
Abstract
This quasi-experimental, before–after study was designed to assess the effect of an educational intervention on knowledge and attitudes about sexually transmitted infections, HIV and preventive behaviours among female sex workers in Shiraz, Iran. A single-group pre–post test design was used and the study was done between August and December 2009. The participants were 80 female sex workers recruited from three drop-in centers in Shiraz, with stratified random sampling. Pre-intervention knowledge was assessed by interview with a standard questionnaire. The educational intervention consisted of a lecture, face-to-face education, printed information, an educational movie, role playing and a contest. After 2 months, the effect of the intervention was evaluated (post-test). The average age of the participants was 32.6 ± 9.1 years. After the intervention, the mean score for general knowledge about HIV and sexually transmitted infections increased from 13.7 ± 0.95 (pre-test) to 19.47 ± 11.62 (post-test, p < 0.001). There were significant improvements in attitude and the number of participants who self-reported preventive behaviours such as using a condom consistently (from 45 to 63) (p < 0.001). The results show that the educational programme was successful in increasing the participants’ HIV- and AIDS-related knowledge and attitudes, and in decreasing their risk behaviours.
Keywords
Introduction
According to the Iranian Ministry of Health, the HIV epidemic is in the concentrated phase and about 23,000 HIV/AIDS cases have been registered as of November 2011. 1 In Iran, cases of HIV infection in the current epidemic are reported mainly among high-risk groups such as injection drug users, although there is evidence that the mode of transmission is shifting towards sexual contacts. 2
Female sex workers are potential carriers and represent an important source of sexually transmitted infections (STIs) including HIV, and they can transmit HIV to clients and indirectly to the general population. Studies have shown that 20% to 48.8% of female sex workers had more than one kind of sexually transmitted infection. However, the rates of HIV infection were found to be generally lower than for other types of STI. 3 The results of one study of female sex workers in Kerman, Iran, showed that the weighted prevalence of syphilis and HSV2 were 7.2% and 18.0%. 4 In another study of 279 female sex workers in Shiraz, Iran, 13 (4.65%) of the women were HIV-positive and the prevalence of syphilis, chlamydia infection, gonorrhoea and herpes were 0%, 9.7% (27), 1.4% (4) and 9.7% (27), respectively. 5
STIs are considered one of the main factors that facilitate the transmission of HIV infection. Syphilis and genital ulcers such as herpes, transmitted through sexual contact, increase the vulnerability to HIV infection. 6 Risky sexual behaviours such as a history of sex with multiple partners and inconsistent condom use also increase the risk of HIV infection among female sex workers. 7
A key component of all AIDS control programmes is the modification of risky sexual behaviours by reducing the numbers of sexual partners and increasing condom use. Such programmes often increase knowledge about AIDS and how to prevent HIV infection, and improve attitudes towards infected persons; however, evidence for sustained behavioural change is lacking. Exceptions in this regard are programmes that focus on high-risk or vulnerable groups, in particular groups of men and women with multiple sexual partners. Many such programmes focus on female sex workers. 8 The results of one study that evaluated the effect of a peer education programme for female sex workers showed that in trained clusters, there were higher levels of AIDS knowledge, STI knowledge and condom use. 9 Another intervention programme was shown to increase knowledge of the routes of HIV transmission, knowledge that condoms can reduce the risk of STI/HIV infection and condom use. 10 Both studies showed that the intervention programme was effective at increasing HIV/AIDS knowledge and condom use rates among sex workers.
The prevalence of STIs and HIV in female sex workers suggests a critical need for preventive efforts and health education. In addition, the results of some studies in Thailand, Cambodia and Vietnam have shown that successful preventive intervention programmes for STI have had a major impact in reducing the spread of HIV.11–13
The first step in health education is awareness; subsequent changes in attitudes and beliefs can eventually lead to changes in behaviour. Health education is one of the main parts of any health activity. The effectiveness of educational programmes requires recognizing the factors that influence behaviour in order to modify existing behaviours and replace them with new behaviours.14,15 To achieve this, health policy makers in Iran are considering the harm reduction approach in response to the increased risk of HIV infection. This approach includes all actions that will reduce high-risk behaviours. The National Committee on Harm Reduction, in order to achieve the goals of current harm reduction strategies, has established drop-in centres in high-risk districts. These centers provide a place where homeless people with high-risk behaviours can rest, and offers harm reduction services including various educational programmes, peer-group education and enrichment of leisure time activities, and provides referral letters for free counseling and therapy. 16
In recent years, numerous governmental initiatives in Iran have been undertaken in order to control the HIV/AIDS epidemic. These efforts include promoting public awareness, reducing the vulnerability of high-risk groups through voluntary counseling and testing centres, and education through the mass media as symptomatic approaches to STI, but particular high-risk groups for HIV/STI such as sex workers have not been the main focus of published research. 17 To the best of our knowledge, no evidence has been published about HIV/STIs awareness and prevention in female sex workers in Iran. We therefore designed this study to examine the effect of an educational intervention on knowledge and attitudes of female sex workers referred to three urban academic drop-in centers in Shiraz.
Methods
Setting and population
From August to December 2009, a quasi-experimental before–after study with a single-group pre–post test design was carried out. The intervention consisted of a health education programme. All female sex workers referred to services from harm reduction centers affiliated with Shiraz University of Medical Sciences (Bayat and Saadi districts and the Marvdasht center) comprised the study population. These three drop-in centers for vulnerable women have been operating since 2008 in Fars province and provide harm reduction services such as condom distribution, methadone therapy, needle exchange and gynaecological examination. The women also benefit from other facilities such as showers and a daily hot meal at these centres.
Design
A sample size of 80 female sex workers was recruited based on stratified random sampling. Initially, the three drop-in centres were selected as subgroups (strata) and the real proportion of samples for each center was calculated based on total sample size; then participants at each center were selected with systematic random sampling. The inclusion criteria were engaging in commercial sex work for at least 1 month and being HIV-negative.
Measures
The data collection tool was a questionnaire prepared and designed on the basis of review articles, theses, Persian sources, previous questionnaire studies and a translation and adaptation of the HIV, AIDS and STI questionnaire developed by Family Health International for behavioural surveillance 18 based on the PRECEDE model. The PRECEDE model is an educational model that focuses on factors that influence health-related behaviour, based on the relationship between the health professional and the patient. This model considers the influence of three factors on health-related behaviour. Predisposing factors are those that influence the patient’s motivation to undertake the behaviour to be analyzed or encouraged and are subjective (beliefs, opinions, values, thoughts, knowledge). Facilitators are factors that influence the level of ease or difficulty the patient and his/her family has in undertaking a given behaviour. Reinforcing factors are those that arise after the patient has undertaken the behaviour, and which reward or punish it. 19
The questionnaire consisted of two parts: the first contained six demographic questions and the second consisted of 34 questions about knowledge, 12 questions about attitudes and 6 questions related to behavioural factors. For the items about knowledge and behavioural factors, the three response categories were yes (1 positive point), no (1 negative point) and don’t know (0 points). The three possible responses for questions regarding attitudes were agree (2 points), no idea (1 point) and disagree (0 points). The total STI/HIV knowledge index was estimated by summing the scores for all 34 items (yes, no, don’t know; scored, respectively, as 1, −1 and 0). The total attitude index was estimated by summing the scores for 12 items on a 3-point Likert scale (disagree, no idea, agree; scored, respectively, as 0, 1 and 2). The items related to behavioural factors were used to obtain information about preventive behaviours, reasons for the lack of regular medical examination and reasons for not using condoms. Preventive behaviours were compared before and after the intervention on the basis of female sex workers’ self-reports regarding whether they engaged in specific behaviours. The item used to obtain this information was the question, “Which of the following behaviours do you currently engage in to prevent the transmission of HIV/STI?”
To verify content validity, comments were requested from expert faculty members at Shiraz University of Medical Sciences. A panel of experts consisting of four faculty members and scholars in the areas of health behaviour and education assessed the content validity of the instrument by evaluating the appropriateness and relevance of the items, face validity and response format. The feedback from the panel of experts was used to revise and modify the instruments. In addition, in a pilot study of 30 female sex workers, a Cronbach’s alpha coefficient of 0.85 (range 0.78 to 0.92) was calculated as evidence of the internal reliability of the total questionnaire, with α = 0.80 (range 0.73 to 0.86) for knowledge, α = 0.59 (range 0.43 to 0.74) for the behavior subscales and α = 0.75 (range 0.66 to 0.82) for the attitudes/perception subscale.
In order to gain the participants’ cooperation, an introductory meeting was held in an informal atmosphere at each centre to explain the objectives of the project and assure the women that all questionnaire information and research results would remain confidential. The women were informed that they could withdraw from the study at any stage and they would receive an incentive at the end of the study. The staff members at the harm reduction centres cooperated in the study, and all questionnaires were completed by educated peers in a safe, private place. A code was allocated to each participant to ensure anonymity.
Intervention
The educational sessions for women were designed to (1) increase their knowledge of HIV/STI, (2) increase their perceived susceptibility to HIV/STI, (3) improve skills related to condom use and partner negotiation and (4) increase awareness of STI symptoms and the need for STI screening and treatment. The educational intervention provided information about STI, symptoms, complications, risk factors, ways to prevent STI and negotiating skills. At each centre, the interventions took place in two sessions in the morning and evening of the same day, with lecture, question-and-answer, group and face-to-face discussion, role-play and a contest. Printed information was distributed and video material was also shown. The later sessions extended the discussion of STI, condom use and negotiation about condom use. Women were encouraged to visit the clinic to obtain treatment for genital symptoms. In addition, participants took part in a role-play exercise to practice their negotiating skills regarding condom use with clients. The first session dealt mainly with informational issues about AIDS, STI and the symptoms of illness. All the participants (100%) completed both sessions.
After 2 months, all participants were contacted during a 1-week period according to their participant code and contact information, and the post-test study was done in the same setting and in small groups at the three centres as for the intervention. This phase of the study was facilitated by the fact that the women were usually referred to the same centres for routine services.
Statistical analysis
Independent t-test, paired t-test, one-way ANOVA, Pearson correlation coefficient and the McNemar test were used for data analysis. All tests were done with SPSS v. 13 software and differences of 0.05 or less were considered significant.
Ethical aspects
This study was approved by the ethics committee of the Tehran University of Medical Science, and informed consent was obtained from all the women who were willing to participate in the study.
Results
All 80 participants initially enrolled remained in the study for its duration. The average age of the women who participated in the study was 32.62 ± 9.11 years. 38 were in the 15- to 30-year age group (47.5%), 46 (57.5%) were married, 77 (96.3%) were unemployed and most had primary or secondary school education (91.3%). Below we report the findings for the changes in participants’ knowledge level for different aspects of STI, HIV and preventive behaviours.
Types of STI
Knowledge of the type of transmission of HIV and STI before and after the educational intervention in 80 female sex workers in Shiraz, Iran.
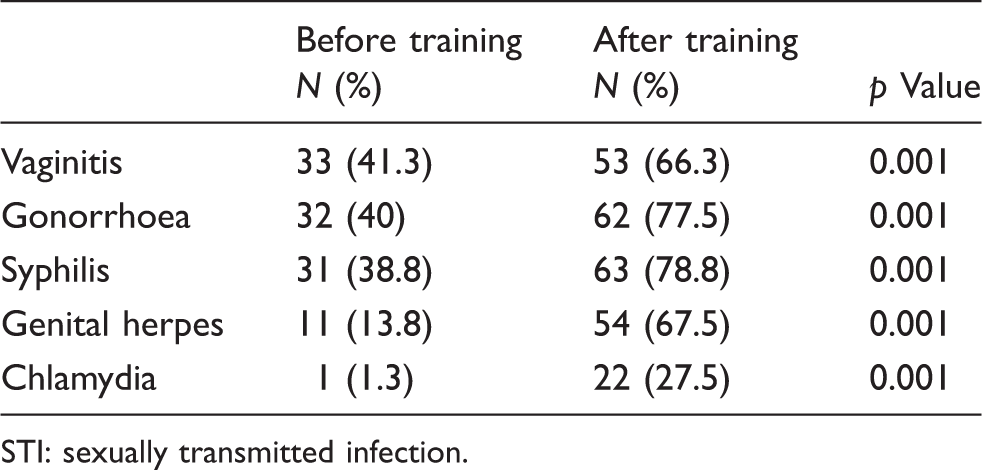
STI: sexually transmitted infection.
Symptoms of STI
Knowledge of the mode of transmission of HIV and STI before and after the educational intervention in 80 female sex workers in Shiraz, Iran.
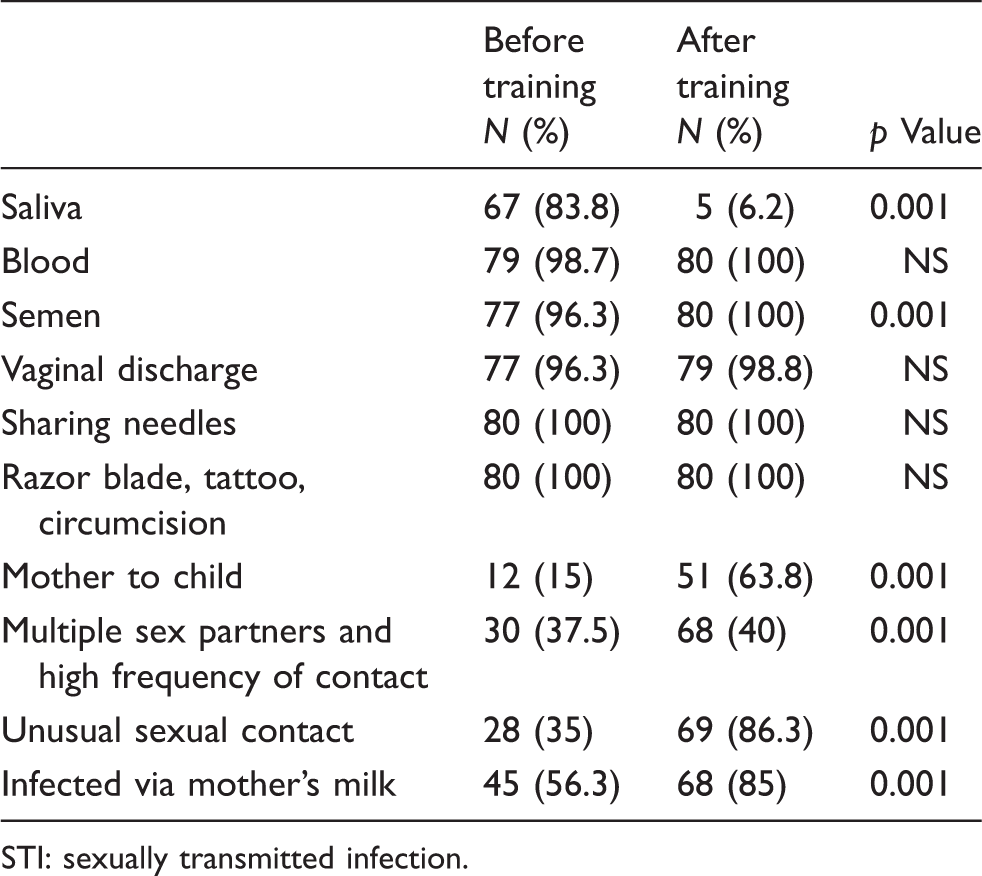
STI: sexually transmitted infection.
Complications of STI
Knowledge about the complications of STI including genital cancer (36.3%) and morbidity and mortality (31.3%) was low. None of the participants was aware of other complications such as ectopic pregnancy, infertility and sterility or neonatal malformations. After the intervention, the participants’ knowledge of all complications increased (p < 0.0001).
Mode of transmission
Before the intervention most women had a good level of knowledge about the mode of transmission of HIV and STI via the blood (98.7%) and through substance abuse (100%). However, the number of women who had lower awareness of these issues decreased after the intervention (Table 2). At the beginning of the study, 15% of the participants were aware of HIV/AIDS transmission from the pregnant mother to the child. About 56.3% knew that infection can be transmitted via the mother’s milk, 35% were aware of transmission via unconventional sexual contact and only 37.5% knew that having multiple sexual partners can lead to HIV infection. After the intervention, the rates of knowledge increased to 86.3% for unconventional sexual contact, 85% for mother’s milk, 63.8% for pregnant mother to the child and 60% for multiple sexual partners (p ≤ 0.001).
Knowledge of ways to prevent HIV and STI transmission before and after the educational intervention in 80 female sex workers in Shiraz, Iran.
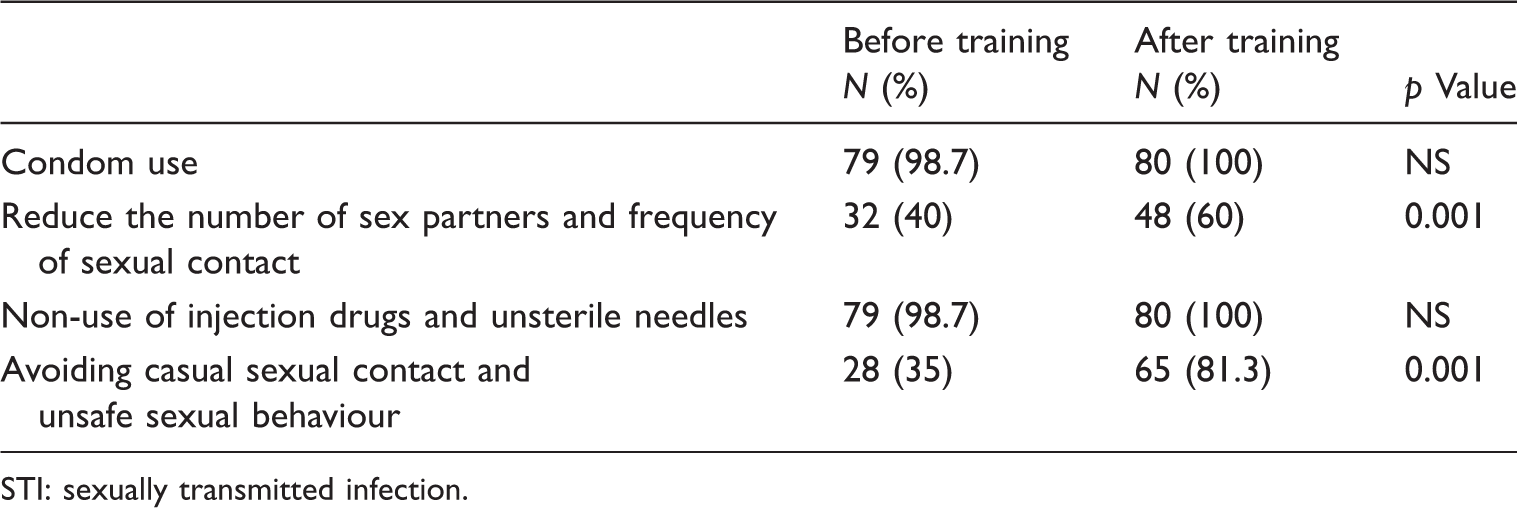
STI: sexually transmitted infection.
Comparison of mean differences in the knowledge about HIV and STI before and after the educational intervention in 80 female sex workers in Shiraz, Iran.
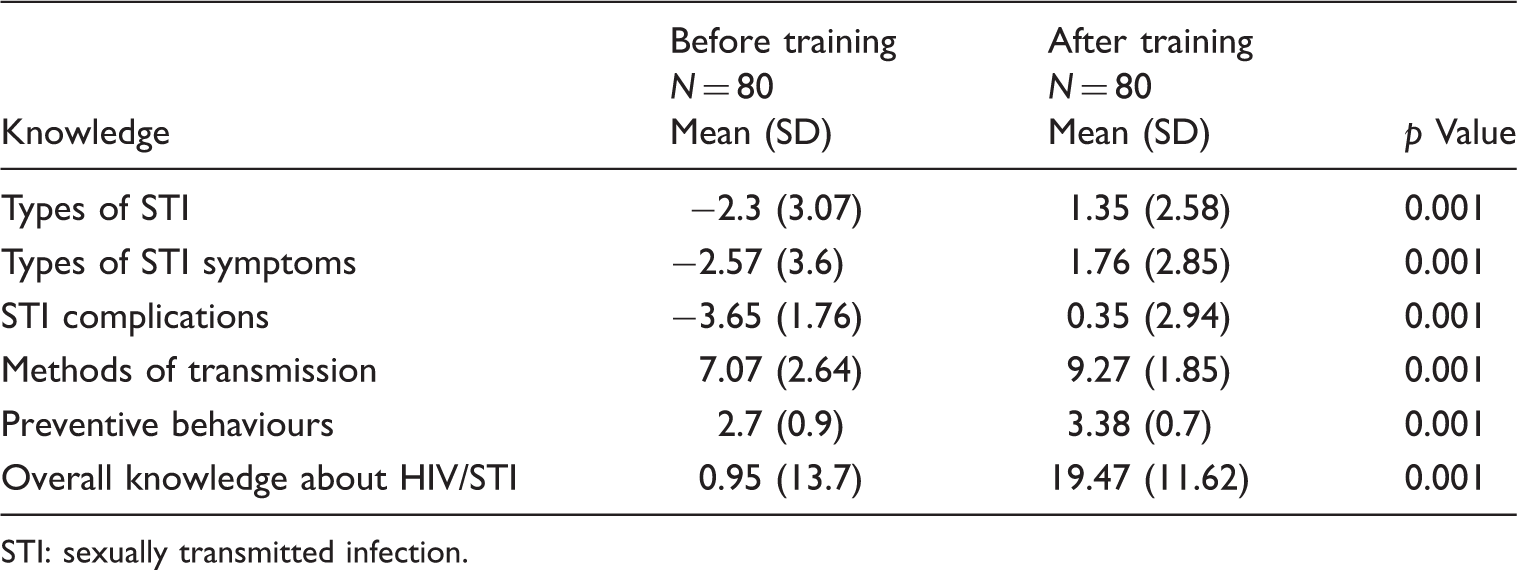
STI: sexually transmitted infection.
At the start of the study, 43 women (53.8%) believed that HIV/AIDS is controllable, and after the intervention this number increased to 76 (95%). Only 18 (22.5%) women believed in treatment for themselves and their partners. After the intervention, 48 participants reported a positive attitude toward the benefits of treatment (60%). Before the intervention, 58 (72.5%) women had volunteered to take an HIV test, but after the educational intervention, 73 (91.3%) were willing to take this test.
According to the McNemar test, before the intervention, 51.2% of women had a neutral attitude and 48.8% had a positive attitude toward different aspects of HIV/AIDS such as method of prevention, transmission mode, public school attendance for infected children, free counseling for HIV-positive individuals at public centres and ostracism by family members. In the post-test, these proportions changed to 5% and 95%, respectively.
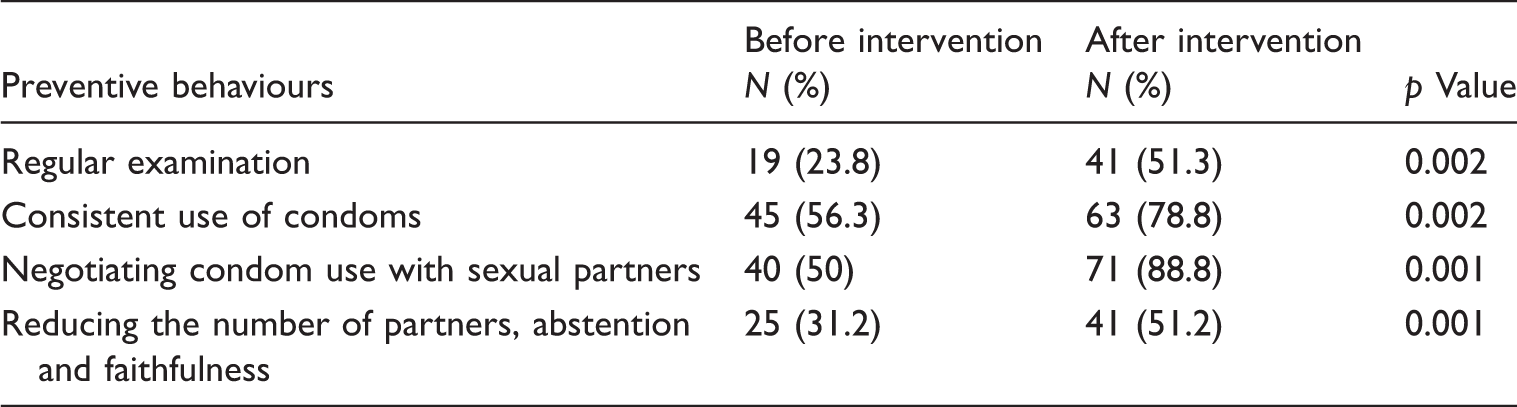
Distribution of preventive behaviours in 80 female sex workers in Shiraz, Iran.
The result of ANOVA showed no significant differences in that the association between knowledge with educational level and income level. In addition, there was no correlation between age and knowledge score. However, a significant association was found between marital status and mean knowledge score (p < 0.001).
Discussion
Inadequate knowledge regarding STI in groups exposed to risk such as women with high-risk sexual contacts is a well-known problem that requires serious planning efforts. With widespread publicity about the importance of AIDS, other STI have been overshadowed. This study focused on the first intervention in Iran designed to enhance STI/HIV-related knowledge, attitudes and preventive behaviours in female sex workers. Overall, the results indicated that educational intervention was effective in our study sample.
Many women were knowledgeable about HIV/AIDS. In contrast, the results showed that on average, only about one-third of the participants were aware of STI and about 24% of the women were aware of the symptoms of STI (burning pain during urination, genital sores, genital discharge, abdominal pain, swelling and itching in the groin) before our educational intervention – a relatively low awareness level.
One earlier study found that only 30.5% of the participants knew the symptoms of STI and only 40% knew about the serious complications of STI. 16 A 1996 study by Lupiwa et al. 20 on rural women’s awareness of STI found that most women knew little about their disease. Some had even thought the signs and symptoms were normal and most were unaware of the complications of STI. 20 The findings of these studies in terms of low levels of awareness about STI are consistent with the results of the present study.
Another study showed that general awareness about the main transmission routes of HIV was high in most cases. More than half (55.5%) of the women said that transmission could be avoided by having only one noninfectious sexual partner, using condoms, a lower frequency of sexual contacts and avoiding anal sex. 15 A study of 241 female sex workers in Italy found that almost all of them had heard about AIDS and syphilis, but their information about other STI was inadequate. 21 These findings also are consistent with ours. As in our study, the results of another study showed that most of the women had heard about AIDS but their awareness of STI was very low. 22
In one study of 525 girls and women, all participants had heard about AIDS and had some knowledge of its transmission. 23 In our study, almost all women had heard about AIDS. The findings of another study showed that education increased the average scores for awareness of HIV and STI in a group of prisoners. 24 In similar studies, the results were consistent with our finding of a significant difference between pre-test and post-test scores after health education; these results are evidence that the intervention was effective in raising awareness in the study population.25,26 Jean and colleagues designed an educational program for imprisoned women based on lectures, question-and-answer sessions and video presentations. A significant increase in the participants’ awareness of ways to reduce risky behaviours related to AIDS and STI was seen after the educational intervention. 26
A review in China documented the positive effects of behavioural interventions in HIV/AIDS in female sex workers. Most intervention strategies included training to improve awareness about HIV and behavioural skills such as the use of protective devices, less needle sharing and ways to reduce the rate of STI. 27 In the present study, the educational intervention increased the rate of regular condom use from 56.3% to 78.8%. In a similar study of 1079 female sex workers, 38% used a condom correctly and consistently for frequent relationships, whereas condom use with an intimate friend was low. 28 The results of similar studies have shown increased rates of condom use after training, which indicates the effect of educational programmes on behaviour.29,30 In another study, condom use among female sex workers increased after education, and 41% of the women stated that if their customers refused to use condoms correctly they would not have sex with them. 31 The results of previous studies are consistent with our finding that the rate of correct regular condom use after the learning intervention was better than before training.
The women in the present study reported that the main reasons for failing to seek regular examinations for STI were fear of the examination, inability to pay, lack of disease symptoms and lack of susceptibility to disease. Another study of normal women found that only 23% of the women were referred for examination. The main reasons for nonreferral in 70% of the participants were embarrassment, pain during the examination, lack of symptoms, lack of awareness of the importance of regular examinations and not being prone to STI. 32
Future interventions should be designed to take place at an appropriate time and in a suitable setting in order to improve and consolidate learning. To improve HIV-related knowledge and attitudes and prevent high-risk behaviours, health education should be considered a fundamental element at harm reduction centres. Because many health problems are interconnected with life style, health educators can play an important role in promoting healthy behaviours. On a broader level, educational interventions need to be developed for specific at-risk populations such as immigrants, seasonal workers, sex workers and their customers, and injection drug users.
The study had several strengths and limitations. To the best of our knowledge, ours is the first study in Iran to investigate and analyze HIV- and STI-related knowledge, attitudes and behaviours in female sex workers, and to test the effects of an educational intervention in promoting safe behaviours in this hard-to-study population. The other strength of this study was the high rate of successful follow-up. None of the women dropped out during the study process, and we attribute this to several reasons. Our study was done at three different centres, and this facilitated contacts and communication with small groups of 5 to 10 participants. The greatest problems were encountered at the largest centre (Bayat centre, with 40 participants), where an additional challenge was the need to increase the duration of the educational interventions to 4 days. Usually about 220 female sex workers attend these centres daily to obtain free medical care services and other types of support including a hot meal, receiving condoms and needle exchange, so it was not hard to contact potential participants. Collaboration among researcher and staff members was excellent. The interviewers were peers (female sex workers who work at the centres), and this facilitated communication with the participants. All participants were aware of receiving incentive at the end of study.
One of the most important limitations of this study was the single-group pre–post test design, in which it was not possible to use a control group. This design was used because our sample was from a hard-to-reach population. Although this design was appropriate for the characteristics of this research, the lack of a control group means that our findings should be considered with due caution. In other words, other as yet unidentified factors in addition to the intervention we studied may have contributed to the changes we observed in the post-test results. Another limitation is that in an interview, the accuracy of self-reported behaviours is difficult to evaluate since there is no true gold standard. This factor may limit the external validity of some of our findings.
Another factor that may have affected some of our results is addiction and methadone maintenance therapy in some participants, which may have had a negative effect on their learning since substance abuse and maintenance therapy can slow the flow of training. Because of privacy and confidentiality issues, other factors that may have affected our findings could not be studied in depth, and this constitutes another potential limitation. Individual differences in learning can influence the effects of educational interventions, and thus need to be taken into consideration in assessing our results. These reasons as well as suboptimal decision-making in emotional situations can reduce some participants’ use of preventive behaviours, despite their increased knowledge.
Conclusions
The present study shows that the educational intervention we tested led to increases in female sex workers’ knowledge about HIV/AIDS and STI, and improved their ability to reduce risky behaviours and health problems. Such training plays a key role in the control and prevention of STI and AIDS. The results of the pre-test questionnaire showed that the most important source of information was the peer group. An appropriate teacher who is accepted by the target group and is a trusted, effective communicator is essential for peer group education. Members of the peer group understand the economic and social pressures that these women endure, but their knowledge of behavioural theory is limited. Sources of information can be strengthened through educational interventions. The results of this study can be used to plan sexual health education, prevent STI and provide effective sexual health services to vulnerable women. Our findings point to the need for educational interventions in female sex workers as a core group for HIV transmission. In particular, our study can encourage policy makers to consider educational programmes as a key component of strategies for reducing the risk of HIV transmission in the wider population.
Footnotes
Acknowledgments
This study was part of an MS dissertation supported by Tehran University of Medical Sciences (grant number 735p). We thank Dr H Joulaei, former Deputy Vice-Chancellor for Health Affairs of Shiraz University of Medical Sciences, Dr AR Hasanabadi and the staff of the voluntary counseling center of Shiraz University of Medical Sciences. We greatly appreciate the efforts of the women who participated in this study. We also thank K Shashok (Author AID in the Eastern Mediterranean) for improving the use of English in the manuscript.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.