
Abstract
HIV-infected individuals have poor responses to hepatitis B vaccine and may have decreased durability of post-vaccination immunity. Retrospective chart review was conducted for HIV-1 positive individuals aged ≥18 years who received hepatitis B vaccine at an urban HIV clinic. A total of 309 patients completed three doses and 178 had post-vaccine serology testing after the third dose. In multivariate analysis, time between the third dose and the first post-vaccine serology testing at 180–359 days (OR = 0.077, p = 0.049) and at ≥360 days (OR = 0.065, p = 0.019) were associated with poor vaccine responses. A significant decrease in seropositivity appeared as early as 180 days after the third vaccine dose, suggesting a rapid loss of vaccine-acquired hepatitis B surface antibody in HIV-infected persons. Our findings suggest that hepatitis B surface antibody should be tested at 6 to 12 months after completing primary vaccine series in order to detect early secondary vaccine failure.
Keywords
Introduction
HIV has spread globally into regions in which hepatitis B virus (HBV) has long been prevalent. HIV and HBV coinfection is associated with an increased risk of chronic hepatitis B, a higher prevalence of cirrhosis and hepatoma, and higher liver-related mortality highlighting the need for HBV prevention by vaccination.1,2 However, HIV-infected individuals have poor response rates to hepatitis B vaccines, and some data suggest decreased durability of post-vaccination immunity compared to immunocompetent persons. Although more than 90% of healthy individuals develop protective immunity against hepatitis B after a standard three-dose vaccine schedule, response rates among HIV-infected persons are reported to be 17.5% to 62%.3–13 It has been recommended that post-vaccination serologic responses to HBV vaccination should be checked 1 to 2 months or 6 to 8 weeks after administration of the last dose of the vaccine series for HIV-infected persons to screen for primary vaccine failure.14,15
Factors previously reported to be associated with hepatitis B vaccine responses in HIV-infected individuals include age, CD4 cell counts at time of the first dose of vaccine, HIV viral suppression, female gender and pre-vaccine nadir CD4 cell counts.3,6,9,10,16–27 Loss of vaccine-induced hepatitis B surface antibody (HBsAb) has been reported in homosexual individuals, 28 HIV-infected haemophilia patients29,30 and HIV-infected patients without haemophilia,9,16,17 although all those studies were conducted in small numbers of patients. HIV-infected persons who developed HBsAb after vaccination should have follow-up HBsAb testing to assess post-vaccine immunity and the need for either a booster dose or repeat vaccination series if HBsAb becomes negative.15,31,32 We conducted a retrospective study at an urban HIV clinic on durability of vaccine-induced hepatitis B surface antibody and factors associated with vaccine responses including time of testing in a larger study population.
Methods
Study population and design
Retrospective chart review was conducted for HIV-1 positive individuals who received hepatitis B vaccines at Peter Krueger Clinic from 1 January 2000 to 31 December 2010. Peter Krueger Clinic is an adult ambulatory medical care clinic for HIV patients in Manhattan, New York. The male to female ratio of the clinic patients was approximately 7 to 3; approximately 50% of the patients were Hispanic and 30% were African American. All patients were scheduled to receive a vaccine dose at 0, 1 month and 6 months; however, some patients were vaccinated at intervals which deviated from the planned schedule. Inclusion criteria for the study included age 18 years or older, having a negative pre-vaccination HBsAb and hepatitis B surface antigen (HBsAg) tests and having received a total of three 20-mcg intramuscular doses of recombinant hepatitis B vaccine (Engerix B, GlaxoSmithKline) regardless of any deviation from the intended vaccination schedule; patients with isolated hepatitis B core antibody (HBcAb) were considered to need vaccination and were included in analyses. Clinical data were collected regarding age, gender, race/ethnicity, smoking, alcohol use, drug use, diabetes mellitus, chronic kidney disease, lymphoma, malignancy other than lymphoma, chemotherapy use, splenectomy, hepatitis C antibody, HCV viral load, pre-vaccine nadir CD4 cell counts, AIDS at time of the first vaccine and exact dates of all vaccine doses. We used the CDC case definition for AIDS.33,34 CD4 cell counts, HIV viral load and antiretroviral therapy (ART) were examined at time of the first vaccine dose and at time of post-vaccination serologic testing. Seroconversion was defined as developing an HBsAb titer ≥10 mIU/mL. The study was approved by the institutional review board of Beth Israel Medical Center in New York.
Statistical analysis
Stata Release 12 (StataCorp LP, College Station Texas) was used for statistical analysis. Categorical variables were compared by using chi square test or Fisher’s exact test and continuous variables were compared by using two-sample t-test. Two-sided p values <0.05 were considered significant. Covariates that were statistically significant in univariate analysis or considered clinically relevant were included in the multivariate analysis.
Results
Baseline characteristics and univariate predictors of serologic response.
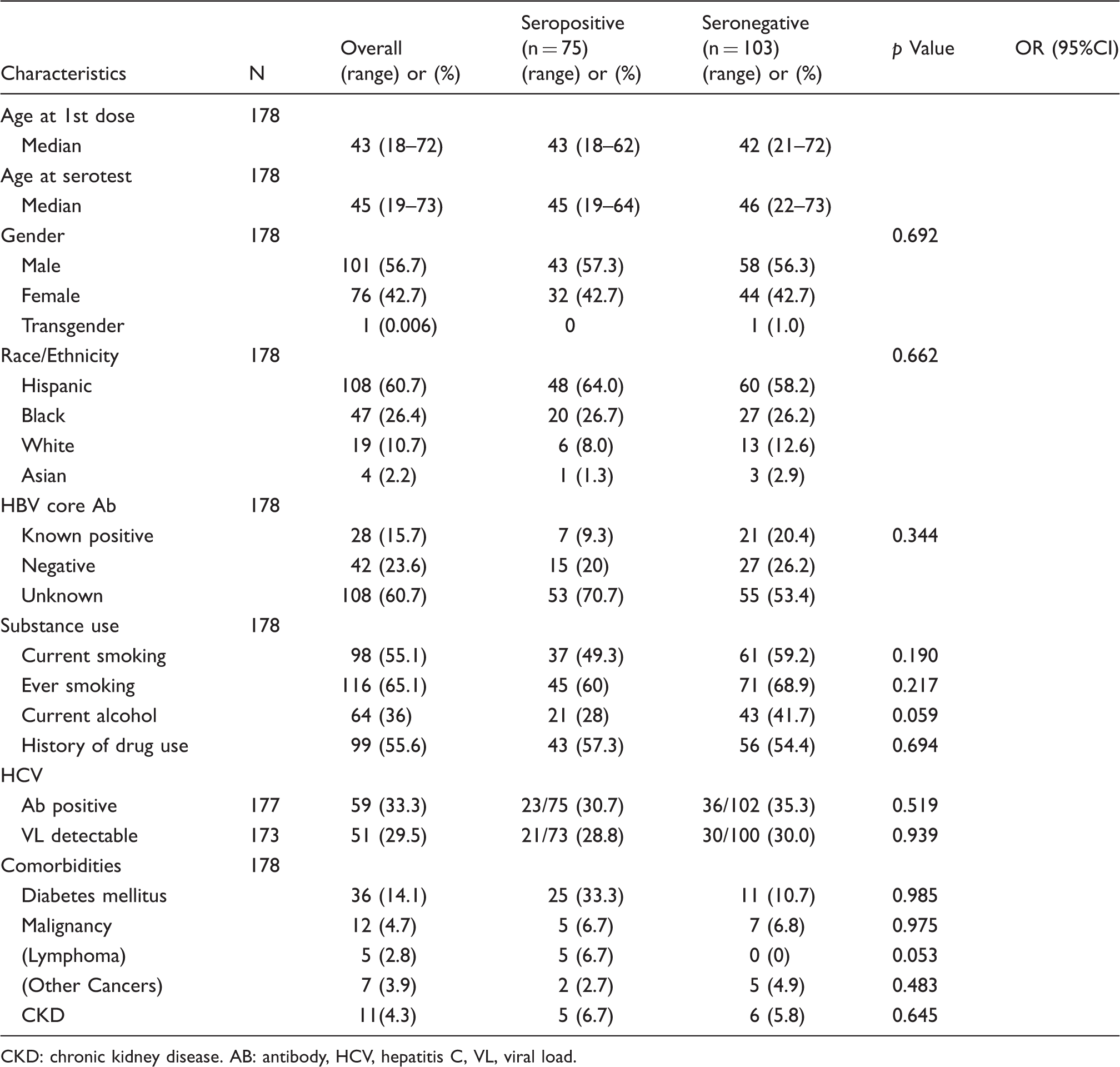
CKD: chronic kidney disease. AB: antibody, HCV, hepatitis C, VL, viral load.
Baseline characteristics and univariate predictors of serologic response.
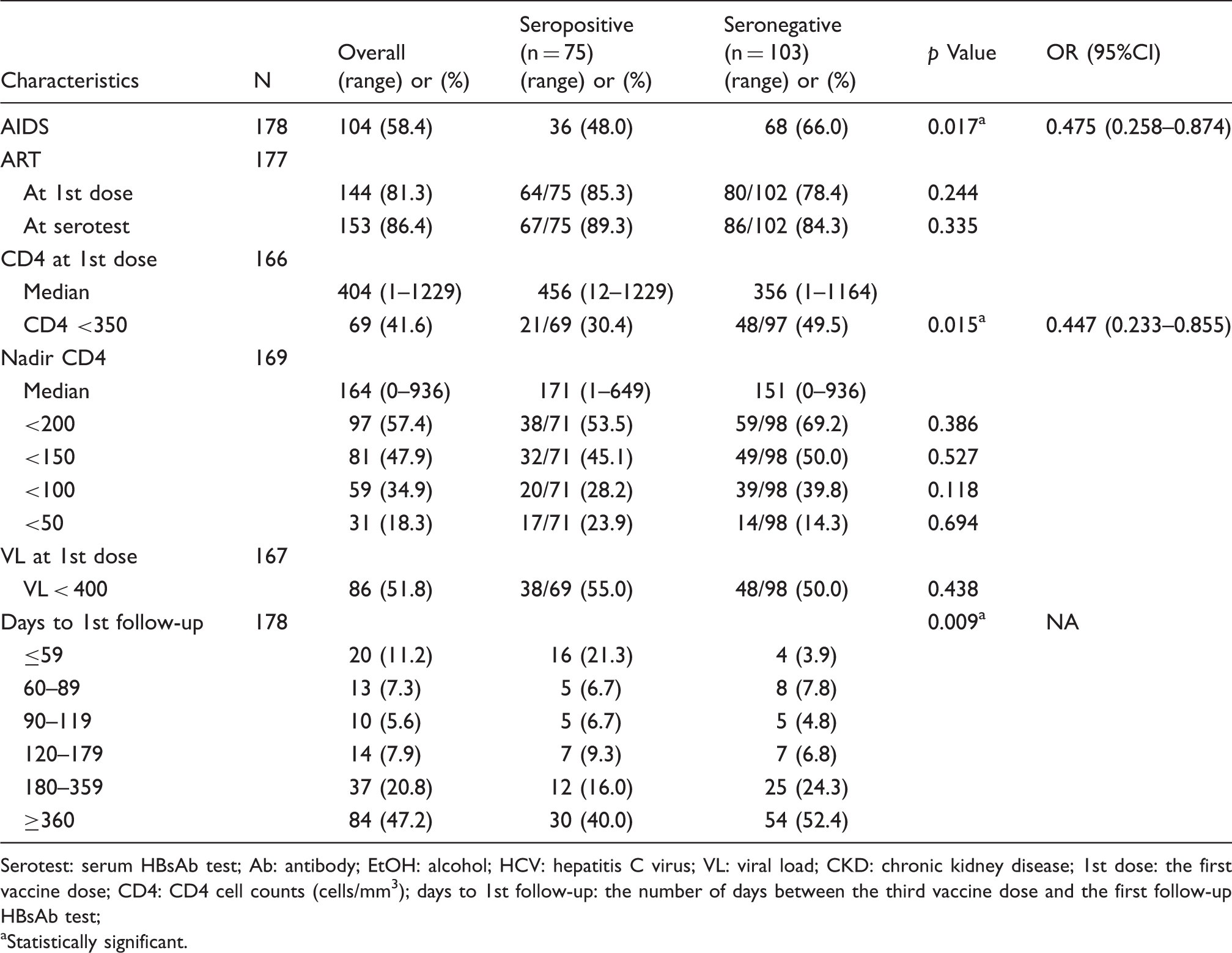
Serotest: serum HBsAb test; Ab: antibody; EtOH: alcohol; HCV: hepatitis C virus; VL: viral load; CKD: chronic kidney disease; 1st dose: the first vaccine dose; CD4: CD4 cell counts (cells/mm3); days to 1st follow-up: the number of days between the third vaccine dose and the first follow-up HBsAb test;
Statistically significant.
Multivariate predictors for serologic response.
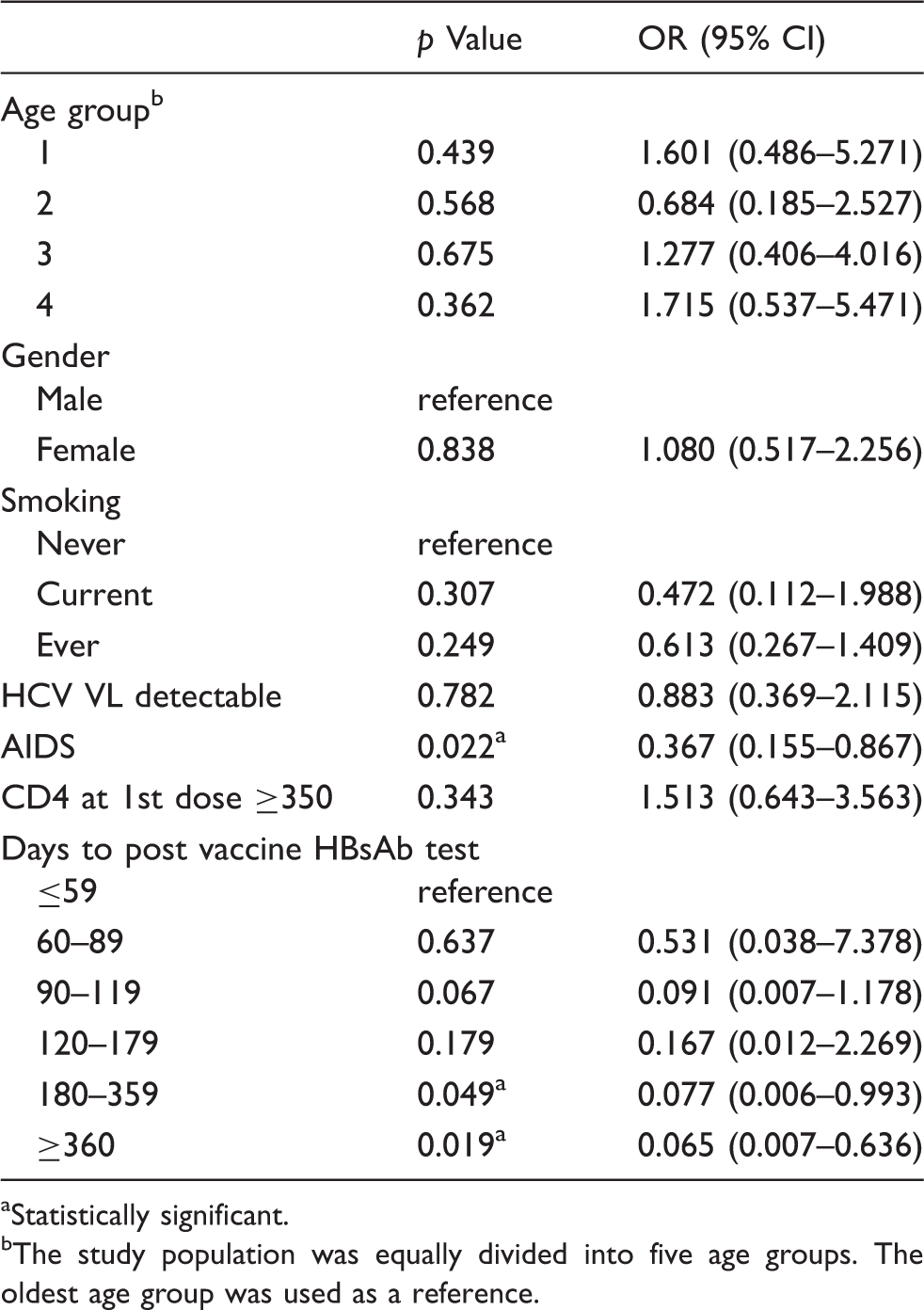
Statistically significant.
The study population was equally divided into five age groups. The oldest age group was used as a reference.
Discussion
We found that rates of HBsAb seropositivity were significantly decreased among those tested ≥180 days after the third vaccine dose. The significant decrease in seropositivity rates over time is suggestive of a rapid loss of vaccine-acquired immunity in primary responders. Prior studies demonstrated the loss of vaccine-acquired HBsAb in small numbers of HIV-infected patients, even in those with CD4 cell counts >200 cells/mm3, and with a variety of vaccine dosing regimens.9,16,17 For example, Rey et al. 9 reported the follow-up serologic testing for vaccine responders in a rapid vaccine schedule. In their study, 20 patients received 20 mcg of recombinant hepatitis B vaccine at 0, 1, 2 months. The number of initial responders were 11 (55%) and seven more patients responded to additional three booster doses, which improved overall response rate to 90%. However, 12 months after the first vaccine dose (10 months after the last vaccine dose) only 58.8% (10/17) of those patients had positive HBsAb. All of those patients had CD4 cell counts >200 cells/mm3 and median CD4 cell counts and median nadir CD4 cell counts were 470 cells/mm3 and 286 cells/mm3, respectively. Cruciani et al. 17 vaccinated HIV-infected persons using high dose (40 mcg) hepatitis B vaccine given at 0, 1, 2 months. In their study, 65 patients completed the vaccine schedule and 39 (60%) patients had primary responses. 17 Of 26 initial non-responders, 11 patients responded to the first booster dose and eight responded to the second booster dose, which improved overall response rate to 89%. However, the HBsAb positive rate decreased to 70.6% (41/58) at 1 year and 32.7% (19/58) at 2 years after the last vaccine dose. The median CD4 cell counts of the enrolled patients in their study were 533 cells/mm3.
Our data, in a population with lower median CD4 cell counts, suggest that loss of vaccine-acquired HBsAb may start within the first 180 days after the third dose in the primary vaccine responders, suggesting high and rapid rates of secondary vaccine failure. Post-vaccination testing for serologic response is recommended for HIV-infected persons 1 to 2 months or 6 to 8 weeks after administration of the last dose of the vaccine series14,15; this would detect primary vaccine responses but may be too soon to detect early secondary vaccine failure. Furthermore, it may be impractical to have patients return for a visit solely for HBsAb testing and may be more practical to integrate testing at regularly scheduled visits. Considering that guidelines suggest that HIV-infected patients have follow-up visits every 3 to 6 months, it may be more reasonable and practical that the first post-vaccination serology testing should be performed three months after the last dose in order to detect primary vaccine responses. Our data suggest that post-vaccination serology testing at 6 to 12 months after the last dose should also be considered in order to detect early secondary vaccine failure. The effect of CD4 cell counts on hepatitis B vaccine response in HIV-infected individuals has been repeatedly reported,3,6,9,10,17,21–27 and our study also showed that both CD4 cell counts at time of the first vaccine and pre-vaccine nadir CD4 cell counts were associated with vaccine response. Hepatitis B vaccine schedules for HIV-infected individuals have been investigated with different dosages and intervals17,20,27,35,36; the use of higher and more doses have been shown to improve vaccine responses but not HbsAb retention. The recent CDC recommendation suggests that adult patients receiving haemodialysis or with “immunocompromising conditions” should receive 1 dose of 40 mcg (Recombivax HB) administered on a three-dose schedule or two doses of 20 mcg (Engerix-B) administered simultaneously on a four-dose schedule at 0, 1, 2 and 6 months, 37 which could be taken to apply to patients with HIV. While cumulative data indicate better response rates with higher doses and more frequent vaccination, such regimens are still not considered standard of care for HIV-infected patients and studies of their effectiveness and durability are lacking. The optimal hepatitis B vaccine regimens in HIV-infected individuals remain uncertain. HIV patients with higher CD4 cell counts may develop and retain HBsAb with standard hepatitis B vaccine regimen. On the other hand, those with lower CD4 cell counts may not respond to even higher or more frequent dose schedule. Individualized strategies including vaccine regimen based on expected responsiveness, practical timing of follow-up serology testing and actual hepatitis B risk in nonresponders should be investigated to achieve the best outcome in preventing hepatitis B infection for HIV patients. Randomised controlled trials examining the promising hepatitis B vaccine regimens are needed.
Limitations of this study include the fact that post-vaccine series serologic testing was not available for all patients vaccinated in clinic. Further, baseline HBcAb data were not available for all analyzed patients, hence HBcAb could not be included as a variable in multivariate analyses; also, early and serial HBsAb tests after vaccine series completion were not available and therefore we could not directly differentiate between primary and secondary vaccine failure. Further, post-vaccine immunity was assessed using a routine clinical HBsAb assay reporting results as ≥10 mIU/mL; quantitative HBsAb titers or determination of the immunity with antibody titers in excess ≥100 mIU/mL would be valuable. 38 Additionally, the lack of HBV DNA data for those with isolated HBcAb positive is also a limitation. Nonetheless, the progressively lower HBsAb seropositivity rates over time strongly suggest secondary vaccine failure as the operative mechanism and follow-up HBsAb testing at 6 to 12 months may be indicated to detect secondary vaccine failure.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.