
Abstract
Raltegravir was the first licensed integrase inhibitor. Real-life experience is informative and complements trial data. We therefore evaluated raltegravir use in adults in a large HIV treatment centre. From pharmacy and departmental HIV database records, we identified all adults taking ≥1 dose of raltegravir from first availability to the end of November 2012. Data were collected using a standardised case report form. Two hundred and fifteen individuals provided 502 patient-years (median 2.6 years/person) of raltegravir use. Of 215 individuals, 166 (77%) were male, median age 43 years; 189 (88%) were antiretroviral therapy (ART)-experienced and 26 (12%) ART-naive, with median baseline CD4 counts of 324 and 54 cells/µL, respectively. Of ten individuals using once-daily raltegravir, four, with good adherence remained virologically suppressed after a median 28 months, four stopped against medical advice, one stopped to simplify and one failed virologically. In hepatitis co-infection, 35 individuals (92 patient-years) took raltegravir without evidence of hepatotoxicity. Six women started raltegravir during pregnancy for intensification (5/6) or switch for tolerability without complications. Of ten individuals stopping raltegravir after virological failure, 2/4 with successful sequencing showed resistance. Raltegravir appears safe and effective, without evidence of toxicity above that in published trials, including in pregnancy and co-infections. Once-daily dosing seems effective where adherence is good.
Keywords
Introduction
Raltegravir was the first integrase strand transfer inhibitor (INSTI) in clinical use in combination antiretroviral therapy (ART) for human immunodeficiency virus (HIV) infection. Licensed by the European Medicines Agency in December 2007, 1 its efficacy has been demonstrated in clinical trials including ART-naive 2 and -experienced 3 individuals.
In treatment guidelines issued by the British HIV Association (BHIVA), shortly after the licensing of raltegravir, it was first recommended for use in ART-experienced individuals, as part of an individualised combination. 4 In later guidelines, following an extension of the license to include use in ART-naive individuals in September 2009, 1 it is recommended as a preferred third agent in ART-naive individuals. 5 Raltegravir, and the newer INSTIs, has been shown to reduce HIV viral loads (VLs) more rapidly than agents with which they have been compared2,3 and this property may be exploited in some specific circumstances.
Real-life, post-marketing experience is informative, can differ from and can complement trial results. In this study, we aimed to describe our practice and experience in using raltegravir on- and off-license, since its availability, in a wide range of adult patient groups at a large UK HIV centre, using retrospective case note review.
Methods
Setting
The Monsall Unit has around 2000 HIV-positive individuals regularly attending for care and has been a centre for HIV treatment since the first detection of HIV in the United Kingdom in the early 1980s. In general, BHIVA guidelines are followed and physicians in the department include co-authors of these guidelines.
Study methods
This was a retrospective, observational study evaluating routine clinical care. Pharmacy data and the departmental HIV database were used to identify all HIV-1 infected adults who had taken one or more doses of raltegravir, outside of clinical trials, from its availability (including expanded access) to 30 November 2012 at the Monsall Unit. We excluded those taking raltegravir as part of clinical trials as their data would already be published in those studies and because their management would reflect the clinical trial setting rather than routine clinical care. A standardised reporting form was used to collect demographic, clinical and laboratory data from electronic records, supplemented by paper records where necessary. The primary source of information was the detailed summary letter to the primary care physician (General Practitioner or GP) from each consultation. For a minority of individuals not registered with a GP, or not permitting correspondence with the GP, our practice is that letters are written in the same way but kept in hospital records only. Information recorded in routine clinical records was interpreted by investigators collecting data as far as was considered reasonable and ‘unknown’ recorded if data were not available or reasonable interpretation from clinical records not possible. Multiple reasons for starting or stopping raltegravir could be recorded per individual.
Duration on raltegravir was calculated from the start date to the time of the last contact with the patient when they were known to be taking raltegravir, usually the most recent outpatient visit. Mutations were analysed in the regional referral laboratory and sequences submitted to the Stanford database (http://hivdb.stanford.edu) for interpretation.
Results
Study population
A total of 227 HIV-1 infected individuals were identified; 12 were excluded in total because insufficient clinical data were available (n = 7); raltegravir was used in a clinical trial (n = 2); identification details did not correspond to an existing patient (n = 2) and <18 years old (n = 1). Therefore, 215 individuals were included, with a median duration of 2.6 years on raltegravir use (interquartile range [IQR] 0.8, 3.5 years), giving 502 patient-years total raltegravir use. Raltegravir was stopped in 68 individuals, with the remaining 147 still taking raltegravir at the time of last contact.
Of these 215 individuals, 166 (77.2%) were male; median age was 45 years (IQR 38, 51) for males and 38 years (IQR 33, 43) for females; 144/166 (86.7%) of males and 10/48 (20.8%) of females were Caucasian and 19/166 (11.4%) of males and 35/48 (72.9%) of females were Black African; 189/215 (87.9%) were ART-experienced at the time of starting raltegravir (although 25 of these 189 were not taking ART at that time), with a median CD4 count of 323 cells/µL (IQR 132, 569) and 26/215 (12.1%) were ART-naive, with a median CD4 count of 54 cells/µL (IQR 23, 258).
Reasons for starting raltegravir
Among 26 ART-naive individuals, raltegravir was started for ‘rapid HIV viral load reduction’ in 14/26 (53.8%) to avoid drug–drug interactions (DDIs; 13/26 [50.0%]) or for tolerability reasons, including contraindications to efavirenz. Raltegravir was started during hospitalisation in 18/26, among whom the median CD4 count was 25 cells/µL (IQR 10, 95) and VL was 117,600 copies/mL (IQR 25,380, 642,081) compared with a median CD4 count of 330 cells/µL (IQR 226, 368) and VL of 18,033 (IQR 7100, 28,965) among those starting as an outpatient. Among 189 ART-experienced individuals, 217 reasons for selecting raltegravir were recorded, including 113/189 (59.8%) for tolerability reasons and 48/189 for previous virological failure (Figure 1).
Reasons for starting raltegravir in 189 ART-experienced individuals (217 recorded reasons; VL = viral load; DDI = drug–drug interactions).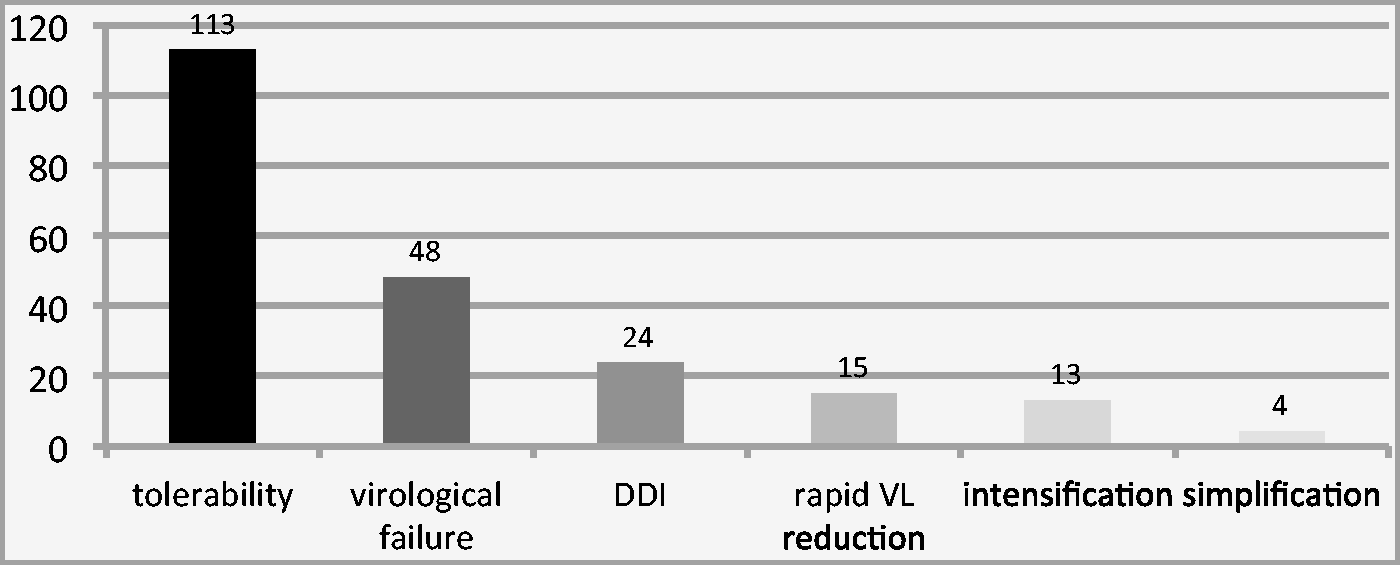
Accompanying drugs
In ART-naive individuals, raltegravir was co-administered with a fixed dose of tenofovir/emtricitabine in 17/26 and abacavir/lamivudine in 3/26. The remaining six took raltegravir in protease inhibitor (PI)-containing regimens, due to complex comorbidities (for rapid VL reduction; n = 5; 2/5 with suspected primary drug resistance) or contraindications to nucleos(t)ide reverse transcriptase inhibitors (NRTIs; n = 1). All six took ritonavir-boosted darunavir at the once-daily 800 mg darunavir/100 mg ritonavir dose as part of those PI-based regimens, and of these, four also had NRTIs as part of their combination therapy (one because of hepatitis B co-infection). Four of six on PI-based regimens started ART as inpatients with advanced HIV disease (baseline CD4 counts 45, 110 and 225 cells/µL [one baseline CD4 count unknown]). Of these four, three later stopped raltegravir to simplify their ART regimens because resistance test results were available (2/3) or because the VL became undetectable after discharge and the remaining regimen was considered sufficient.
Accompanying regimens in antiretroviral therapy (ART)-naive and ART-experienced individuals starting raltegravir.
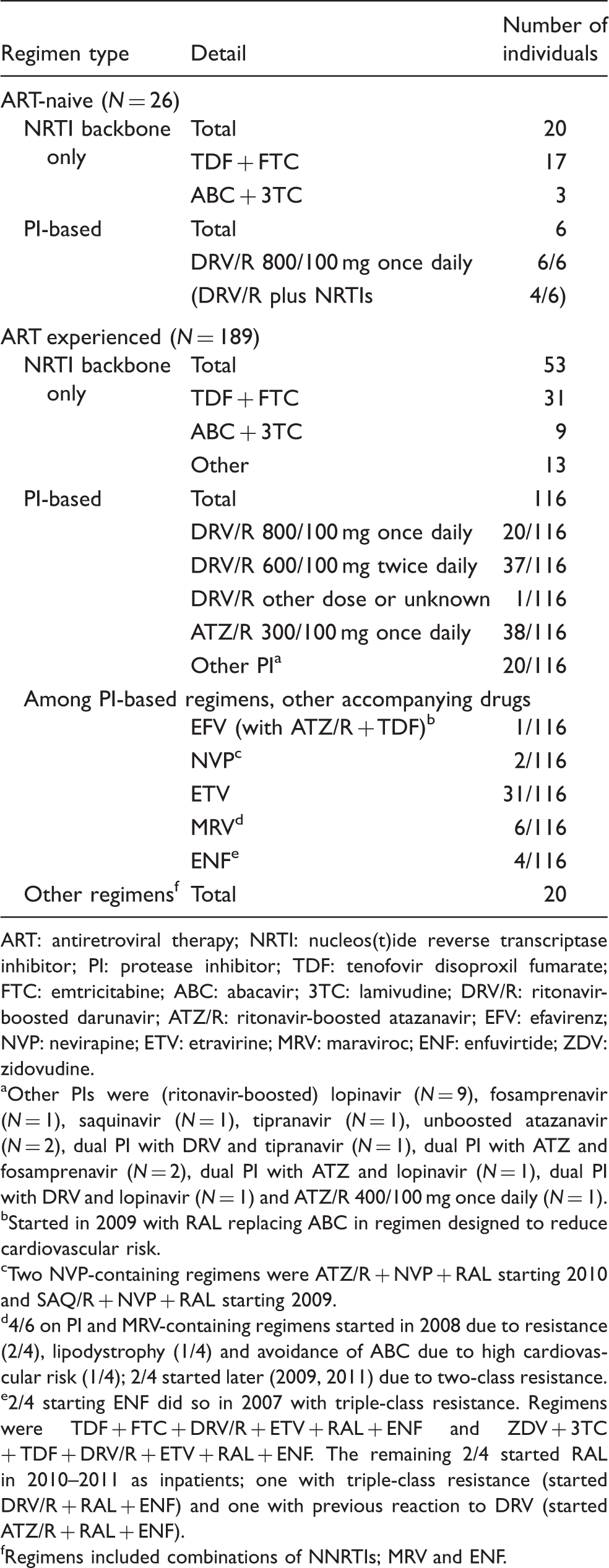
ART: antiretroviral therapy; NRTI: nucleos(t)ide reverse transcriptase inhibitor; PI: protease inhibitor; TDF: tenofovir disoproxil fumarate; FTC: emtricitabine; ABC: abacavir; 3TC: lamivudine; DRV/R: ritonavir-boosted darunavir; ATZ/R: ritonavir-boosted atazanavir; EFV: efavirenz; NVP: nevirapine; ETV: etravirine; MRV: maraviroc; ENF: enfuvirtide; ZDV: zidovudine.
Other PIs were (ritonavir-boosted) lopinavir (N = 9), fosamprenavir (N = 1), saquinavir (N = 1), tipranavir (N = 1), unboosted atazanavir (N = 2), dual PI with DRV and tipranavir (N = 1), dual PI with ATZ and fosamprenavir (N = 2), dual PI with ATZ and lopinavir (N = 1), dual PI with DRV and lopinavir (N = 1) and ATZ/R 400/100 mg once daily (N = 1).
Started in 2009 with RAL replacing ABC in regimen designed to reduce cardiovascular risk.
Two NVP-containing regimens were ATZ/R + NVP + RAL starting 2010 and SAQ/R + NVP + RAL starting 2009.
4/6 on PI and MRV-containing regimens started in 2008 due to resistance (2/4), lipodystrophy (1/4) and avoidance of ABC due to high cardiovascular risk (1/4); 2/4 started later (2009, 2011) due to two-class resistance.
2/4 starting ENF did so in 2007 with triple-class resistance. Regimens were TDF + FTC + DRV/R + ETV + RAL + ENF and ZDV + 3TC+ TDF + DRV/R + ETV + RAL + ENF. The remaining 2/4 started RAL in 2010–2011 as inpatients; one with triple-class resistance (started DRV/R + RAL + ENF) and one with previous reaction to DRV (started ATZ/R + RAL + ENF).
Regimens included combinations of NNRTIs; MRV and ENF.
Prior ART use
Previous ART use among 186 ART-experienced individuals starting raltegravir.

Note: NRTIs = nucleos(t)ide reverse transcriptase inhibitors; nNRTI = non-nucleoside reverse transcriptase inhibitors.
Reasons for stopping raltegravir
During this time period, 68 individuals stopped raltegravir (Figure 2). Among 18 individuals stopping raltegravir for toxicity reasons, one had acute hepatitis considered to be due to raltegravir, with alanine transaminase (ALT) levels increasing from 22 U/L at baseline to 540 U/L on day 30 of treatment. This Caucasian male was hepatitis B- and C-negative and raltegravir 400 mg twice daily was co-administered with tenofovir and ritonavir-boosted atazanavir, after resistance mutations were detected during a blip on tenofovir, abacavir and ritonavir-boosted atazanavir. Three individuals had headaches attributed to raltegravir and two stopped due to potential drug reactions (one, admitted with rash, angioedema and raised transaminases [ALT 314 U/L], with Epstein-Barr viraemia was taking darunavir/ritonavir concurrently with raltegravir and all drugs were stopped; the second was known to have multiple drug allergies and stopped raltegravir due to a rash, while also taking enfuvirtide and atazanavir/ritonavir).
Reasons for stopping raltegravir in 68 individuals who stopped during the period reviewed. AMA = against medical advice.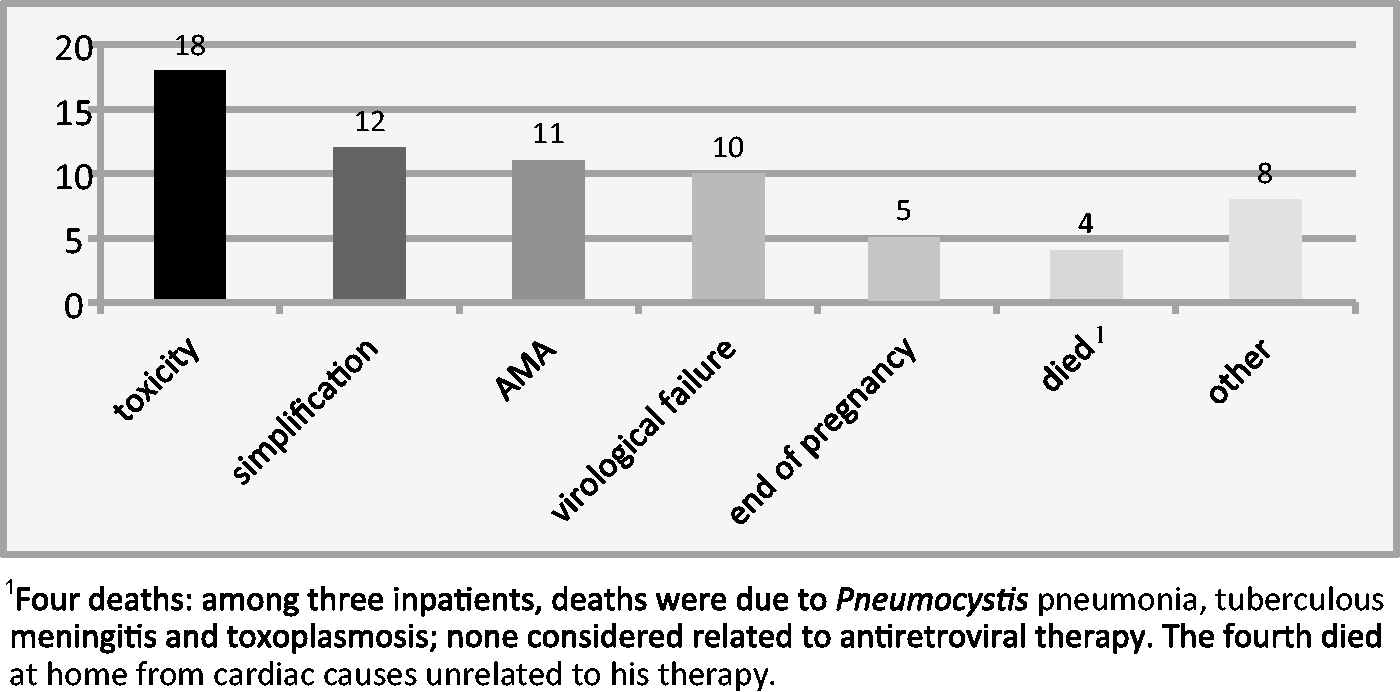
Twelve individuals stopped raltegravir for simplification, of whom four had taken raltegravir to avoid DDIs with antimycobacterial or antifungal treatment and stopped once those treatments were completed; two stopped on receipt of a resistance test permitting simplification; two had undetectable VL on PI-based regimens for several months and the stop was physician initiated and the remaining four requested simplification. Four individuals died (Figure 2). Among three inpatients, deaths were due to Pneumocystis pneumonia, tuberculous meningitis and toxoplasmosis; none considered related to ART. The fourth died at home from cardiac causes unrelated to his therapy.
Hepatitis co-infection
Thirty-five individuals with hepatitis B or C infection provided 92 patient-years of raltegravir use. Of these, 21 were positive for hepatitis B surface antigen (HBsAg) and 14 positive for hepatitis C RNA. The median ALT at baseline was 29 U/L, with range of 8–179 U/L. None stopped raltegravir due to hepatotoxicity.
Of 21 HBsAg-positive individuals, 19 were taking tenofovir-containing regimens and two took entecavir along with suppressive ART as tenofovir was contraindicated due to renal disease. Of 14 individuals with hepatitis C infection, three took pegylated interferon-alpha and ribavirin for hepatitis C while on raltegravir. None in this time period took directly-acting antivirals for hepatitis C.
Mycobacterial co-infection
Twenty-two individuals used raltegravir during treatment for mycobacterial co-infection, of whom 13/22 (59.1%) were female and 17/22 (77.3%) were Black African. The median CD4 count at the time of starting raltegravir was 83 cells/mm3 (IQR 23, 229) and, among 11/22 not on ART, median VL was 109,833 copies/mL (range 7766, 8,647,191). Three had known K103N mutation and one had G190S at baseline. Fourteen individuals were inpatients at the time of starting raltegravir and eight were ART naive.
The majority had M. tuberculosis (18/22 [81.8%]), including three with tuberculous meningitis and five with disseminated disease. Four (18.1%) had M. avium complex bacteraemia. Of the 22 individuals, 19 were taking rifampicin and two were taking rifabutin concurrently with raltegravir, while one was taking other antimycobacterial drugs for M. avium complex. Raltegravir was dosed at 800 mg twice daily in 13/18 with M. tuberculosis and 400 mg twice daily in five, and two of them commenced 800 mg twice daily then reduced after therapeutic drug monitoring. Only one stopped raltegravir due to side effects (peripheral neuropathy while also taking isoniazid) and two, one of whom had virological failure, switched therapy due to concerns about adherence and barrier to resistance. One individual with tuberculous meningitis died six weeks after starting raltegravir.
Pregnancy
Of six women taking raltegravir during pregnancy, one switched from a PI-based regimen for tolerability reasons affecting adherence and five started raltegravir to intensify PI-based regimens at median 32 weeks gestation (range 21–37 weeks, with the woman starting at 21 weeks previously taking ritonavir-boosted lopinavir only due to tolerability and extensive reverse transcriptase mutations). All six women had undetectable HIV RNA at delivery and all infants were HIV-negative with no foetal abnormalities.
Once-daily dosing
Once-daily (OD) raltegravir (800 mg) in ten ART-experienced individuals.

Blip = detectable viral load <400 copies/mL, which is preceded and followed by an undetectable result without any change in therapy (ref BHIVA ART GL).
On once-daily raltegravir, 4/10 stopped all ART against medical advice; one stopped due to virological failure with poor adherence after 26 months; one stopped raltegravir for simplification after 27 months and four remained suppressed on raltegravir-containing once-daily regimens after a median of 28 months.
Virological failure
Of 215 individuals, ten (4.7%) stopped raltegravir because of virological failure: of these, the HIV-1 integrase region was successfully sequenced in four and the remaining six had low-level viraemia precluding sequencing or failed sequencing. Two of the four individuals showed evidence of INSTI resistance after virological failure. The first had Q148R, on a background of pre-existing triple-class resistance; the second had Y143R, with pre-existing M184V, Y115F and major protease mutations. The two individuals without evidence of INSTI resistance had no pre-existing mutations in the reverse transcriptase or protease regions. Concerns about adherence were documented in 4/10.
Discussion
Data from this large, diverse group, taking raltegravir in the first five years of its availability, support raltegravir’s safety and efficacy, without apparent toxicity above that was found in clinical trials. It was used without complications in pregnancy and in co-infection. In our experience, once-daily dosing was effective where adherence was good, but caution is required where adherence is poor. INSTI resistance mutations occurred in those failing raltegravir with pre-existing resistance to other ART classes.
ART-naive individuals starting raltegravir had low CD4 counts and many were inpatients, using raltegravir for rapid VL reduction.2,3 Raltegravir is now among preferred first-line agents in ART-naive individuals, 5 so this scenario may become less typical of ART-naive individuals, as more choose raltegravir as outpatients with higher CD4 counts. Raltegravir has been especially useful in avoiding DDIs when managing co-infections.
Off-license use of raltegravir in pregnancy has shown to be successful in that it contributed to virological suppression and good outcomes were observed for all pregnancies. These data support previously published reports of raltegravir use in pregnancy6–10 and the current BHIVA guidelines. 11
Tolerability was good, with relatively few side effects; only one patient stopping due to hepatitis and three due to headaches, consistent with clinical trial data.2,3 INSTI resistance mutations were detected on virological failure where there was pre-existing resistance to other classes.
The main limitation of this study is its retrospective nature, relying on routine clinical records for data. Virological monitoring was done according to individual patient and physician-agreed schedules and broadly in line with BHIVA guidelines 12 during the time they were in place but was not regular enough meaningfully to employ the type of analysis of efficacy end points used in clinical trials. Analysis and conclusions are also somewhat limited by the inclusion of one centre and it is the patient group and information obtained may have been incomplete. However, as a description of routine use of a first-in-class antiretroviral agent, the study benefits from the large numbers included and relatively long follow-up.
In conclusion, raltegravir has been used for individuals with very advanced HIV infection and for both ART-naive and ART-experienced individuals and patterns of use may change over time. It appears to be safe and effective in our practice. These real-life data, including off-license use, add usefully to clinical trial results and contribute to understanding of the role of raltegravir in clinical practice.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CvH has received educational grant funds from Merck, Sharp & Dohme Ltd; AT has received advisory board fees from Merck, Sharp & Dohme Ltd.; AU has received speaker and advisory board fees from Merck, Sharp & Dohme Ltd.; TW, NL, KM declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Materials
Original data and data collection tools can be obtained by contacting the corresponding author.