
Abstract
Vasculitis has long been associated with chronic viral infections, thus the twin perils of the infection and the immune response against it that bedevils the specialties of infection and immunity. After HIV was identified, it too became associated with vasculitic syndromes. Later, hepatitis C virus was also isolated, identified and described with its own spectrum of vasculitic diseases, including hepatitis C virus-associated cryoglobulinaemia. With the increasing prevalence of HIV and hepatitis C virus coinfection, there has come an increasing recognition of the range of vasculitides that can occur in this population leading to significant morbidity, diagnostic and treatment challenges. In this review, we examine the epidemiology, pathogenesis and general principles of treatment of these systemic diseases in HIV/hepatitis C virus coinfected individuals.
Introduction
Summary of the Chapel Hill classification of vasculitides.
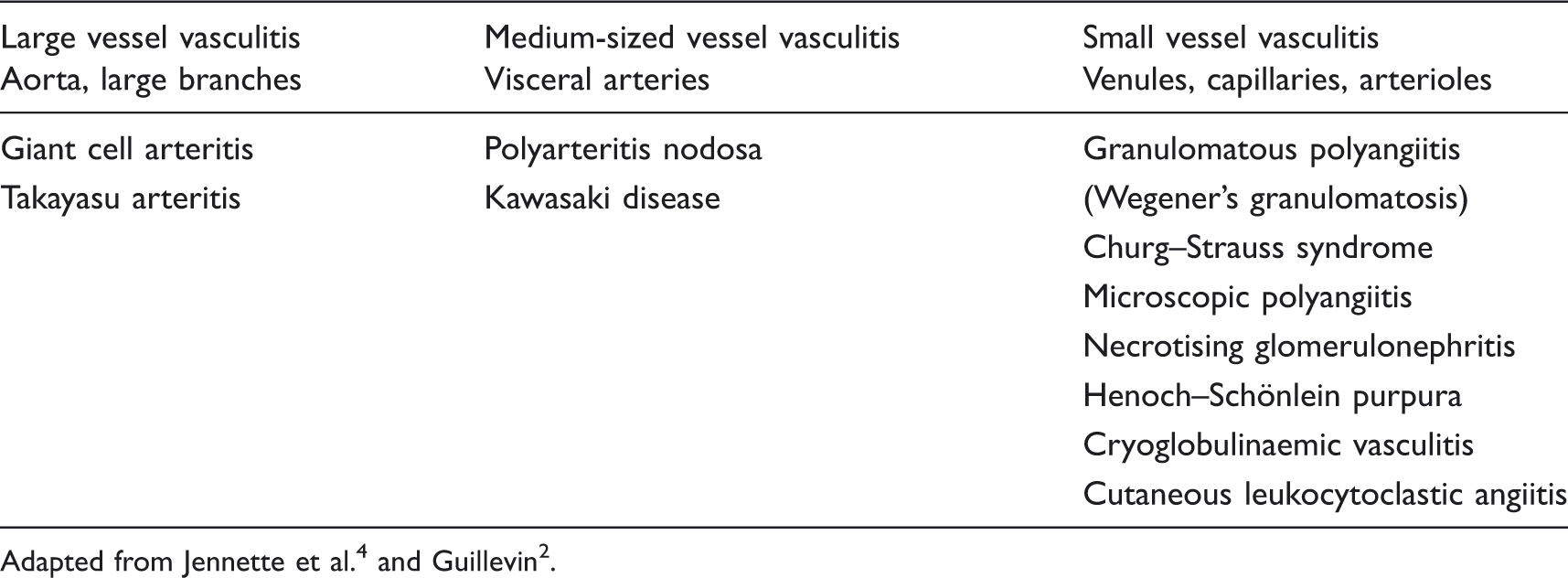
Multiple infectious agents have been linked to vasculitis. A causal relationship, however, has only been determined for a few viral infections. 5 Hepatitis B virus (HBV) has been classically associated with PAN since the 1970s. 6 PAN was previously considered a connective tissue disorder, until a relationship to HBV was noted, with transmission of the disease occurring between household members. 6 Mixed cryoglobulinaemia (MC) was initially thought to be mostly secondary to HBV, but upon the discovery of hepatitis C virus (HCV) in the late 1980s, the significant role of this virus in causing MC was identified. 7 Likewise, since the epidemic began, HIV has been linked to vasculitides affecting all vessels.8–10
It is difficult to fully ascertain a direct causal relationship between HIV and vasculitis given the usual concurrence of other conditions and pathogens, especially viruses such as Epstein Barr Virus (EBV), cytomegalovirus (CMV), HBV and HCV, which are also associated with vasculitis. 10 It may be possible that the welcomed growth in world-wide use of antiretrovirals and the available classes, as well as changes in the pattern of use of these drugs, may alter the vasculitic manifestations of the disease with time. However, evidence at this point is sparse.
Vasculitis in the setting of HIV or HIV/HCV coinfection is uncommon; however, awareness and understanding of the vasculitides involved in HIV and HIV/HCV coinfected individuals is essential due to important differences in the management of such patients. In this paper, we review these conditions, paying particular attention to HIV/HCV coinfection and cryoglobulinaemia. We hope to highlight to HIV physicians that vasculitis is a possible disease entity to be considered in this population, as well as provide some guidance in treatment of these conditions.
Vasculitis in HIV mono-infection
Background
Since the beginning of the HIV epidemic, an extensive array of vasculitides have been described in HIV-infected people.8,10 In one study, prior to the ART era, 23% of symptomatic HIV-infected patients were found to have a vasculitis. Diagnoses included hypersensitivity vasculitis, PAN and Henoch–Schönlein purpura. 11 In the early ART era, the incidence was reported to be approximately 1% of all infected patients and mostly involved the skin, peripheral and central nervous systems, skeletal muscle and less commonly, the lungs, gastrointestinal tract (GIT), oropharynx and the kidneys. 10 This is a higher frequency than seen in other settings. In their cohort of 450 HIV-infected patients, Guillevin et al. found only seven patients with vasculitis.12,13 On the other hand, Zhang et al. 14 recently reported in a Chinese population of 98 consecutive HIV-infected inpatients, that vasculitis was the most commonly seen rheumatic disorder in HIV (20 cases, 20.4%), followed by diffuse infiltrative lymphocytosis syndrome (DILS), lupus-like syndrome and myositis.
Pathogenesis
The mechanisms by which HIV results in vasculitis are not completely understood, other than the common finding of vessel wall inflammation, resulting from cell-mediated or immune complex-mediated inflammation characterised by intimal and medial thickening secondary to hyperplasia of smooth muscles.2,15 Current evidence suggests that pathogenesis is complex and likely to be multifactorial, with histopathology showing diverse changes that reflect probable varying disease entities and pathogenesis. 16 Both direct and indirect effects of HIV on tissue and immune cells, via interactions with superantigens, adhesion molecules, cytokines, growth factors and immune complexes, in addition to host genetics, are likely drivers of the process.10,17,18 There is also a likely role for the immunosuppressive effect of HIV, which results in opportunistic infections by both known and unknown pathogens, potentially triggering autoimmunity through molecular mimicry.10,17,19
The occurrence of HIV-related vasculitides during the different stages of HIV infection is thought to reflect the diversity of pathogenic mechanisms involved, with a mixture of general immune activation and impaired immunity allowing concurrent opportunistic infections, especially in the pre-ART era. 12 There is also evidence of direct HIV infection of endothelia, especially in the setting of low CD4 T cells of <200 cells/µl.2,16,17 HIV-like particles have been found by electron microscopy in the vessels of HIV-infected individuals with necrotising vasculitis, while HIV antigens were detected in the perivascular cells of some patients. 11 Gherardi et al. 20 also demonstrated HIV replication in infiltrating mononuclear cells, involved in necrotising vasculitis of the nervous system. Pathogens that have been shown to cause necrotising vasculitis, regardless of the presence of HIV infection, include CMV, Toxoplasma gondii (CNS vasculitis), parvovirus, Pneumocystis jiroveci (pulmonary vasculitis) and HBV.1,2,10,12 CMV causes GIT, lung, CNS and skin vasculitis, which occurs more commonly in advanced HIV infection. 16
In addition to the depletion of CD4 positive T cells, HIV also leads to dysregulation of the immune response resulting in expansion of CD8 positive T cells and B cells, with a consequent increase in circulating immune complexes and polyclonal hypergammaglobulinaemia. 21 This may explain the presence of detectable autoantibodies, e.g. antinuclear (ANA), antineutrophil cytoplasmic (ANCA) and cardiolipin (ACL) antibodies, often of the low-affinity IgM isotype and unlikely to be of clinical significance.1,3,19,22 ANCA, which are usually seen with the small vessel vasculitides, are found in 20–83% of HIV-infected sera. 23 In small vessel vasculitides ANCA are usually associated with either MPO or PR3 specificity, however HIV-associated ANCA are commonly atypical and do not correlate with symptoms.2,5,6,23–26 There does not appear to be a correlation between the presence of ANCA and the stage of HIV infection or intercurrent infection.7–9,24,25
Vasculitides associated with HIV mono-infection
Vasculitis in the setting of HIV infection has been reported in all types of vessels, including large, medium and small-sized arteries, though the latter are more commonly involved.9,12 As proposed by Johnson et al., 16 vasculitides in HIV-infected people may be divided into four categories, including those that occur in the general population and coincidentally in the setting of HIV; vasculitides due to adverse drug reactions caused by antiretrovirals; those that relate to coinfection with an infectious agent that has a known vasculitic association; and lastly, vasculitides occurring without a recognised aetiological cause but possibly facilitated by HIV.
Primary angiitis of the central nervous system, usually presenting with progressive headache, altered mental state and focal neurological deficit, has been reported in the literature and is believed to occur more frequently in the HIV-infected population.2,8,10,16,21 Melica et al. 27 reported on four patients with this condition, all of whom presented with stroke-like events and in the setting of advanced HIV infection with persistently low CD4 counts despite partial or good control of HIV replication with ART. All patients were of African ethnicity, suggesting a possible ethnic predisposition.
Vasculitic peripheral neuropathy, characterized by distal and symmetrical polyneuropathy with weight loss, myalgias, weakness and leg tenderness, has been reported in 0.1% to 0.3% of patients with AIDS.18,28 Drug-related hypersensitivity vasculitis, typically involving small vessels with leucocytoclastic vasculitis, have been reported with HIV-related drugs. 16 Common medications involved include cotrimoxazole, abacavir, efavirenz and nevirapine. 16
Cases of PAN in HBV-negative HIV-infected patients have been reported in the literature, in patients at variable stages of HIV infection and with variable CD4 counts.2,8,10–12,29 Prevalence appears to be higher in men, accounting for up to 78% of reported cases. 29 HIV-associated PAN tends to present somewhat differently to classic PAN, including more common musculoskeletal symptoms, skin manifestations and peripheral neuropathy.2,16,29,30 Systemic features, such as fevers, are less commonly seen. 29
Kawasaki’s disease is a medium vessel vasculitis that mainly affects children, presenting with fever of greater than five days, mucocutaneous changes, peripheral oedema, rash and cervical lymphadenopathy. It has been reported in both adults and children infected with HIV, especially in the setting of severe immune dysfunction.2,16,31 First reported in 1987, there have now been a total of 20 case reports in the literature of HIV-associated Kawasaki-like syndrome. 31 Stankovic et al. 31 reported on four cases of adult Kawasaki-like syndrome in HIV-infected individuals. Of these, three out of four patients had coinfection with hepatitis (HBV/delta, two cases with HCV coinfection). While HIV-infected adults with Kawasaki-like illness present similarly to non-HIV-affected children, there tends to be more GIT symptoms and less lymphadenopathy. 16 There has been a report of Kawasaki vasculitis presenting after the commencement of ART. 32
Behçet’s disease and a rapidly progressive focal necrotizing vasculitis affecting large vessels, including the aorta, similar to Takayasu’s arteritis, have also been described in the HIV-infected population.21,33
It is worthwhile noting that atypical arterial aneurysms have been reported in young patients with advanced HIV infection, without risk of artherosclerotic disease. 34 While a direct cause was not identified, histopathological features showed both acute and chronic inflammatory cell infiltration, with occlusion of the vasa vasora due to oedema or cellular infiltration, as well as HIV viral proteins being seen within the arterial walls. 34 A small subset of patients tested positive for Treponema pallidum and typhoid on serology and a small number of others cultured various micro-organisms in blood, including Escherichia coli, Staphylococcus aureus and Enterococcus faecalis. 34
Treatment
A detailed discussion of treatment is beyond the scope of this review. If a vasculitis is suspected, patients should typically be referred for management by a specialist service, such as immunology or rheumatology. Briefly, treatment of rheumatic conditions in the HIV-infected is mostly extrapolated directly from experience in the HIV-uninfected population. Evidence specific to treatment of HIV-associated vasculitides is sparse. Corticosteroids are the mainstay of treatment of vasculitis, although cytotoxic agents such as cyclophosphamide or azathioprine may be required particularly in cases where there is evidence of organ-threatening manifestations. 3 Other adjuvant treatments used in non-HIV-associated vasculitis which have been used safely in the HIV-infected population in other settings, include plasma exchange 35 ; monoclonal antibodies such as anti-CD20, in the setting of lymphoma and cryoglobulinaemia treatment as outlined further ahead; anti-TNF therapy, in the setting of rheumatoid arthritis 36 ; as well as intravenous immunoglobulins. 31 Treatment using these agents may be complicated in HIV due to an already immunosuppressed host and diligence is required in assessing for the presence of opportunistic infections, as well as monitoring for drug interactions with antiretrovirals. Cytotoxic agents are generally not recommended for use with CD4 counts <200/mm3. 33 Thus, of particular importance, HIV-infection treatment with antiretrovirals should be pursued with the aim to optimise and maintain CD4 counts. HIV-related vasculitides are thought to respond well to treatment after 1–3 months without recurrence. 9 Drug-related vasculitis typically responds to the cessation or removal of the causative agent, whereas vasculitis due to an infectious pathogen tends to improve with antimicrobial therapy directed against the pathogen and consequent reduction in antigenic burden along with supportive care. 16
Vasculitis in hepatitis C mono-infection
Background
The geographic prevalence of HCV monoinfection varies between 0.003% and >18%, although overall prevalence is decreasing following the introduction of screening of transfused blood products. 37 HCV monoinfection results in chronic infection in up to 80% of patients, of whom 20–30% will develop chronic liver disease.13–15,38–41 HCV infection has been associated with multiple extra-hepatic manifestations, including mixed cryoglobulinaemia, lymphoproliferative disorders, sialadenitis, arthritis, lichen planus, porphyria cutanea tarda, autoantibody production and autoimmune cytopaenias.37,38,41 It is the virus most commonly associated with virus-induced vasculitis. 42 Anti-HCV antibodies were found in 8.7% of patients with autoimmune disorders, the majority of whom are older males, according to a multicentered study by Agmon-Levin et al. in patients mostly from Europe and Latin America.2,43 The most common vasculitis seen associated with HCV infection is mixed cryoglobulinaemia (MC), which affects small- to medium-sized vessels resulting in purpura, arthralgia, membranoproliferative glomerulonephritis, peripheral neuropathy and rarely CNS vasculitis.10,16,17,38,39 Prior to 1989 and the discovery of the HCV, HBV was implicated in the pathogenesis of MC with HBV surface markers noted in cryoprecipitates of patients, a finding not supported by HBV DNA studies.7,18 Since the discovery of the virus, HCV-RNA is detectable in up to 80% of patients with MC.10,17,19,35,39,44 However, MC affects only 10–55% of HCV-infected patients.2,7,12,16,17,37,38
Classification of cryoglobulinaemia.

Pathogenesis
As with HIV, the pathogenesis of MC in HCV infection is complex and multifaceted. HCV is a lymphotropic virus that is able to replicate in B-cells, binds to the cell via CD817,23,38 and infects it, resulting in an increased expression of the B-cell survival factor, B-lymphocyte activating factor (BAFF) also known as BLyS, which in turn leads to increased B-cell survival and autoimmunity.43,47 There is eventual expansion of a monoclonal B-cell population expressing RF, which may also be facilitated by genetic mutations, such as translocation of bcl-2 that leads to overexpression of the antiapoptotic protein. 7 HCV-infected individuals have been shown to have, in their sera, circulating complexes containing HCV antibodies, antigens and viral genome at concentrations higher than in free form, in proportions of 20 to 1000 times higher.7,25,48 These are believed to then deposit in vessel walls, leading to inflammation and vasculitis.26,42
Saadoun et al. 49 looked at the cytokine and gene profile in the nerves of patients with MC neuropathy, in comparison to those with non-inflammatory idiopathic neuropathy and idiopathic PAN. They found that both CD4 and CD8 positive T-cells predominated within infiltrates, suggesting a Th1 type inflammatory response. They also showed upregulation of MIP-1α, MIP-1β and CXCL10 and its receptor CXCR3. 49 T-regulatory cells, which are CD4+ and CD25+, are diminished in HCV MC vasculitis patients. 49 In another study, Saadoun et al. found that Th1-type cytokines, including TNF-α, IL-2 and IFN-γ, are enhanced in HCV-infected patients with MC, compared to those without MC, likely contributing to the observation that these patients have higher rates of cirrhosis.9,50
Cryoglobulinaemic vasculitis is associated with longer duration of HCV infection, advanced age and cirrhosis,7,12 while the presence of cryoglobulins in the absence of vasculitis is associated with female gender, alcohol excess, liver fibrosis and HCV genotypes 2 and 3. 44 Multiple studies report that cryoglobulins are found in up to 60% of chronically HCV-infected patients.18,27,38,42–44 Most of the cryoglobulins in this case are type III, and are often present at low concentrations28,42. However, MC vasculitis mostly consists of type II cryoglobulins.16,40 It follows a benign clinical course in over 50% of cases.16,38 However, mortality is up to 50% within 10 years in those with renal disease.42,44 MC results in a small vessel, immune complex-type, systemic vasculitis. 7 HCV-associated MC tends to result in vasculitis affecting mostly skin (30–100%), peripheral nervous (45–70%), joints (20–83%) and kidneys (2–50%).7,29 Other organs may be involved, including the mesenteric vessels, lungs and cardiac involvement.7,29 Though occurring rarely, there have also been reports of CNS vasculitis associated with HCV and MC resulting in cerebral ischaemia or haemorrhage.30,39
Other than MC, HCV infection has infrequently been associated with multiple other types of vasculitides, including Wegener’s granulomatosis and giant cell arteritis.2,38 HCV has been found in 5–12% of PAN sufferers,7,16,29,38 and it is thought to be the direct result of deposition of HCV-containing immune complexes within vessels, leading to direct inflammation.2,42
Treatment
Treatment of HCV-associated MC is dependent on the severity of symptoms and extent of end-organ involvement.31,42 Viral clearance and antigen load suppression is the goal, with elimination leading to resolution of symptoms and signs and sustained virological response leading to complete recovery in the majority of patients.16,31,40,51 Nityanand et al. showed that circulating immune complexes and cryoglobulins contain HCV antibodies, antigens and genome, and that these reduced with treatment of HCV.16,48 HCV treatment should be considered as first line therapy in mild to moderate disease, with an extended duration of treatment of 48 weeks for HCV genotypes 2 or 3 and up to 72 weeks for genotypes 1 or 4.32,51 Combination therapy with pegylated interferon alfa (pegIFN alfa) and ribavirin has been shown to provide good results.21,52 Little is known about the impact of newer genotype 1 agents, such as boceprevir; however, given its success in reducing viral load, one would expect good results in reducing cryoglobulins. With interferon remaining a mainstay of treatment, it is important to note that interferon itself has the potential to exacerbate autoimmune disease and has rarely been documented to cause vasculitis.33,41
Plasmapheresis and systemic immunosuppression, including glucocorticosteroids, may be required in severe disease especially in the setting of vital organ involvement, such as membranoproliferative glomerulonephritis, peripheral or CNS neuropathy, severe skin disease, cardiac or gastrointestinal involvement.3,42 A consensus, proposed by the Italian Group for the Study of Cryoglobulinemia, which reviewed 150 published cases of MC treated with rituximab, has recommended the use of this drug over other treatments such as glucocorticoids, immunosuppressants or plasmapheresis.33,51 Rituximab, a humanized murine monoclonal antibody to CD20, expressed on pre-B lymphocytes and mature lymphocytes, has been used successfully by various groups.9,51 It has been shown to effectively normalise disturbances of peripheral B and T-cell homeostasis, including expansion of regulatory T-cells with a decrease in activated CD8+ T-cells. 53 Rituximab has been shown in some cases to increase the HCV viral load, although this rarely translates into clinical disease. 51 Other cytotoxic agents used include cyclophosphamide, azathioprine and mycophenolate mofetil. 41
HIV–HCV coinfection and vasculitis
Background
Coinfection with HIV and HCV is a growing problem, occurring at rates of 50–80% in intravenous drug users and in up to 30% of all HIV-infected individuals.37,38,40,41,54–56 Coinfection with HIV results in increased HCV RNA levels, an accelerated natural course and earlier progression to cirrhosis,37,57 while making HCV persistence more likely after acute infection and decreasing the chance of successful treatment with HCV therapy.55,57,58 Coinfection may also increase the risk of progression to AIDS and AIDS-related deaths, although this may be genotype associated, with genotype 1 being found to have an association with lower CD4 counts and increased risk of AIDS-related mortality.39,56,59
Immunologically, the two viruses behave differently in chronic infections. HIV tends to induce CD8+ T cell responses, in comparison to HCV monoinfection, in which virus-specific CD8 cells are rarely found in peripheral blood. 54 In coinfection, due to the HIV, there is a reduction in HCV-specific CD4 T cells, which play an important role in secreting IFN-γ and thus antiviral response.54,58 The interplay between the two viruses and the various aspects of the immune system makes MC cryoglobulinaemia in coinfection an interesting entity to study.
In considering the general role of coinfection on other rheumatic manifestations, Zhang et al. 14 found that rheumatic manifestations were more likely to occur in patients coinfected with HIV/HCV compared with HIV alone (15.56 vs. 37.74% P < 0.05). In a prospective cross-sectional study of HCV, HIV mono-and coinfected patients, Woitas et al. 60 found that cryoglobulins, RF and non-organ-specific antibodies were significantly associated with HCV monoinfection, but uncommon in HIV/HCV coinfection, whereas, other autoantibodies, including anti-thyroglobulin and anti-cardiolipin antibodies were significantly increased in coinfection. The presence of antibodies did not necessarily correlate with disease and usually was not clinically significant. 60
Cryoglobulins in coinfection
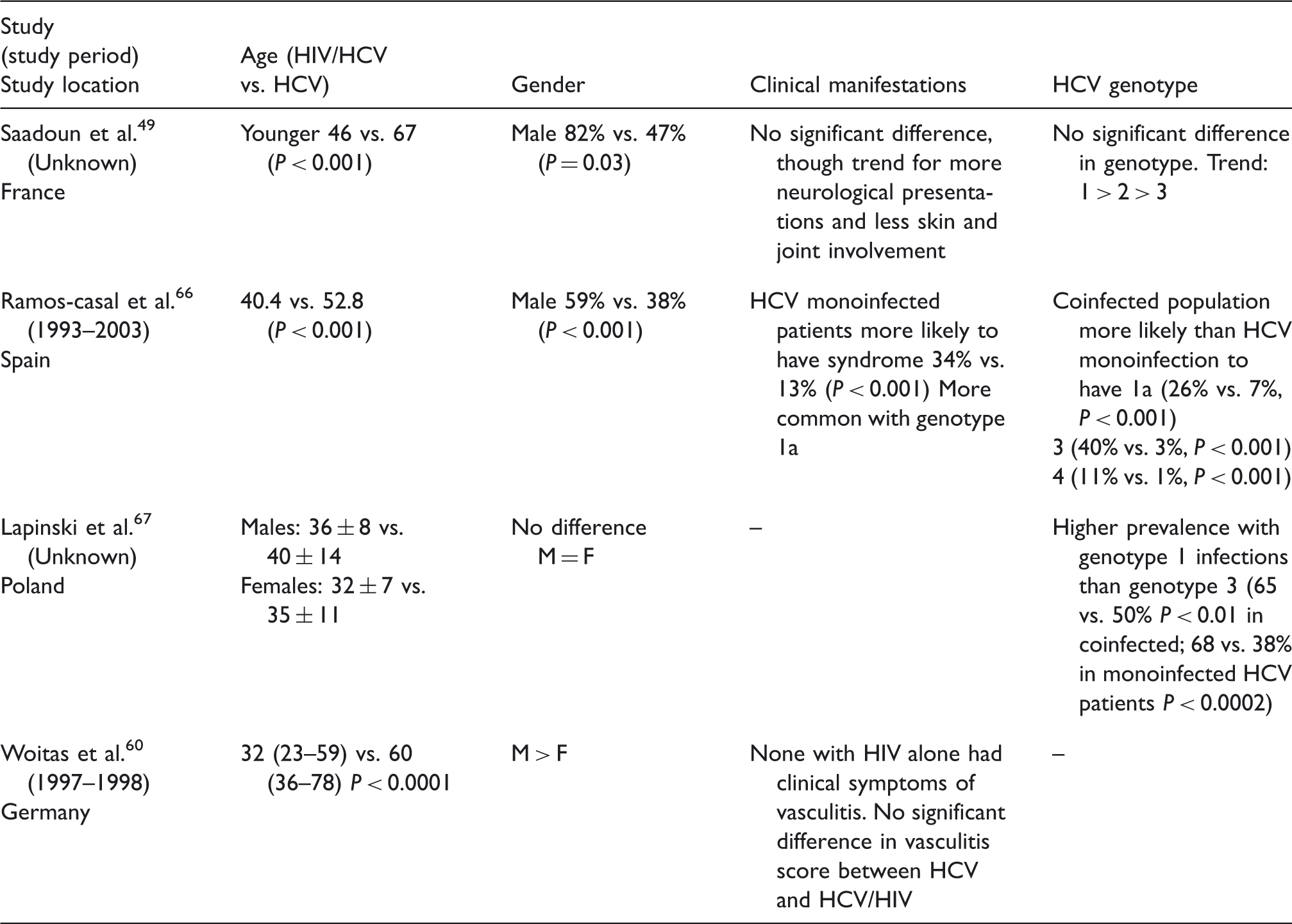
Summary of studies related to HIV, HCV and HIV/HCV infections and cryoglobulinaemia.

Clinical presentation
Characteristics of HIV-HCV coinfected patients with cryoglobulinaemia.
Role of CD4 count and viral load
The prevalence of HIV-associated cryoglobulinaemia may correlate with CD4 count, although the evidence here is again conflicting. Aaron et al. and Kosmas et al. noted higher prevalence of cryoglobulinaemia with lower CD4 counts of <200 cells/µL, while Dezzutti et al. noted an increased prevalence with CD4 < 500 cells/µL.13,62,69 Contrary to this, Bonnet et al. 61 noted a positive trend for increased prevalence of cryoglobulinaemia with CD4 count of >350 cells/µL. This correlates with previously reported cases, in which patients had resolution of symptoms and disappearance of cryoglobulinaemia upon infection with HIV and subsequent immunosuppression, with a drop of CD4 from 337 to 21 cells/µL. 70 Another case report outlines the emergence of cryoglobulinaemic symptoms upon immune restoration and increase in CD4 from 70 to 567 cells/µL. 71 However, a number of other groups have noted no relationship between the presence of cryoglobulins or cryoglobulinaemic symptoms to CD4 cell count.64,66,68,72
There seems to be more agreement between the various studies on the role of HIV viral load on cryoglobulinaemia. A higher HIV viral load tends to correlate more with the presence of cryoglobulins.13,61,72 One group however showed no significant association, 64 and another reported lack of change to the cryocrit with reduction in the HIV viral load. 68
Very few data are available regarding the effect of ART on the prevalence of cryoglobulinaemia and its associated vasculitis. One group reported a lower prevalence following the introduction of ART, 13 while another showed a positive trend to increased cryoglobulinaemia in patients not on ART. 61 However, a number of other groups did not show a correlation.64,67,68,69
Treatment
The possible association with higher viral loads and cryoglobulinaemia suggests that ART has an important role in the treatment of MC-associated vasculitis, although there is no good evidence to support this. As described previously, the treatment of vasculitides in the setting of HIV and thus an immunosuppressed host poses an important challenge and should be done with great caution. Cytotoxic agents are generally not recommended for use with CD4 counts of <200/mm3. 33 The principles of treating MC however are overall unchanged with virus clearance remaining as the main goal of therapy. The treatment of HCV is evolving with the introduction of newer agents, however it remains to be seen how this will impact on MC.
Conclusion
This review provides a short summary of vasculitis in HIV, HCV and HIV/HCV coinfection, with a particular focus on cryoglobulinaemic vasculitis in both populations. It highlights that vasculitic immune phenomena can occur despite the apparent immunosuppressed state of HIV, so that patients are on the one hand affected by immunosuppression and on the other by an aberrant immune response. Treating doctors have to balance the effects of further immune suppression against the effects of the vasculitic illness. Importantly however, the presence of antibodies, or indeed cryoglobulins, in serum does not necessarily indicate disease. With the increasing prevalence and survival rate of HIV patients, as well as coinfection with HCV, it is possible that the prevalence of vasculitides associated with these conditions will also increase, though the widespread use of ART and newer HCV agents may counteract this. Regardless, it is important to continue to be vigilant in assessing patients and consider these potentially important and life threatening conditions as part of routine patient management.
Footnotes
Acknowledgements
We would like to acknowledge Dr Edwina Wright for her review of the manuscript.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.