
Abstract
The clinical severity of human infection with the novel influenza virus A/H1N1v has not been completely defined, especially in HIV/hepatitis C virus (HCV) infected patients. Although most patients develop mild to moderate symptoms, severe disease may occur in a limited proportion of cases. We report the case of a 44-year-old man infected with HIV and HCV with a high CD4 cell count who developed acute respiratory distress syndrome associated with influenza virus A/H1N1v infection. The patient recovered completely after oseltamivir therapy and mechanical ventilation.
CASE REPORT
Human infection with the novel influenza virus A/H1N1v first occurred in Mexico in March 2009. 1 Since then, several epidemic waves have affected an increasing number of countries in both the northern and southern hemispheres. 2
The clinical severity of human infection with the novel influenza virus has not been completely defined. Symptoms of influenza A/H1N1v infection are indistinguishable from those of seasonal influenza. 3 According to the Centers for Disease Control and Prevention (CDC), 4 infection with the influenza virus A/H1N1v should be considered in the differential diagnosis of patients with acute febrile respiratory illness who have been in contact with persons with confirmed influenza or reside in areas where influenza has been reported. Although most patients develop mild to moderate symptoms, severe disease may occur in a limited proportion of cases. Estimated case–fatality ratio is 0.048%. 5
HIV-induced immunosuppression has also been reported to be a risk factor for influenza complications. 6 Furthermore, hepatitis C virus (HCV) infection has been associated with severe influenza infection despite vaccination. 7
We report hereby the case of a 44-year-old man co-infected with HIV (CDC stage A3) and HCV (Genotype 1a), who developed severe pneumonia associated with influenza virus A/H1N1v infection. At the time of influenza symptoms onset, the patient was on antiretroviral therapy (ART) (lopinavir/ritonavir, tenofovir and emtricitabine) and had undetectable HIV-RNA and CD4+ 474 cells/mm3. Child-Pugh score was A, his grade of hepatic fibrosis measured with transient elastography was 11.8 kPa (F3) and HCV load was >5,000,000 cp/mL. The patient was an ex-injecting drug user and a current tobacco smoker. He reported close contact with family members with influenza-like illness.
The patient was admitted to our hospital with a presumptive diagnosis of community-acquired pneumonia. Four days before, he had developed fever, headache, dry cough, muscle pain and worsening dyspnoea. On physical examination, he was febrile (38.8°C) and dyspnoeic, his heart rate was 98 beats/minute, and arterial blood pressure 105/65 mmHg. Laboratory tests showed 7650 leukocytes/mm3 (81.8% neutrophils, 13.8% lymphocytes) and platelets of 59,000/mm3; total bilirubin was 48 µmol/L, albumin 38 g/L, aspartate transaminase 118 U/L, lactate dehydrogenase 338 U/L and C-reactive protein 27.1 mg/L. His arterial blood gas results on room air showed pH 7.42, pO2 54.1 mmHg, pCO2 31.6 mmHg, sAO2 87.2%. His chest X-ray showed bilateral infiltrates (Figure 1). Antibiotic therapy with imipenem/cilastatin 1 g thrice daily plus clarithromycin 500 mg twice daily and empiric treatment with oseltamivir 75 mg twice daily was initiated. On day 3, reverse transcriptase-polymerase chain reaction for influenza A/H1N1v performed on nasal and pharyngeal swabs was positive. On the same day, because of the development of acute respiratory distress syndrome (ARDS), despite non-invasive positive pressure ventilation (Figure 1), he was transferred to the intensive care unit (ICU) where he received mechanical ventilation, broader spectrum empiric antibiotic therapy and circulatory support. ART was temporarily suspended. Blood cultures for bacteria and rapid urinary antigen test for Streptococcus pneumoniae and Legionella pneumophila performed on admission samples tested negative. During his ICU stay, a routine plasma Aspergillus galactomannan antigen was positive and bronchioalveolar lavage microscopy was also positive for Aspergillus spp.; thus, voriconazole was administered for 14 days. The patient developed severe anaemia and thrombocytopenia requiring transfusions. On day 30, after improvement of clinical and respiratory parameters, the patient was extubated, and two days later he was discharged from the ICU.
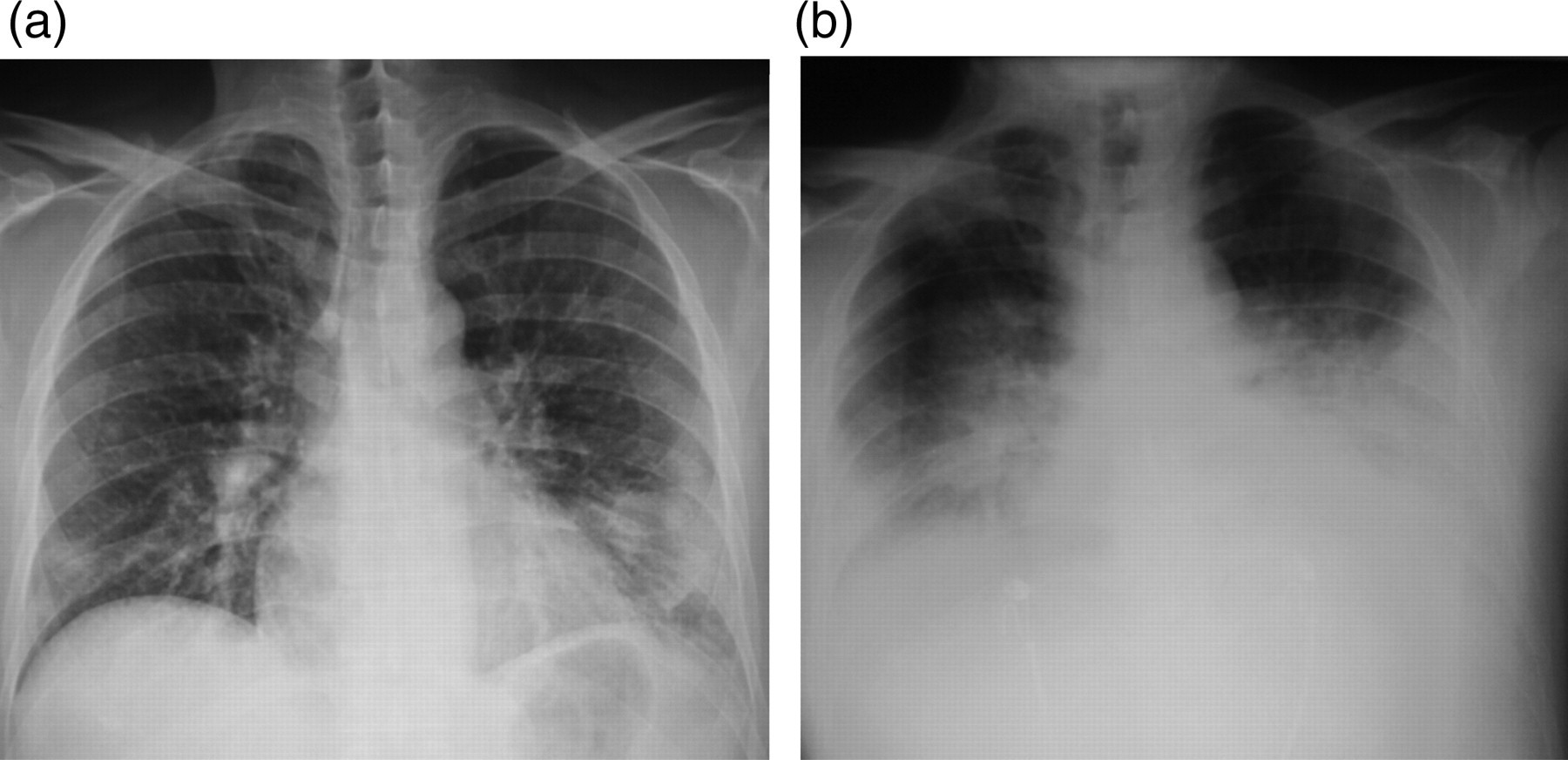
A 44-year-old man infected with HIV (CDC stage A3) and HCV (Genotype 1a) and current tobacco smoker was admitted with fever (38.8°C), dry cough, headache, diffuse myalgias and dyspnoea. Chest X-ray showed bilateral infiltrates (a). He was transferred to the intensive care unit after the development of ARDS (b) where he received mechanical ventilation HCV = hepatitis C virus; ARDS = acute respiratory distress syndrome
The clinical course of influenza A/H1N1v infection in HIV-infected patients seems to be mild and similar to that of HIV-negative controls in both adult and paediatric populations. 8,9 However, is should be considered that most HIV-patients had received antiviral treatment because they were considered at high risk of complications. 8,9
This is one of the few clinical reports of a severe course of the novel influenza virus infection in an HIV-infected patient. A recent article reported a fatal case in a 39-year-old HIV-positive woman with diabetes despite mechanical ventilation. In that case, a rapid influenza A/H1N1v test was negative, causing a delay in the initiation of oseltamivir treatment, started only on day 3. 10
Attention should be given to the possible interactions between oseltamivir and ART in HIV-infected patients with suspected influenza A/H1N1v. Oseltamivir use has been associated with neuropsychiatric reactions; therefore, inhibition of brain P - glycoprotein by boosted protease inhibitors (PIs) may result in an increased risk of neurotoxicity. 11,12 The potential interaction between oseltamivir and renally excreted nucleoside reverse transcriptase inhibitors (NRTIs) warrants caution in patients with renal impairment. Therefore, the co-administration of PIs, NRTIs and oseltamivir should be carefully monitored for adverse events. Based on their pharmacokinetic properties, no significant interaction between oseltamivir and non-NRTIs, CCR5 inhibitors or integrase inhibitors are expected. 13 In our patient, consideration his stable HIV status and the severe clinical condition, ART was temporally suspended and resumed as the patient recovered.
The role played by HCV in such a severe clinical case of influenza A/H1N1v infection is uncertain. However, some studies have shown impaired cytotoxic T-lymphocyte function in HCV carriers, associated with a prolonged influenza-related illness and viral shedding. 14 While the fatal case reported by Klein et al. had <200 CD4 cells/mm3, our patient had >450 CD4 cells/mm3. This suggests that the development of ARDS in HIV-infected patients may not be exclusive to patients with very low CD4+ counts but may occur also in patients with relatively high CD4+ counts, as observed in other reports. 15 In our case, HCV could have favoured the development of severe disease in the presence of moderate HIV-related immunodeficiency.
Although no definitive conclusions can be drawn by single case reports, influenza A/H1N1v should be suspected and empiric oseltamivir treatment should be started promptly in HIV/HCV co-infected patients presenting with influenza-like illness and severe respiratory symptoms.