapy. The patient’s antiretroviral regimen was thus changed to replace her protease inhibitor with the integrase inhibitor raltegravir. Shortly after commencing the drug, the patient developed a severe adverse drug reaction manifesting as Drug Reaction (or Rash) with Eosinophilia and Systemic Symptoms (DRESS) syndrome. First described in 1996, this hypersensitivity syndrome presents with severe skin reaction as well as fever, rash, lymphadenopathy and internal organ involvement with marked eosinophilia. Clinicians should be aware of raltegravir-induced DRESS syndrome as well as the potential for drug–drug interactions due to protease inhibitor-based therapy.
Introduction
The integrase inhibitor raltegravir (RAL) is increasingly used in patients with potential drug interactions. 1 Common side effects include nausea, vomiting, diarrhoea, abdominal pain, headache, fatigue and dizziness. Most recently, severe skin-related side effects have been noted leading to the recent update to the Isentress (RAL) package insert (approved on 2 November 2011). 2
DRESS syndrome stands for Drug Reaction (or Rash) with Eosinophilia and Systemic Symptoms. The term was coined in a 1996 report in an attempt to simplify terminology for a syndrome recognized as early as 1959. 3 It is an adverse drug reaction that may manifest with rash, fever, hepatitis, lymphadenopathy and characteristic haematologic abnormalities such as eosinophilia, thrombocytopaenia and atypical lymphocytosis. The syndrome carries about a 10% mortality. 4 Treatment is cessation of the causative medication and supportive care. Systemic steroids are commonly used as well; however, there are no controlled clinical trials to assess the efficacy of this treatment. 5
With more frequent use of newer antiretroviral medication, more side effects will become apparent. We describe a case of DRESS syndrome in a patient secondary to RAL.
Case report
A 55-year-old African woman living in the UK was diagnosed with HIV in 2005 following a confirmed case of Pneumocystis jirovecii pneumonia; her CD4 nadir was 30 cells/µl. She had a past medical history of Type 2 diabetes mellitus and severe postherpetic neuralgia (PHN) secondary to a severe episode of multi-dermatomal herpes zoster in 2002. Antiretroviral therapy (ART) was commenced with efavirenz (EFV), tenofovir (TDF) and emtricitabine (FTC) and virological suppression achieved. Following an unplanned treatment interruption three years later, drug resistance was suspected. EFV was stopped and protease inhibitor (PI) and atazanavir (ATV)/ritonavir were started.
Due to ongoing severe PHN, ongoing specialist pain review was undertaken. Despite extensive treatment, the only effective intervention the patient reported had been epidural corticosteroid triamcinolone in 2004, prior to HIV diagnosis.
In 2009, the patient received a further lumbar epidural depot injection of 80 mg triamcinolone. Forty-one days later following injection, the patient was admitted in a hyperglycaemic and hyperosmolar state, with facial swelling, dorsocervical fat pads and facial hirsutism. Investigations confirmed Cushing’s syndrome secondary to the use of steroids and their likely interaction with ATV/ritonavir. ATV/ritonavir was changed to RAL to avoid further CYP P450 interactions.
Four weeks after commencing RAL, the patient remained virally suppressed with a CD4 + 305 cells/µl (19%) but presented with a two-day history of a rapidly progressive generalized maculopapular rash, pruritus, malaise and pyrexia (Figure 1).
Generalized maculopapular rash.
Co-trimoxazole and codeine had also been commenced at the time of RAL. Both the codeine and co-trimoxazole were stopped immediately on admission, noting that the patient had also received co-trimoxazole on a previous occasion with no ill effect. Despite discontinuation, the patient continued to remain symptomatic and pyrexial with worsening biochemistry. Eosinophil count was 1.5 × 109/L and liver function tests were elevated: albumin 38 g/L (40–52 g/L), alkaline phospatase 182 IU/L (35–123 IU/L), bilirubin 7 µmol/L (0–21 µmol/L), alanine transferase 65 IU/L (4–45 IU/L) and gammaGT 138 IU/L (4–60 IU/L). C Reactive Protein (CRP) was elevated at 76 mg/L.
As a result of the worsening clinical picture despite withdrawal of other possible causative drugs, a diagnosis of DRESS syndrome secondary to RAL was made. Differing scoring systems have been suggested for confirming diagnosis of DRESS. 6 They take into account the presence of fever (>38.5), enlarged lymph nodes >2 sites and >1 cm, atypical lympocytes, eosinophilis, skin rash (including how extensive and if the rash was biopsied), internal organ involvement, duration of resolution and exclusion of alternative diagnosis. Using this system the described case ‘scores’ equals >5 equating to definite DRESS. This score is generated by the patient needing hospitalization, having a fever of 38.9℃, an elevated eosinophil count, widespread rash with scaling and pupura and liver involvement.
RAL was stopped and a PI recommenced. In moderate to severe cases of DRESS, high-dose systemic steroids are usually required. However, in view of the history of Cushing’s syndrome in this patient, a decision was made by the dermatologists to initiate treatment with prednisolone but at a lower dose of 20 mg/day in addition to topical emollients. Skin biopsy showed compact orthokeratosis, mild diffuse spongiosis with lymphocytic exocitosis with occasional neutrophils. Focal eosinophilic exocitosis and rare individually dyskeratotic keratinocytes, and mild superficial and mid-perivascular and interstitial lymphoid cell infiltrate with eosinophils and papillary dermal oedema consistent with a drug eruption (Figure 2).
Skin biopsy histology.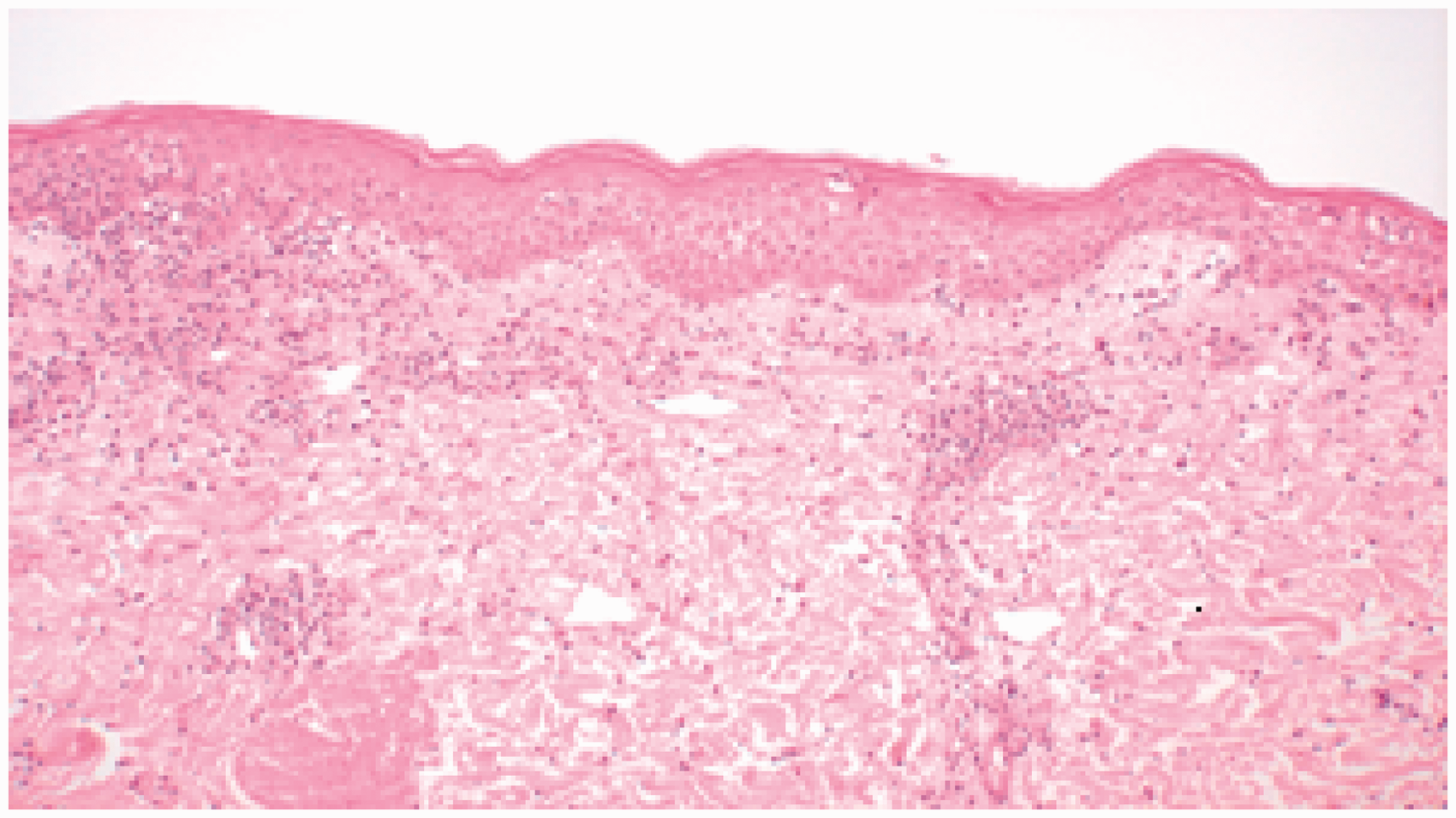
The patient continued on a reducing steroid regimen for six weeks. The rash improved and eosinophil count declined to normal, as did the liver function tests.
Discussion
Interactions of steroid and ritonavir-boosted PIs have previously been described. The extreme Cushingoid response to epidural steroid injection serves as a reminder that any corticosteroid treatment may lead to a significant interaction, causing both significant physiological and psychological complications.
DRESS syndrome is previously described in other antiretrovirals 7 and one additional case has been described in relation to RAL. 8 This case adds to the literature a significant dermatological reaction to RAL, in this instance DRESS. Therapeutic use of RAL was indicated; however, clinicians should be alert for previously undocumented reactions to newer classes of drugs such as integrase inhibitors.
Footnotes
Conflict of interest
The authors declare that there are no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.