
Abstract
To better understand the behavioural characteristics and the factors associated with high risky behaviours among men who have sex with men and women (MSMW) with different orientation, we analyzed data from a cross-sectional survey of 600 MSMW in two large cities in China. Participants completed a questionnaire and underwent serological testing. Overall, human immunodeficiency virus (HIV) prevalence was 26%. In multivariable analysis of risk factors for unprotected anal intercourse in the past six months, factors associated with unprotected vaginal intercourse (UVI) were as follows: gay-identified orientation, having anal sex with a boyfriend, having multiple male partners, and never or sometimes using a condom for vaginal intercourse. In multivariate analyses of risk factors for UVI in the past 12 months, factors associated with UVI were as follows: non-gay-identified MSMW, having multiple male partners, having multiple female partners, and never or sometimes using a condom for anal intercourse. This study revealed a high prevalence of HIV and risky sexual behaviours.
Keywords
Background
The rise of human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) prevalence among men who have sex with men (MSM) in China has been well documented.1,2 According to the Chinese Ministry of Health, 108,780 MSM were living with HIV/AIDS by the end of 2009, accounting for 15% of the total estimated HIV cases in China. 1 Among the approximately 50,000 new HIV infections in 2007, 12% were attributable to male same-sex behaviours 2 and this estimate increased to 33% of newly acquired HIV infections in 2009. 1 A meta-analysis of studies on trends in HIV prevalence among MSM in China revealed an increase from 1.4% (0.8–2.4%) during 2001–2003, to 2.3% (2.0–2.6%) during 2004–2006, to 5.3% (4.8–5.8%) during 2007–2009; the sharpest rise was observed among MSM in the southwest region, where HIV prevalence was 11.4% in 2009. 3
Because of traditional social norms in China, same-sex behaviours are often considered unacceptable and MSM experience social pressures to conform to heterosexual standards. 4 A strong social pressure among MSM arises from family expectations for these men to marry and have children. 5 Many MSM have female partners such as wives and girlfriends, yet also engage in sex with male partners.6,7 Several studies have revealed that, among MSM in China, the prevalence of bisexual behaviours is considerably high and unprotected vaginal sex is relatively common.8–10 A meta-analysis of research on MSM in China revealed that 17% of MSM were currently married to women and 26% of MSM reported sex with both men and women. 8 A survey conducted in Yunnan Province found that among 896 MSM, one-third had ever been married and 31% had engaged in bisexual behaviours in the past six months; of men who have sex with men and women (MSMW) in the sample, 72% reported unprotected vaginal sex with female partners in the past six months. 9 Previous research has also found that married MSM report significantly higher rates of unprotected insertive anal, receptive anal, and vaginal sex compared with unmarried MSM. 10 The epidemiological bridge associated with bisexual behaviours among MSMW may accelerate transmission of HIV and other sexually transmitted infections in the general population.
Previous studies in China have compared HIV prevalence and sexual behaviours between MSM and MSMW.11–13 A consistent finding is that MSM and MSMW show few differences in the rate of condom use for anal sex, and that MSMW use condoms less frequently for heterosexual behaviours than for homosexual behaviours. One study found that Chinese MSMW were less likely to have been HIV tested and exposed to HIV prevention activities compared with MSM, 13 which corresponds with findings from MSMW in the United States.14,15
However, relatively little is known about whether HIV risk among MSMW varies according to how these men identify their sexual orientation. Studies have indicated that there is diversity in how MSMW identify their sexual orientation, with some who identify primarily as gay or homosexual and others who identify as heterosexual, or bisexual, or who do not identify according to any sexual orientation identity. 16 Evidence from research with MSMW in the United States suggests different behavioural risks between men who are gay-identified versus non-gay-identified MSMW. 17 Moreover, because HIV prevention programmes tend to target individuals according to sexual orientation categories, understanding the potential associations between sexual orientation identity and HIV risk among MSMW is important for the planning of targeted HIV interventions.
This study examines sexual risk behaviour among MSMW recruited from two large urban cities in southern China: Chengdu and Guangzhou. These cities were selected due to their relevance to China’s growing HIV epidemic. Chengdu is located along the opium traffic route extending from Thailand and Burma through southwest China, a trade route which contributed to early HIV cases in Chinese injection drug user populations. Guangzhou is a large southeastern coastal city and a major site for global manufacturing and trade, which facilitates migration of populations from rural settings in China. Both cities have large MSM populations. The aims of this study are to examine (1) differences in socio-demographic characteristics and HIV prevalence between gay- and non-gay-identified MSMW; (2) differences in sexual behaviours with male and female partners between gay- and non-gay-identified MSMW; (3) correlates of unprotected vaginal sex and unprotected anal sex among MSMW.
Methods
Participants
From July 2010 to February 2011, 300 participants were recruited in Chengdu and Guangzhou, respectively (total sample = 600). Eligibility criteria were men who were 18 years or older, who had anal sex with another man in the past 12 months, and who had vaginal sex with a woman in the past 12 months or who were currently married to a woman. To facilitate our ability to reach the target populations, we collaborated with a non-governmental organization in each city (Chengdu Tongle Consulting Center and Guangzhou Xqsolutions/GZTZ.ORG) with a history of outreach to MSM and MSMW. Participants were recruited using snowballing methods. Initial participants were referred to the study by staff members at collaborating organizations. After completing the survey, participants were asked to refer other MSMW in their networks to the study. All referrals were screened for eligibility and invited to participate if eligible. Recruitment continued until 300 participants were enrolled at each city. The duration in Chengdu was from July 2010 to February 2011 and in Guangzhou was from July 2010 to January 2011.
Procedures
Surveys were conducted in private rooms at each of our collaborating organizations. A research assistant conducted informed consent procedures and then verbally administered the structured survey to participants. After completing the structured survey, participants received HIV testing and counseling, which involved two rapid tests to screen for HIV antibodies (RT-1, Shanghai Kehua Biotechnology Co., Ltd., Shanghai China; RT-2, Hangzhou ACON Biotechnology Cl., Ltd., Hangzhou China). If participants were previously diagnosed as HIV positive, they were not re-tested. Participants who were diagnosed as HIV positive were immediately referred to Centers for Disease Control and Prevention treatment and care services. Participants received 50 RMB for participation. Study procedures were approved by the Anhui Medical University institutional review board.
Measures
We assessed the following: social demographic characteristics (age, education, marital status, possession of a residence card, sexual orientation, etc.); sexual behaviour with male partners during the past six months (number of male partners, anal sex with boyfriend, anal sex with casual partner, anal sex with commercial male partner, frequency of condom use, condom use in the last three anal sex episodes, condom use in the last anal sex episode); sexual behaviour with female partners during the past 12 months (vaginal sex with wife, vaginal sex with girlfriend, vaginal sex with casual female partner, vaginal sex with commercial female partner, frequency of condom use, condom use in the last three vaginal sex episodes, condom use in the last vaginal sex episode). We used a six-month recall period for male partners, which is consistent with other studies with MSM and MSMW in China. We expanded the recall period for female partners to 12 months because prior studies indicated a low volume of heterosexual behaviours during the past six months.10,11
Statistical analysis
EpiData 3.0 (The EpiData Association, Odense, Denmark) software was used to input the original data, and SPSS 10.01 (Chicago, IL) was utilized for all analyses. In descriptive analyses, participants were categorized as gay-identified or non-gay-identified based on their response to an item on self-reported sexual orientation. Chi-square tests were conducted to examine the differences on socio-demographics, HIV status, and male and female sexual behaviours between gay-identified versus non-gay-identified MSMW. Logistic regression was utilized to identify independent covariates (especially sexual orientation) of unprotected anal and vaginal sex. The logistic regression were assessed by residual analysis (Hosmer and Lemeshow test) and the influence of possible conflicting observations was evaluated by a diagnostic test, with p < 0.05.
Results
Participant characteristics
Of 600 MSMW, 157 (26.2%) were HIV-positive; 41 (6.8%) were newly diagnosed, and 116 (19.3%) were previously diagnosed. Therefore, the prevalence of newly-diagnosed HIV infection in this sample was 8.5% (41/484).
Socio-demographic characteristics and HIV prevalence among gay- and non-gay-identified MSMW.
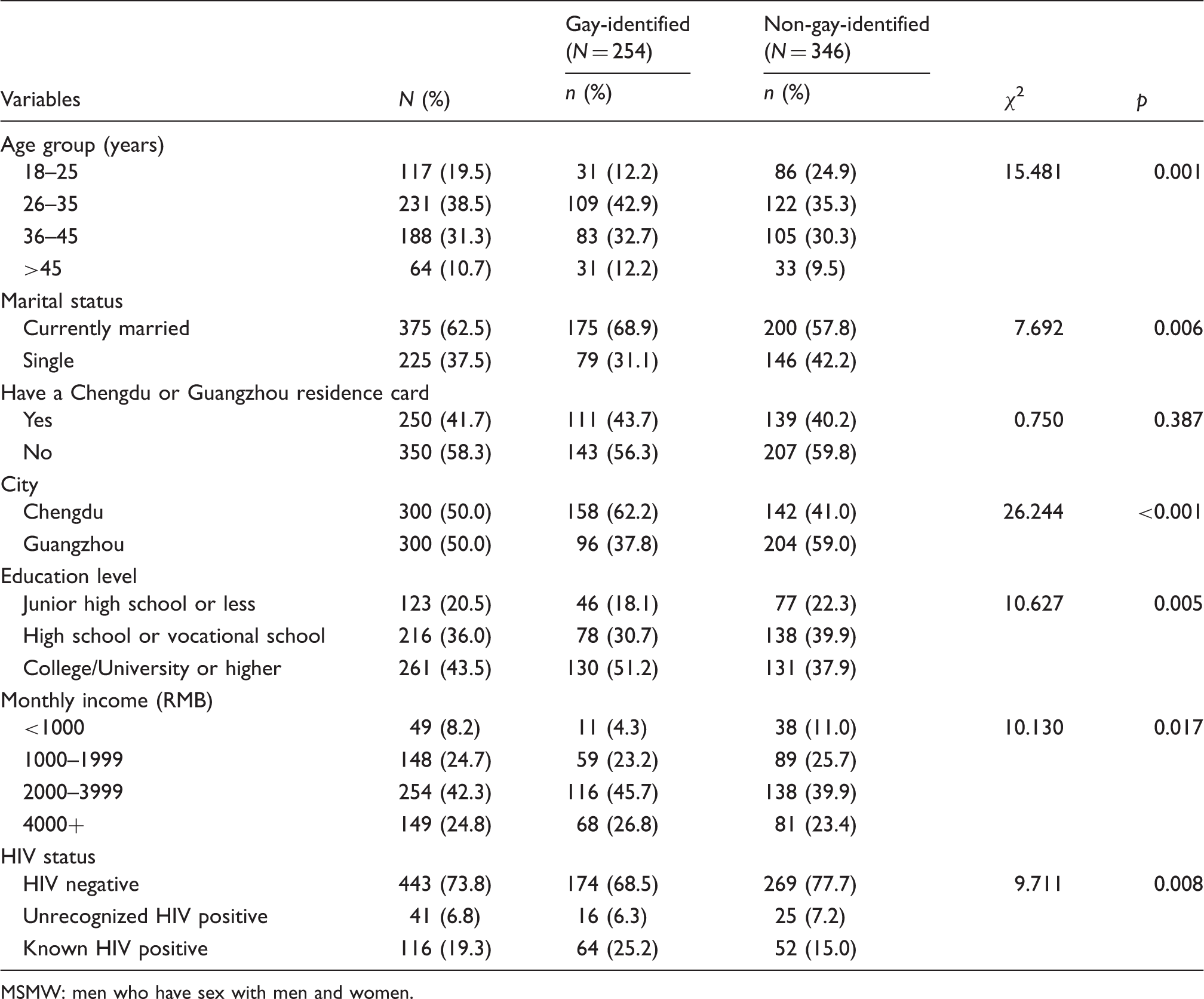
MSMW: men who have sex with men and women.
The mean age was 35.6 (SD = 9.2) among gay-identified MSMW and 33.4 (SD = 9.6) among non-gay-identified MSMW. Overall, 19.5% were aged 25 or below. Among non-gay-identified MSMW, the proportion of them aged 18–25 was 24.9%, which was significantly higher than 12.2% among gay-identified MSMW (χ2 = 15.481, p < 0.05). There were 68.9% gay-identified MSMW currently married, higher than 57.8% among non-gay-identified MSMW (χ2 = 7.692, p < 0.05). Men in two groups of MSMW did not differ significantly in their residency. In the sample as a whole, the majority (58.3%) did not have a residence card. More than half of gay-identified MSMW reported education level as college or higher. Moreover, the gay MSMW were slightly richer than non-gay MSMW (χ2 = 10.130, p < 0.05). Newly-diagnosed HIV infection among gay MSMW was 6.3% and 25.2% were already HIV-positive before our study, in contrast with 7.2% and 15.0% for non-gay MSMW, respectively (χ2 = 9.711, p < 0.05).
Sexual behaviours
Differences in sexual behaviours with men and women between gay-identified and non-gay-identified MSM.

MSMW: men who have sex with men and women.
Sexual behaviours with women for gay and non-gay MSMW are also shown in Table 2. The heterosexual behaviours for gay- and non-gay-identified MSMW were totally different. During the past 12 months, having a wife was common among MSMW, reported by 70.9% of gay-identified MSMW and 60.7% of non-gay-identified MSMW. In the past 12 months, the proportions of non-gay-identified MSMW who had girlfriends, causal female partners, or commercial female partners were 35.0%, 16.2%, and 5.8%, respectively, and were all higher than the 20.1%, 7.9%, and 2.8% reported by gay-identified MSMW. Almost all non-gay-identified MSMW (96.8%) reported having vaginal sex with women in the past 12 months; however, reported by only 71.3% of gay MSMW (χ2 = 79.485, p < 0.001). In the overall sample, the reporting of unprotected vaginal intercourse (UVI) was quite high (54.3%), which included MSMW who never or sometimes used condoms in the past 12 months. Furthermore, during the past 12 months among non-gay-identified MSMW 64.1% had UVI with female partners, which was higher than the 40.9% reported by gay-identified MSMW.
Risk factors for unprotected sexual behaviour
The prevalence and correlates of unprotected anal intercourse (UAI) with men during the past 6 months and unprotected vaginal intercourse during the past 12 months among 600 MSMW.

AOR: adjusted odds ratio; CI: confidence interval; UAI: unprotected anal intercourse; UVI: unprotected vaginal intercourse.
Model for UAI adjusted for age, marital status, city, residence card, education level, and monthly income.
The multivariate analysis of UVI in Table 3 showed that compared with gay-identified MSMW, non-gay-identified MSMW were more likely to engage in UVI during the past 12 months (AOR = 2.463, 95% CI = 1.780–3.407). Moreover, the risk factors for UVI included having multiple male partners (2–4, AOR = 1.293, 95% CI = 0.837–1.998; 5 or more, AOR = 2.148, 95% CI = 1.305–3.536), having multiple female partners (2–4, AOR = 1.202, 95% CI = 0.852–1.694; 5 or more, AOR = 2.044, 95% CI = 1.275–3.277) and during the past six months never or sometimes using condom for anal sex (never, AOR = 2.423, 95% CI = 1.299–4.522; sometimes, AOR = 3.329, 95% CI = 1.783–6.215). The normality of the residual values of this model was also checked with the Hosmer and Lemeshow test, which yielded a p value of 0.139, which indicated reasonable goodness of fit.
Discussion
This study demonstrated a high prevalence of HIV and unprotected sexual behaviours among MSMW and revealed substantial differences in demographic and sexual behaviours for gay-identified versus non-gay-identified MSMW. Overall, 26% of this MSMW sample was HIV positive and the prevalence of HIV was significantly higher among gay-identified (31.5%) than non-gay-identified MSMW (22.3%).
Nearly a quarter of non-gay-identified MSMW were aged under 25 years, indicating that many young men not identifying as gay engaged in homosexual and heterosexual behaviours at the same time. Moreover, high rates of unprotected vaginal (60.5%) and anal (23.3%) intercourse were detected. Therefore, future intervention strategies for Chinese MSMW should pay more attention to these young non-gay-identified MSMW. In this study, young non-gay-identified MSMW were more likely to engage in high risk behaviours and had less exposure to HIV interventions.
In the present study, we found that compared with gay-identified MSMW, non-gay-identified MSMW were highly heterosexually active, as evidenced by non-gay-identified MSMW being more likely to report sex with wives, girlfriends, casual and commercial female sexual partners during the past 12 months. However, it was striking that non-gay-identified MSMW were also highly homosexually active compared with gay-identified MSMW (32.4% non-gay-identified MSMW had five or more anal sex partners during the past six months compared with 22% gay-identified MSMW). We had anticipated that non-gay-identified MSM were less likely to report sex with men than gay-identified MSM, but these data indicate that this high rate of engagement in bisexual behaviours may put non-gay-identified MSMW at substantial risk of HIV infection. Furthermore, we found that having more than five male sex partners during the past six months increased the risk of UVI. This suggests that the sexual network of non-gay-identified MSMW is much broader and complex than that of gay-identified MSMW. The reason may be that non-gay-identified MSMW were better adapted to bisexual behaviours than gay-identified MSMW. This warrants increased attention on MSMW who do not identify them as gay as they may play a more important role in HIV spread.
The prevalence of UAI and UVI were high both among gay- and non-gay-identified MSMW. Gay-identified MSMW (52.4%) were more likely than non-gay identified MSMW (42.5%) to engage in unprotected anal sex with men during the past six months. However, non-gay-identified MSMW (64.1%) were more likely than gay-identified MSMW (40.9%) to report UVI during the past 12 months. The underlying reasons for these HIV risk behaviours remain unexplained. A large study among 2250 Chinese MSM reported that reasons for not using condoms included emotional and physical sensation with partner, sex with a regular partner, unavailability of condoms and lack of trust. 18 There are already many studies revealing the underlying psychological, cultural, social, economic, and structural factors related to these HIV risk behaviours.19–21 There are some common reasons that both gay MSMW and non-gay MSMW did not use condoms with men or women. There are also some specific reasons for subgroups of different orientations. Thus future Chinese studies should explore these common and specific factors for these two subgroups.
After controlling for the socio-demographic characteristics and HIV status we still found that gay-identified MSMW were more likely to engage in unprotected anal sex and less likely to engage in unprotected vaginal sex. In contrast, non-gay-identified MSMW were more likely to engage in unprotected vaginal sex and less likely to engage in unprotected anal sex.
Furthermore, an interesting finding in the correlates of unprotected sex is that MSMW who used condoms only sometimes or never for anal sex with men during the past six months were nearly two-fold and three-fold more likely to engage in unprotected vaginal sex during the past 12 months compared with MSMW who consistently used condoms for anal sex. At the same time, MSMW who sometimes or never used condoms for vaginal sex during past 12 months were nearly twice and four-fold more likely to engage in UAI during the past six months. Therefore, MSMW who had UAI with their male partners were much more likely to have UVI with their female partners and vice versa. This suggests that the habit of condom use or lack of use can be carried over from male to female partners and vice versa. This result was also found in a study among black MSMW in USA. 22 Consequently, targeted intervention is needed to change behaviours in order to not only increase condom use with male partners but also to increase condom use with female partners.
There are some limitations in this study. Firstly, we used convenience sampling to recruit participants which limits the generalizability of the findings. Secondly, the cross-sectional nature does not allow for the associations between related factors and unprotected behaviours. Thirdly, social desirability bias might have influenced responses to the questionnaire in this survey. Insufficient data were collected about other risk behaviours, social factors, and partnership characteristics. Further studies are needed to learn more about the general health and social risks of MSMW, and qualitative methodologies might be particularly useful to obtain in-depth narratives.
Conclusions
Our research findings show that the prevalence of both HIV and unprotected bisexual behaviours are high among MSMW of different orientations in two cities of China, as well as the significant differences in sexual behaviours between gay-identified and non-gay-identified MSMW. These differences should be taken into consideration to develop better targeted and comprehensive intervention strategies for controlling HIV spread between MSMW and from MSMW to the general population.
Footnotes
Acknowledgments
We would like to thank Delin Han from Center for Disease Control of Chengdu and Liping Dai from Center for Disease Control of Yuexiu district in Guangzhou for their aid in HIV testing, as well as MSM volunteers from Chengdu Tongle Consulting Center and Guangzhou Xiaoqi culture spread company for their aid in the data collection and HIV testing during our research.
Conflict of interest
The authors declare no conflict of interest.
Funding
This work was supported by Chinese Center for Disease Control and Prevention, AIDS Applied Research Project grant No. 2010146.