
Abstract
The varieties of luetic clinical variants are countless in nature. In this regard, an autopsy case of a 72-year-old homeless man who accidentally succumbed to carbon-monoxide poisoning is here presented and reviewed. The autopsy revealed the highly unusual finding of asymptomatic syphilitic necrosis of spleen followed by luetic mesaortitis, a solitary skin gumma, and syphilitic arthritis. The spleen was 8 × 4 × 3 cm in size; the capsule was completely calcified and firm, 3 to 5 mm thick. Only in the region of the hilus was a small part of preserved tissue found. After puncturing the capsule, a brown-yellowish pus-like mass was found which filled the entire space inside. When reviewing the relevant literature, this case and its finding of pan splenic necrosis accompanied by a calcified capsule seem to be unique in nature. In terms of the final diagnosis, a Treponema pallidum haemagglutination assay confirmed it to be syphilis. Since it was a late stage of the disease, it is estimated that it may have been present for more than 20 or 30 years in the deceased.
Introduction
Syphilis is a systemic infectious disease distributed world-wide. In the post-Second World War period, its incidence was in decline,1,2 to the extent that syphilis has become a rare disease in the developed world. Nevertheless, in recent years, its frequency has been found to be slowly on the rise.3,4 Changes in sexual behaviour have facilitated the spread of syphilis, especially among men who have sex with men. Therein, less restrictive immigration, as well as HIV infection, have been implicated as being two major factors contributing to the resurgence of the disease.
Most commonly, the appearance of single or multiple sores are signs of the first (primary) stage of syphilis. The sores are painless, lasting 3 to 6 weeks and heal regardless of whether treatment is undertaken. If left untreated, the infection progresses to a second stage often manifesting with skin rashes, sores in the mouth and on the external genitalia. Itching is not usually present at this stage. The rash itself may appear in a range of variations in texture, colour and areas of the body. In addition to these symptoms, secondary syphilis may be followed by fever, swollen lymph nodes, sore throat, patchy hair loss, headaches, weight loss, muscle aches and/or fatigue. Without appropriate treatment, the infection can progress to a possibly latent and late stage of the disease, and the infection can continue to be harboured in the body, while bearing no signs or symptoms of the disease itself. This latent stage can continue for years. In the late stages of syphilis, the disease can damage the brain, nerves, eyes, heart, blood vessels, liver, bones and joints, which can result in death.5–7
Due to the wide range of symptoms, it would seem that the varieties of clinical presentations of syphilis are endless in their nature.8–10 In the present paper, a very unusual case of asymptomatic syphilitic pan-splenic necrosis in addition to several other syphilitic manifestations is presented.
Case presentation
A 72-year-old homeless man succumbed to the carbon-monoxide poisoning in his improvised shelter due to inadequate ventilation of the firebox. His friends, who had known him for the last 25 to 30 years of his life since he had moved to the area, described him as a healthy man in comparison to them. In the language of the homeless, “healthy” should be considered to mean that he did not cough as frequently, did not abuse alcohol, had no visible skin disease, furuncles, pediculosis, scabies or other such symptoms commonly suffered by this population.
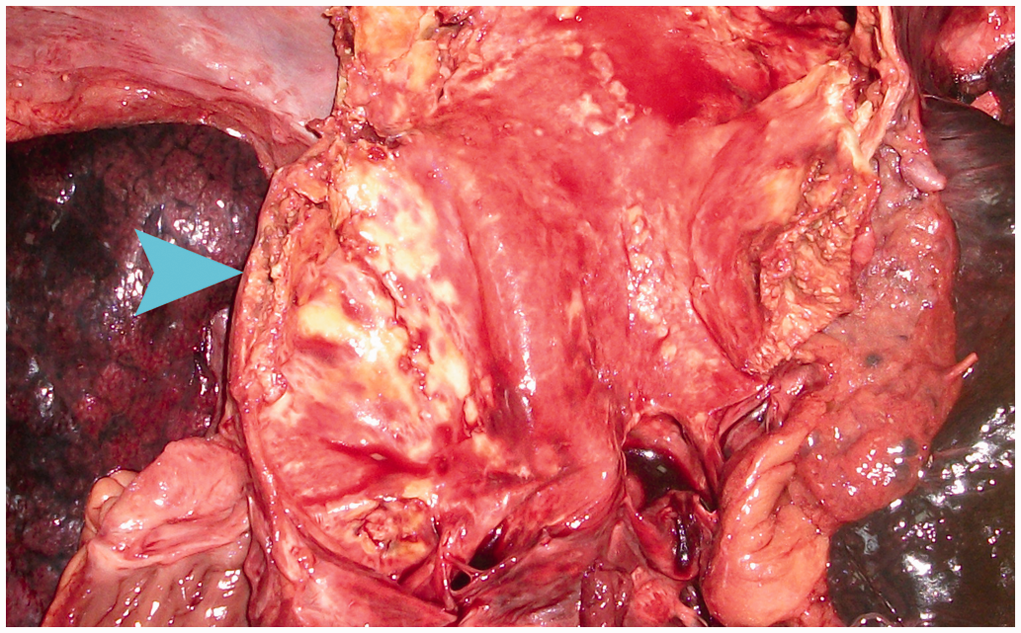
The autopsy’s external examination noted the deceased’s unkempt physical appearance. A dense bean-sized dark-purple rash covered his chest region. In the interscapular region, there was a soft, purple-reddish ulcerated lesion, 4 × 3 × 0.5 cm in size, which resembled a basal cell carcinoma. The finger and toe joints were tortuously deformed and callous. An unusual finding was noted in the section of the spleen (Figure 1), which was 8 × 4 × 3 cm in size. The capsule was completely calcified and firm, 3- to 5-mm thick; only in the region of the hilus was a small part of preserved tissue to be found. After puncturing the capsule, a brown-yellowish pus-like mass was found to fill the entire area inside. The total weight of the spleen was 220 g, but when the pus-like mass was emptied, the weight of capsule was approximately 140 g. Moreover, an aneurysm of the ascending aorta was present of nearly 6 cm in diameter, whose endothelium was thick, rugged and husky, similar to the bark of a tree, since the central part of the aortic wall was necrotic, brown-yellowish, pus-like (Figure 2). Despite this unusual finding, all other organs were macroscopically normal in their appearance.
Pansplenitic necrosis – capsule. Luetic mesaortitis.
Apart from the fatally elevated carboxyhaemoglobin (53%), the toxicological examination was completely negative regarding the presence of any narcotics, drugs, poisons or heavy metals.
Since the presented autopsy findings suggested the presence of syphilis, a qualitative VDRL test was performed, and it was negative (Biotec VDRL Carbon Antigen, BIOTEC Laboratories Ltd Kentford, Suffolk, UK), whilst a Treponema pallidum haemagglutination assay gave a positive result (IMMUNOTREP-TPHA, Immunotrep, Omega Diagnostics, Alloa, Scotland, UK).
A detailed microscopic examination, which was performed using haematoxylin-eosin (HE) staining, revealed a mild pulmonary oedema; the endothelium of the aorta was covered by merged plaques, mostly calcified and somewhere ulcerated, since the muscle layer was almost entirely necrotic. HE stains of the small preserved area of splenic tissue and cuts of tumorous skin lesion revealed a granulomatous inflammation, with lymphocytic infiltrate, zones of epithelioid cells, multinuclear giant cells and initial fibrous degeneration accompanied by large, mostly central, areas of necrotic tissue. Utilizing Gomori's silver staining cuts of the aortic wall, rare spirochetes were seen (Figure 3); however, no spirochetes were found in the cut sections of the preserved splenic tissue, nor in the skin lesion.
Spirochetes seen with the use of Gomori silver stains, ×100.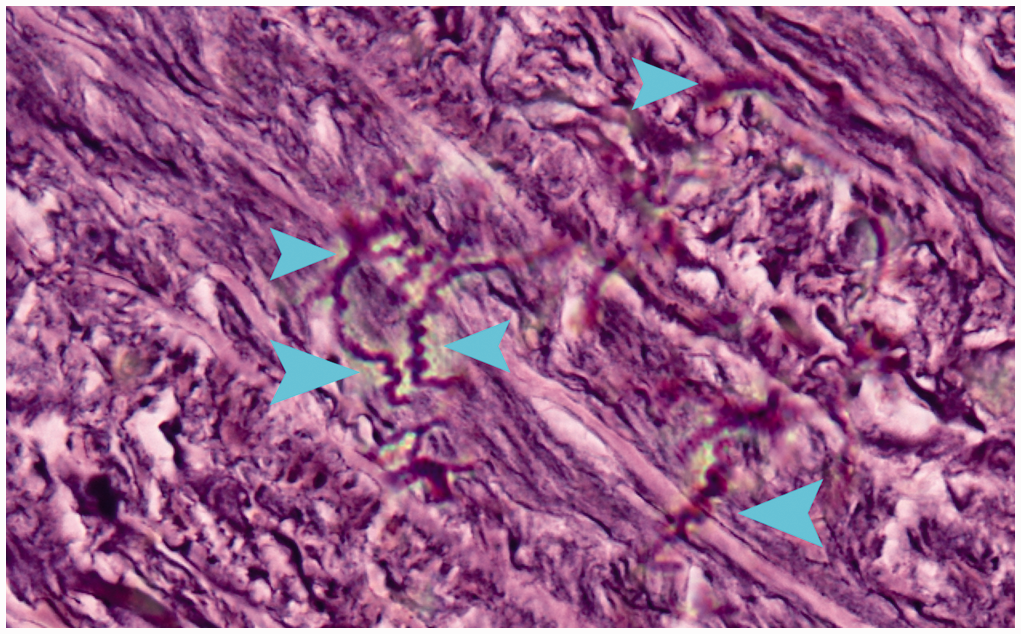
Discussion
Andrade et al. 11 have reported on a case of a young immunocompetent woman suffering from a solitary cutaneous ulcer, which was the first and singular manifestation of a previously unknown and undiagnosed case of late syphilis. This would seem to be the first published case of asymptomatic late syphilis that also had a solitary gumma.
In the case under review here, the various clinical manifestations, which can be seen in different stages of the disease created confusion related to the duration of the disease. The latent (hidden) stage or late stage of syphilis begins when the disease’s primary and secondary symptoms disappear.5,7 Considering a skin rash to be a proper sign of the secondary stage, all other manifestations are related to the late stage itself. Therein, in the case of the deceased here, a tumour-like ulcerated lesion was found, likely representing a solitary skin gumma, while the appearance of the fingers and toes was in accordance with syphilitic arthritis. The luetic mesaortitis hence completes the picture of late syphilis. Reviewing the literature, the pan-splenic necrosis with completely calcified capsule found in this case would seem to be a unique finding. Such inflammation that leads to complete splenic necrosis might be expected to cause symptoms that warrant medical attention, otherwise succumbing to an early death as a result. It is very difficult to understand why the deceased had not done so or had not needed to. It is notable that the brain and liver were intact in the presence of so many other manifestations of late syphilis.
In the differential diagnosis of complete splenic necrosis, the Kinyoun modification of the Ziehl–Neilsen technique for detecting tuberculosis was performed in the present case, and was negative (Koch's bacilli were not seen). In addition, the man was not cachectic, which is supported by obtained information that he had been “healthy” and “did not cough.” The lungs were macroscopically and microscopically normal in their appearance, and the hilar lymph nodes were not enlarged. All of these signs suggest active tuberculosis was unlikely. Apart from tuberculosis, splenic abscess/necrosis can be seen as a complication of endocarditis, in AIDS, typhoid fever, cat scratch disease, trauma of the spleen or induced by chemotherapy.12–14 Due to the fact that the granulomatous massive necrosis of the spleen was investigated histopathologically, as well as that the heart valves were macroscopically normal in their appearance, no internal or external signs of trauma of the splenic region were found, and no medical data or autopsy findings of neoplasm were present, we conclude that syphilis was the causative agent of the necrosis of spleen.
In his paper published in 1921, Wile 15 wrote that syphilis of the spleen is an exceedingly common finding in congenital syphilis in newborns, and a not infrequent pathologic finding in recent syphilis, but is relatively rare in acquired syphilis. Clinical syphilis of the spleen occurs early, in the form of an acute splenic tumour, with or without pain. In late syphilis, it occurs as interstitial splenitis, as solitary or miliary gummas of the spleen. 15 When conducting a study involving 2056 patients suffering from splenomegaly, O’Reilly 16 found that five of them had luetic hepatitis and one had gummas of the spleen. The entire spleen in the case presented here resembles a large gumma.
The homeless usually die at much younger ages, mostly as a consequence of tuberculosis, pneumonia, liver insufficiency or alcohol intoxication. The age of the deceased in the present case suggests he was seemingly healthy. Approximately 15% of individuals who have not been treated for syphilis do develop late-stage syphilis, which can appear decades after the initial infection.5,7 Since the late stage of the disease was diagnosed in this particular individual, the estimated duration of the syphilitic infection might have been more than 10 or even as much as 30 years.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.