
Abstract
Preventing HIV infection is a priority for militaries. HIV prevention research is needed to monitor existing programme, identify areas for modification, and develop new interventions. Correct and consistent condom use is highly effective against HIV. However, use among soldiers is lower than ideal. This study describes condom use behaviours and examines correlates of use in the Botswana Defence Force (BDF). Analyses were based on 211 male BDF personnel, aged 18–30, who completed a cross-sectional survey that collected baseline data for an intervention study. Results showed that 51% of participants reported always using condoms, 35% used condoms most times, and 14% used condoms occasionally/never. Condom use varied by partner type and was typically higher with casual partners in comparison to regular partners. After adjustment for age and marital status, factors associated with lower condom use included excessive alcohol use, perception that using condoms reduce sexual pleasure, and having a trusted partner. However, higher levels of HIV knowledge and reports of being circumcised were protective against lower condom use. HIV interventions aimed at increasing condom use in the BDF should address condom perceptions, alcohol abuse, and issues of trust. Innovative ways to increase condom use in this population should also be explored.
Introduction
Botswana has one of the highest HIV prevalence rates in the world, estimated at 25% among adults aged 15–49. 1 While the HIV epidemic in Botswana is generalized, there is concern that military personnel may be particularly vulnerable due to unique circumstances that surround military service. They are predominately young, susceptible to peer pressure,2,3 and highly mobile. To relieve stress and loneliness during deployments, soldiers may engage in risky sexual behaviours, such as having unprotected sex with sex workers. 4 Furthermore, studies have found high HIV risk-taking behaviours in this population, including having multiple sexual partners and abusing alcohol.5–7
There is overwhelming evidence that condoms are highly effective in preventing sexual transmission of HIV if used correctly and consistently.8–10 However, consistent condom use among sexually active military personnel has generally been reported to be very low. For example, studies in the Nigerian military showed that consistent condom use was only found in 16–20% of participants, 7 and 41% did not use a condom the last time they had sex with a sex worker. 4 In the Rwanda Defence Forces, 24% did not use a condom the last time they had sex with a sex worker. 11 And in the Angolan military, only 54% of participants reported using a condom during their last sexual encounter with a sex worker. 6
While several studies have examined correlates and predictors of condom use among military personnel,6,12,13 additional research in other militaries is needed to better characterize these predictors, evaluate the effectiveness of existing military HIV prevention programmes, and identify key programme areas that need targeting or modification. This study describes current condom use behaviours and examines correlates of use in the Botswana Defence Force (BDF), which to our knowledge has never been previously investigated.
Materials and methods
Study design and participants
Data used for this analysis were based on a cross-sectional survey conducted among the BDF which formed the baseline data for a non-randomized intervention study of the effect of condom wrapper graphics and scent on condom use in the BDF. Participants were male BDF personnel who ever had sex, aged 18–30 years, and stationed at one of four selected military sites. Participants were recruited through flyers, command newsletters, and standard military communication channels. Interested personnel attended an informational briefing where the study purpose and procedures were explained. A total of 211 (81.2%) men, of a target sample size of 260, provided written informed consent. This study was approved by institutional review boards in the United States (Naval Health Research Center and San Diego State University, San Diego, California) and Botswana (Ministry of Health, Gaborone, Botswana).
Study procedures
Study personnel briefed interested individuals on the procedures and conducted the written informed consent process. Consented participants self-completed a paper-based survey that was administered in a group setting. Questions were read out loud by a trained survey administrator while participants followed along and marked responses on their surveys. The baseline survey collected demographics, sexual behaviour history, condom use frequency, attitudes and behaviours, HIV risk perception, HIV knowledge, alcohol use, and circumcision status.
Correlates of interest
Sexual history correlates included age at sexual debut, number of lifetime partners, number of regular and casual partners in the past 12 months, and having more than one sexual partner in the past 3 months. HIV risk perception correlates included knowledge of one’s HIV status, knowledge of others in the unit known to have HIV, and ever cared for or lived with someone with HIV/AIDS. Participants were tested on HIV prevention, transmission, and general knowledge with eight questions: five were based on the United Nations General Assembly Special Session (UNGASS) on HIV/AIDS core indicators 14 and three were locally adapted. The HIV knowledge score was calculated as a percent of the 8 HIV knowledge questions correctly answered. Participants with missing values for HIV knowledge questions were excluded from this calculation.
Circumcision status was self-reported. Alcohol use was measured using the Alcohol Use Disorders Identification Test (AUDIT), which has been validated in several countries world-wide (including those in Africa) 15 and previously used in African military personnel.6,11 The AUDIT consists of 10 questions that measure alcohol use, harmful and hazardous drinking, and alcohol dependence. Responses to each question were scored on a range of 0–4 and were summed for a composite score ranging from 0 to 40. Non-drinkers were defined as those having an AUDIT score of 0, mild drinkers had a score of less than 8, and problem drinkers had a score of 8 or higher. Participants who were missing all AUDIT questions (n = 1) and those missing several questions from the AUDIT but had a computed score bordering on problem drinking were excluded from analyses (n = 3).
Participants were asked to provide their opinions (agree, disagree, or don’t know) about condom use on 10 statements. Denominators for each statement varied and only included those who agreed or disagreed; those responding “don’t know” were excluded. Participants were also asked to provide reasons for not using condoms and indicate how often they carried condoms with them, such as in their uniform or wallet.
Outcome measures
The outcome was condom use frequency in the past 3 months defined as always, most times, occasionally, or never using condoms. The categories occasionally and never were collapsed into one group due to few responses in each.
Statistical analysis
Descriptive statistics were computed, including frequencies and percentages for categorical variables and means and standard deviations or medians and ranges for continuous variables. Bivariate ordinal regression analyses were used to examine the relation of each correlate of interest with the outcome of condom use frequency, defined as the odds of decreasing condom use. Variables significant at p ≤ 0.15 were examined further in individual ordinal models adjusting for continuous age and marital status, since these covariates have been found to be significantly associated with condom use.16,17 All variables significant at p ≤ 0.15 were entered into a backwards selection regression model, which also adjusted for age and marital status. The Likelihood Ratio test was used to determine whether a variable was kept in the model at each step of the elimination process. A two-tailed p < 0.05 was used to determine statistical significance in the Likelihood Ratio test and the final backwards selection regression model. The proportional odds assumption was satisfied for all models. Multicollinearity was assessed by examining the variance inflation factor (VIF) and tolerance values; no variables in the model were determined to be collinear. Logistic regression analyses were also performed treating condom use frequency as a binary outcome in two separate models: (1) occasional/never vs. most times/always and (2) occasional/never/most times vs. always. All statistical analyses were performed using SAS statistical software version 9.3 (SAS Institute, Cary, NC).
Results
Demographic characteristics of study participants (N = 211).

NCO: non-commissioned officer; SD: standard deviation.
Excludes one participant with a missing response.
Approximately 69% of participants who were single and 72% of those who were cohabitating reported having more than one sexual partner in the past 3 months. One of two married participants (50.0%) reported having more than one sexual partner. Participants were asked a series of questions about sexual behaviours with their two most recent partners during the past 3 months. Of the 168 single participants who provided responses to these questions, 25.6% reported having one regular partner only, 20.8% reported two regular partners, 5.4% one casual partner only, 13.1% two casual partners, and 35.1% reported having both one casual and one regular partner. Of 36 cohabitating (non-married) participants who provided responses, 27.8% reported having one regular partner only, 16.7% two regular partners, and the remainder (55.5%) reported having both one casual and one regular partner. Of the two married participants, one reported having one regular partner only and the other reported having 2 regular partners (data not shown).
Characteristics of condom use correlates of study participants (N = 211).

AUDIT: Alcohol Use Disorders Identification Test; SD: standard deviation.
Excludes participants with missing responses.
Percentage of correct responses to eight HIV knowledge questions: HIV can be prevented by having sex with one faithful uninfected partner (94.8%), by using condoms (99.5%), and remaining abstinent (91.0%). A healthy looking person can have HIV (98.1%). HIV cannot be transmitted through mosquito bites (86.3%), witchcraft/supernatural means (76.8%), or by sharing a meal with an infected person (96.2%). HIV can be transmitted through traditional practices (60.2%).
Agreement with each statement.
Condom use frequency in the past 3 months is presented in Figure 1. Approximately 51.2% of participants reported always using condoms, 35.1% reported using condoms most times, and 13.7% reported using condoms occasionally/never. Among 54 participants with one regular partner in the past 3 months, 51.9% reported always using condoms with this partner. Of 9 participants with one casual partner, 77.8% reported always using condoms with that partner. Of 79 participants with one casual and one regular partner, 84.8% reported always using condoms with their casual partner, while 40.5% reported always using condoms with their regular partner (data not shown).
Study participants’ reported condom use frequency in the past 3 months (N = 205).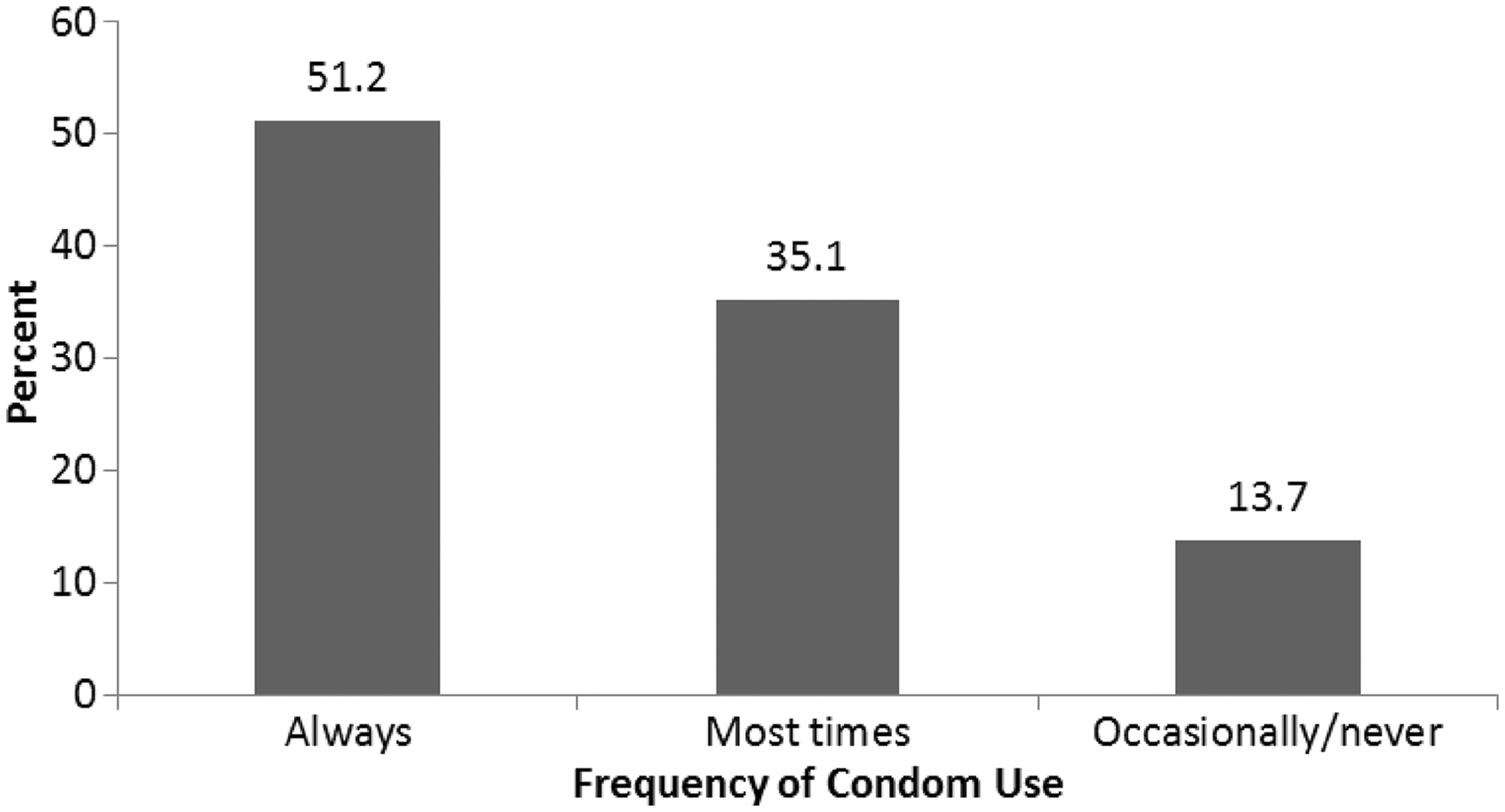
Unadjusted and adjusted associations of each condom use correlate with decreasing condom use frequency.

AUDIT: Alcohol Use Disorders Identification Test; CI: confidence interval; OR: odds ratio.
Adjusted for age and marital status.
Estimates may be wide due to small samples.
Multivariate ordinal regression model examining the association between correlates of condom use and decreasing condom use frequency (N = 192).

AUDIT: Alcohol Use Disorders Identification Test; CI: confidence interval; OR: odds ratio.
Adjusted for age, marital status, and other variables in the model.
Estimates may be wide due to small samples.
Discussion
Increasing condom use is critical to reducing HIV infection. It is one of the least expensive and most accessible methods for HIV prevention. However, its use continues to be disappointingly low among military personnel due to many factors, including the belief that condoms are ineffective 18 or unreliable, 19 conflict with religious beliefs, 18 trust issues that are raised with its use, 20 and a desire to become pregnant. Results show that consistent condom use was relatively low in the BDF, with only 51% of participants reporting always using condoms. Similar to other studies, condom use was also generally higher with casual partners than with regular partners.6,21,22 However, while we may be encouraged by the high percentage of participants reporting condom use with their casual partners, this percentage is still not 100%. Military personnel in multiple sexual partnerships who are not consistently using condoms place themselves and their partners at higher risk for HIV infection.
The correlate most strongly associated with lower condom use was the belief that condoms make sex less enjoyable. As reported in other studies, putting on a condom dampens sexual mood, 18 using condoms causes discomfort, 19 or skin-to-skin sexual contact is preferred. 18 Furthermore, there could be physical attributes of the condom that discourages use. As observed in this study, lower condom use was bivariately associated with the belief that condoms smell bad. These findings have important implications regarding condom use in general and specifically the use of government-issued condoms (i.e. condoms provided free of charge by the BDF to their members). Anecdotal reports suggest that government-issued condoms are often not used due to an unpleasant scent (personal communication with BDF, September 2009). Therefore, while most (82%) agreed they would use condoms more often if they were available for free, the authors speculate they may not be using government-issued condoms because of the unpleasant odor. The BDF should consider providing condoms that are appealing to their members, which may help increase usage. Further qualitative research examining why condoms reduce sexual pleasure among this population is also needed.
The high percentage (59%) of problem alcohol use in the BDF and its association with lower levels of condom use and hindrance of condom use raises concern. The percentage of BDF personnel categorized as problem alcohol users in the AUDIT (59%) are much higher than those reported in the general male Botswanan population of comparable mean age (39%). 23 Alcohol abuse, risky behaviours, and HIV risk should be addressed in BDF prevention programmes. Other potential preventive measures include supporting the Botswana government initiatives of increasing tax on alcohol purchases, limiting alcohol availability on the military bases, and providing free condoms where alcohol is sold. The BDF should also bolster and increase their alcohol abuse prevention, treatment, and rehabilitation programmes.
This study found a significant association between reported trust for a sexual partner and lower condom use, as shown in other quantitative24,25 and qualitative studies. 26 While lower condom use among those in a monogamous relationship is expected, lower and inconsistent condom use among those involved in multiple sexual partnerships or HIV-discordant relationships may be extremely risky. As observed in this study, nearly 70% of participants reported having more than one sexual partner in the past 3 months, suggesting that multiple partnerships are quite common; therefore, the practice of consistent condom is highly important. The BDF should encourage couples’ HIV testing and counseling and support the disclosure of HIV status to all sexual partners, which will assist in making informed decisions regarding sexual practices and condom use.
Although not statistically significant, due to a low number of affirmative responses, highly elevated odds of lower condom use were observed among those who agreed with the statement that a woman would lose respect if she asked a man to use a condom. These findings suggest some BDF personnel may have a negative attitude towards condoms or they may be influenced by norms that affect usage, as shown in other studies.27,28 This area of research should be further explored among military personnel as it touches on important factors that may affect condom use.
Consistent with other studies,29,30 higher levels of HIV knowledge were found to be associated with more frequent condom use. Elevated levels of HIV knowledge may be an indication that the BDF HIV educational programmes have been effective and are reaching the younger populations. The BDF should continue to educate their members on HIV prevention and transmission, coupled with messages of correct and consistent condom use.
Lastly, the finding of increased condom use among men who reported being circumcised is promising, since there is concern that circumcised men may practice more risky sexual behaviours following male circumcision (MC) because their perception of HIV risk may be falsely reduced. These results support findings from other studies that show circumcised men do not engage in more risky sexual behaviours than uncircumcised men31–33 and suggest that BDF prevention messages regarding correct and consistent condom use after MC may be highly effective. The BDF should continue to promote consistent condom use after MC.
There were a few limitations to this study including the cross-sectional study design and the fact that the target sample size was not reached, possibly affecting the study power. Due to strict participant eligibility criteria, results may only be generalizable to BDF members of comparable age. Although not all BDF sites were included in the study, the four that were selected contained the largest number of personnel with diverse backgrounds. Respondent bias may also have been an issue, with participants providing socially desirable responses. However, confidentiality measures were in place to ensure privacy during survey administration and participants were informed they could skip any questions they did not feel comfortable answering. Despite these limitations, the study also has several strengths. For instance, the survey was self-completed, which may have encouraged participants to provide reliable responses. In addition, numerous correlates of condom use were examined and the participation rates were considered high, with very few missing data in the baseline survey. These allowed for more complete statistical analyses of factors associated with condom use among military personnel in Botswana.
In summary, this study described condom use behaviours in the BDF, highlighted factors associated with lower condom use, and discussed approaches to increase condom use among military personnel, a population at increased risk for HIV. Because condoms are the most effective way to prevent sexual transmission of HIV, understanding why condoms are not used and developing methods to increase use in this population should be a high priority for militaries.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, the Department of Defense, or the US Government. Approved for public release, distribution is unlimited. Human subjects participated in this study after giving their free and informed consent. This research has been conducted in compliance with all applicable federal regulations governing the protection of human subjects in research (Protocol NHRC.2010.0025).
Footnotes
Acknowledgments
We wish to thank members of the BDF who participated in this study and all BDF study personnel who helped facilitate data collection. We also thank the staff at Population Services International and the Department of Defense HIV/AIDS Prevention Program epidemiology team for their logistical support throughout the study.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research is supported by the Department of Defense HIV/AIDS Prevention Program, under work unit 60546. Funding for this study was provided by the President’s Emergency Plan for AIDS Relief.