
Abstract
In 2015, the Centers for Disease Control and Prevention (CDC) and the American Academy of Ophthalmology (AAO) released clinical advisories on rising cases of ocular syphilis. We examined the association between eye disease and syphilis infection among primary care and sexually transmitted infection (STI) clinic patients attending an urban lesbian, gay, bisexual, transgender (LGBT) health center. We conducted a retrospective medical record review of all patients who underwent syphilis testing at Howard Brown Health between 1 January 2010 and 31 December 2015. Confirmed eye diagnosis was based on International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes for conjunctivitis, uveitis, keratitis, retinitis, and red eye. Demographic information, syphilis treatment, HIV status, and high-risk behaviors were abstracted. Syphilis diagnosis was defined by available laboratory data (enzyme immunoassay [EIA], rapid plasma reagin [RPR] titer, fluorescent treponemal antibody absorption [FTA-Abs], Treponema pallidum Ab). Multivariable logistic regression with robust variance was used to identify independent associations. During the study period, 71,299 syphilis tests were performed on 30,422 patients. There were 2288 (3.2%) positive syphilis tests. Seventy-seven patients had a confirmed eye diagnosis (0.25%). Patients with eye disease had higher probability of at least one positive syphilis test (33%) compared to those without eye disease (8%) (p < 0.01). Of patients with eye disease, 77% were men who had sex with men (MSM) and 65% were HIV-positive. Patients with eye disease had 5.97 (95% CI: 3.70, 9.63) higher odds of having syphilis compared to patients without eye disease. When adjusted for age, race, gender/sexual orientation, insurance status, and HIV status, this association between positive syphilis test and eye disease decreased but was still significant (OR 2.00, 95% CI 1.17, 3.41). Patients who present with an eye diagnosis to STI/primary care clinic have a higher probability of positive syphilis tests even after adjusting for other risk factors for syphilis. High-risk patients with eye symptoms should have routine STI testing and in keeping with CDC and AAO recommendations, full ophthalmologic examination.
Key messages
Patients with eye diagnoses at a large, urban STI/primary care clinic had a
significantly higher odds of positive syphilis testing than those without eye
disease. The overall prevalence of eye disease in this population was low at 0.25%. In multivariable analyses, eye diagnosis, MSM, and HIV status were significantly
associated with positive syphilis tests; however, MSM and HIV were stronger risk
factors for positive syphilis tests than eye diagnosis.
Introduction
The incidence of syphilis, including ocular syphilis, has been increasing steadily over the past 15 years, particularly in men who have sex with men (MSM) and HIV-positive patients. 1 Ocular syphilis often presents with symptoms of blurred vision and clinical signs of uveitis during the secondary or tertiary stage of disease. Minor ocular complaints such as red eye or conjunctivitis may be associated with earlier stages of disease. 2
The purpose of this study was to determine the prevalence of eye disease in patients who presented to a large urban sexually transmitted infection (STI)/primary care clinic and to analyze whether patients with eye diagnoses had a higher likelihood of having positive syphilis test results. We examined risk factors that were associated with co-occurrence of eye diagnoses and positive syphilis test results.
Methods
Subjects and data collection
We conducted a retrospective medical record extraction of all patients who had syphilis testing performed at Howard Brown Health between 1 January 2010 and 31 December 2015. Howard Brown Health is the largest lesbian, gay, bisexual, transgender (LGBT) clinic providing primary care and STI testing in the Midwest of the United States. Patients who had eye diagnoses based on specific International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes for conjunctivitis, uveitis, keratitis, retinitis, and red eye were identified and medical chart review was performed. Institutional review board approval was obtained by the participating institutions (UIC 2016-0279, Howard Brown E-054) for medical chart review. Informed consent was waived due to the retrospective nature of the medical record review.
Variable classification
The exposure or independent variable of interest was defined as presence or absence of eye disease. The outcome or dependent variable was a positive or negative syphilis test result. Patients with at least one positive test during the study period were categorized as positive. Positive syphilis test results were defined by an algorithm using available laboratory test results including: enzyme immunoassay (EIA), rapid plasma reagin (RPR) titer, and fluorescent treponemal antibody absorption (FTA-Abs) or Treponema pallidum Ab. Sensitivity analysis for a positive syphilis test result was performed by using the medication order for bicillin associated with a positive syphilis test result to confirm a true case of syphilis. The proportion of bicillin orders in the negative test group was also calculated.
Covariates included HIV status, a gender/sexual orientation composite variable (Male-MSM, Male non-MSM, Transgender, and Female), race/ethnicity (white, black, Hispanic, Asian/unknown), insurance status (public, private or none), and age group in years (18–29, 30–39, ≥40).
Analysis
The closest observation in time to eye disease for each subject was selected to represent demographic information for covariates. Categorical data were analyzed using Chi square tests. Multivariable logistic regression with robust variance was used to model the odds of at least one positive syphilis test comparing the group with eye disease to the group without eye disease with exposure and covariate variables as fixed effects. Subgroup analysis was conducted by restricting the analysis to specific subpopulations, including MSM male, not MSM, and HIV-positive men. All analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC) with a significance level α = 0.05.
Results
Frequencies and percentages by eye diagnosis results are shown in Table 1. During the study period, 71,299 syphilis tests were performed on 30,422 patients. The prevalence of eye disease among all patients was 0.25% (77 patients). Of the 77 patients with eye diagnoses, 50 (65%) had conjunctivitis, 14 (18%) redness, five (6.5%) iridocyclitis, five (6.5%) chorioretinitis, and three (4%) keratitis. There were 2288 positive syphilis tests (3.2%) among 1789 unique patients. Patients with eye disease were more likely to have positive syphilis tests (32.5%) compared to those without eye disease (7.5%) (p < 0.01). Patients with eye disease were more likely to be HIV-positive (64.9%), MSM (76.6%), 40 years or older (42.9%), and have private insurance (51.9%) compared to patients without eye disease (p < 0.01).
Demographics by eye diagnosis.

Patients with positive syphilis tests were more likely to have bicillin orders within 30 days of testing than those with negative tests (78.1% vs. 6.1%, p < 0.01). In the eye disease group, 76% of patients with positive syphilis tests had a bicillin order while 17.3% of negative tests also had a bicillin order (p < 0.01).
Based on chart review, 19 of 77 patients with eye diagnoses were referred for further ophthalmologic evaluation and only six of these patients had confirmation of ophthalmic diagnosis and follow up. Eight of 19 (42%) patients had positive syphilis tests. There was a median of 163.5 days between eye diagnosis and syphilis testing in all 25 patients with eye diagnosis and positive syphilis tests; these diagnoses included 12 conjunctivitis, seven redness, three iridocyclitis, two chorioretinitis, and one keratitis. Of the 58 patients who had eye disease and did not follow up with ophthalmology, 45 patients had STI testing a median of 113 days later with no report of eye disease mentioned at this follow-up appointment.
Multivariable logistic regression results of the likelihood of positive syphilis test results are shown in Table 2. There was 5.97 higher odds of a positive syphilis test result in the eye disease group compared to the no eye disease group (p < 0.01). When adjusted for other risk factors such as HIV, age, race, gender, and insurance, this association was slightly attenuated but still significant (OR 2.00, p = 0.01). When analysis was restricted to the MSM subgroup only, the odds of a positive syphilis test result in the eye disease group compared to no eye disease was 4.61 (p < 0.01) in the unadjusted model and 1.97 (p = 0.02) in the adjusted model.
Crude and adjusted logistic regression for likelihood of a positive syphilis test.
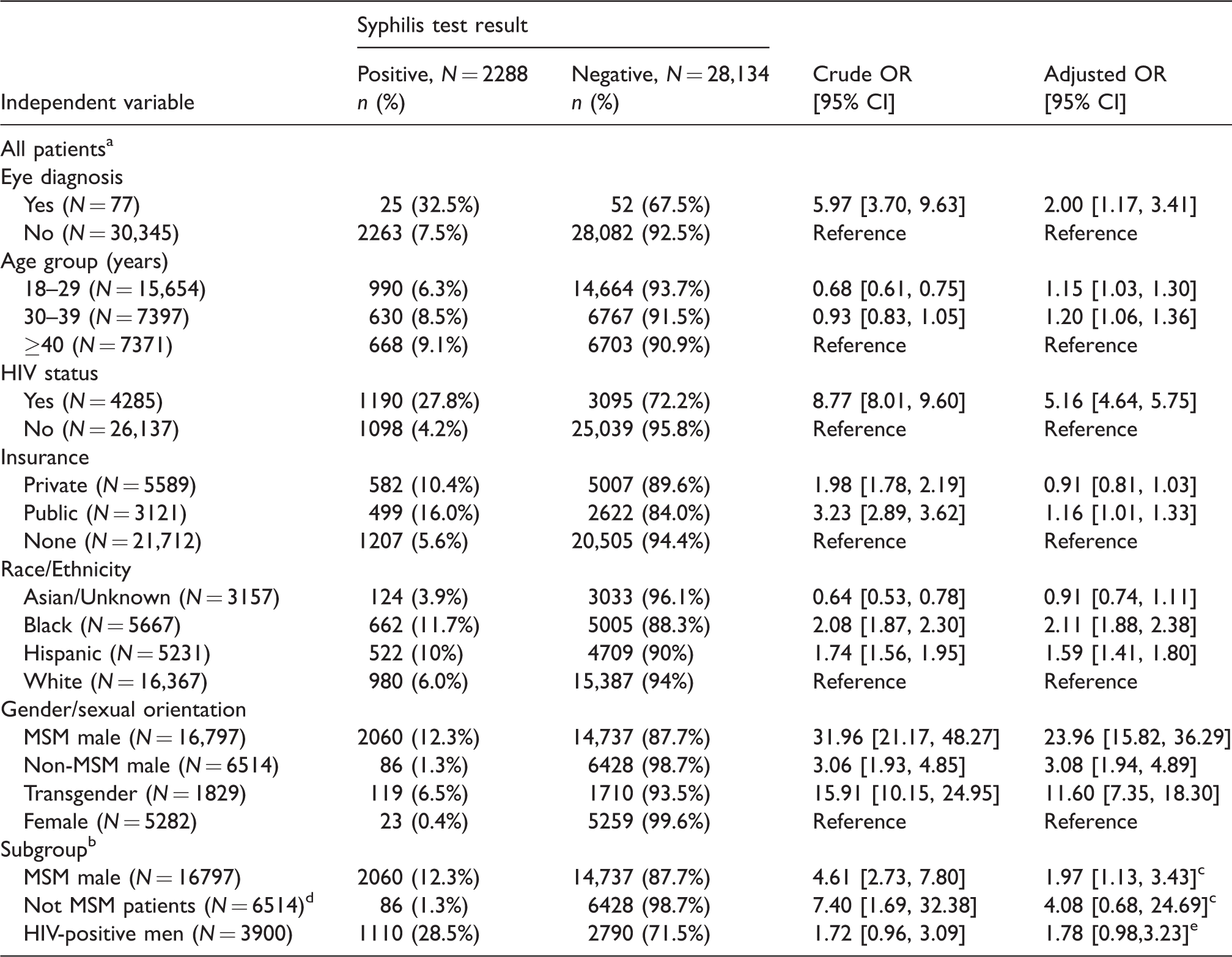
aFor all patients, the crude OR and adjusted OR, simultaneously accounting for all variables, refer to the odds ratio of at least one positive syphilis test in the comparison group vs. the reference group.
bFor subgroup analysis, the crude OR and adjusted OR, accounting for selected covariates, refer to the odds ratio of at least one positive syphilis test in patients with eye diagnosis vs. no eye diagnosis when the analysis set is restricted by the specific subpopulation.
cAdjusted for covariates: Age Group, HIV Status, Insurance, and Race/Ethnicity.
dNot MSM patients included female, Non-MSM male, and transgender.
eAdjusted for covariates: Age Group, Insurance, and Race/Ethnicity.
Discussion
This patient population at a large, urban LGBT health clinic had a high frequency of syphilis tests, but a low prevalence of eye diagnoses. Patients with an eye diagnosis had significantly higher odds of a positive syphilis test result than patients without an eye diagnosis. Even after adjusting for other known risk factors for syphilis, including MSM and HIV status, eye diagnosis was associated with two-times increased odds of a positive syphilis test. However, the MSM and HIV covariates overall had an even stronger association with positive syphilis test results than eye diagnosis. When the subgroup of MSM patients was analyzed, the association between eye disease and a positive syphilis result was significant but slightly attenuated. In the subgroup of non-MSM patients, there was a stronger association between eye disease and positive syphilis tests but the sample sizes were small limiting reliability of these results.
Although rates of ocular syphilis are low in population-based studies, there has been a recent resurgence in cases of ocular syphilis reported in the United States with 0.6% of cases of syphilis consistent with ocular syphilis.3,4 Patients may be more likely to notice and complain of eye symptoms compared to other symptoms associated with various stages of syphilis; therefore, patients with other risk factors for syphilis who present with eye complaints may have a higher likelihood of a positive syphilis test. Of 19 patients referred for ophthalmology examination, only two were diagnosed with ocular syphilis (1 confirmed case of syphilitic iridocyclitis and one case of probable ocular syphilis) or 0.08% of positive syphilis cases due to ocular syphilis. Two additional patients with positive syphilis tests had diagnoses of iridocyclitis and were referred for ophthalmology examination without any record of follow up. Both patients received at least two doses of bicillin for positive syphilis tests; it is unclear if these cases represented early ocular syphilis or missed diagnoses. Patients presented with eye diagnosis less than six months after positive syphilis testing, although this time frame varied significantly per patient.
The patients presenting to this primary care/STI clinic may be more likely to present for eye symptoms and have regular STI testing which may explain the overall low rate of ocular syphilis in this study population. Patients with eye diagnoses were older and were more likely to have private insurance; older patients may have higher risk for eye disease in general and patients with private insurance may have greater health literacy and quality of care. HIV patients regularly had screening for STI with RPR titers at least every six months. Of all, 17% of patients with eye diagnosis and negative syphilis test results based on our algorithm had a bicillin order, suggesting that there was a lower threshold for treatment for high-risk patients. There have been reports of subclinical uveitis in cases of secondary syphilis which can respond to treatment with benzathine penicillin G, although this treatment has been abandoned due to lack of adequate treponemicidal levels in the cerebrospinal fluid (CSF) and ocular fluid.5,6 In the present study, treatment with bicillin may have prevented further development of ocular syphilis in patients who had eye symptoms and positive syphilis test results. A recent report on ocular syphilis cases from various regions in the United States highlighted the variability of clinical presentation, with one-third of cases presenting with red eye or ocular irritation and 50% of cases presenting to primary care or emergency room settings. 2 Delay in diagnosis of ocular syphilis has been associated with increased ocular complications and poorer visual outcomes.7,8
There are several limitations to this study. The retrospective nature of the medical record review, variable methods of syphilis testing, limited information on ophthalmologic examination, and reporting of true infection and stage of infection limit the generalizability of the study results. There may be an overestimation of positive syphilis tests based on RPR titer in patients with multiple tests who have a titer > 1:4 but are clinically negative based on a four-fold decline in RPR titer following prior treatment. Many patients in this study had multiple syphilis tests during the study period, but analysis was limited to patients with at least one positive syphilis test result because of the difficulty in determining true infection versus serofast status in patients with multiple RPR titers >1:4. Sensitivity analysis to confirm true positive results was attempted using the bicillin order as a surrogate for treatment-requiring infection. Not all patients with eye disease had follow-up evaluation with an ophthalmologist, so we were unable to determine if eye symptoms associated with a positive syphilis test were related to ocular syphilis and improved with bicillin treatment or were due to another diagnosis. The eye diagnoses may have occurred before or after the syphilis testing, limiting the ability to find an association between ocular symptoms and STI test results. There were no data available on whether patients with eye diagnoses and positive syphilis test results were referred for lumbar puncture or treatment with intravenous penicillin in addition to intramuscular bicillin.
Clinical advisories were issued by the CDC and the American Academy of Ophthalmology in 2015 regarding rising rates of syphilis and ocular syphilis in the United States. In this study, eye diagnoses were associated with positive syphilis test results. High-risk patients, including those with HIV and MSM, with eye symptoms should have routine STI testing and be referred for complete ophthalmologic examination to identify and treat early stages of ocular syphilis. Further prospective studies and coordination of primary care, infectious disease, and ophthalmologist providers are needed to improve surveillance and identify the risk factors associated with development of ocular syphilis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH grant EY021475.