
Abstract
Transient detection of hepatitis B surface antigen (HBsAg) following hepatitis B vaccination is a rare but recognized phenomenon that may be misinterpreted as acute hepatitis B virus (HBV) infection. We report a case illustrating this diagnostic challenge in an HIV pre-exposure prophylaxis (PrEP) user. A 36-year-old man presented in October 2025 for PrEP initiation. He reported condomless sex with multiple male partners and occasional on-demand use of tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) obtained from a partner. Screening for sexually transmitted infections in August 2025 showed negative viral hepatitis serologies. Two days prior to the PrEP consultation, he received a combined hepatitis A/B vaccine in preparation for travel to Thailand.Routine baseline testing revealed isolated HBsAg positivity. The patient was asymptomatic and recalled for further evaluation. Repeat testing eight days later showed HBsAg negativity, newly positive anti-HBs antibodies, undetectable HBV DNA, negative hepatitis D serology, and normal liver enzymes. Follow-up serology fourteen days later confirmed sustained HBsAg negativity with isolated anti-HBs positivity. The rapid resolution of HBsAg in close temporal proximity to vaccination, together with the absence of hepatitis B core antibodies and undetectable HBV DNA, supported transient post-vaccination antigenemia rather than acute HBV infection.Transient HBsAg positivity after vaccination has previously been described, particularly among hemodialysis patients. Retrospective studies indicate that circulating recombinant HBsAg may be detected shortly after immunization, most commonly within five days but occasionally up to twenty days. To our knowledge, this is the first reported case of transient HBsAg positivity in a PrEP user. This is clinically relevant given the anti-HBV activity of TDF and evidence suggesting that TDF-based PrEP reduces HBV acquisition. As incident HBV infection during PrEP use is uncommon, isolated HBsAg positivity shortly after vaccination may create diagnostic uncertainty. Awareness of this phenomenon is essential to avoid misdiagnosis, unnecessary anxiety, and inappropriate interruption of PrEP.
A 36-year-old man presented in October 2025 for PrEP initiation. He reported condomless sex with multiple male partners and occasional on-demand use of tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) obtained from a partner. Screening for sexually transmitted infections in August 2025 showed negative viral hepatitis serologies. Two days prior to the PrEP consultation, he received a combined hepatitis A/B vaccine in preparation for travel to Thailand.
Routine baseline testing revealed isolated HBsAg positivity. The patient was asymptomatic and recalled for further evaluation. Repeat testing 8 days later showed HBsAg negativity, newly positive anti-HBs antibodies, undetectable HBV DNA, negative hepatitis D serology, and normal liver enzymes. Follow-up serology 14 days later confirmed sustained HBsAg negativity with isolated anti-HBs positivity. The rapid resolution of HBsAg in close temporal proximity to vaccination, together with the absence of hepatitis B core antibodies and undetectable HBV DNA, supported transient post-vaccination antigenemia rather than acute HBV infection.
Transient HBsAg positivity after vaccination has previously been described, particularly among hemodialysis patients. Retrospective studies indicate that circulating recombinant HBsAg may be detected shortly after immunization, most commonly within 5 days but occasionally up to 20 days.
To our knowledge, this is the first reported case of transient HBsAg positivity in a PrEP user. This is clinically relevant given the anti-HBV activity of TDF and evidence suggesting that TDF-based PrEP reduces HBV acquisition. As incident HBV infection during PrEP use is uncommon, isolated HBsAg positivity shortly after vaccination may create diagnostic uncertainty. Awareness of this phenomenon is essential to avoid misdiagnosis, unnecessary anxiety, and inappropriate interruption of PrEP.
A 36-year-old man attended our clinic in October, 2025, for HIV pre-exposure prophylaxis (PrEP) initiation. He was in a steady relationship with a male partner but reported condomless sex with multiple other male partners. He had occasionally taken on-demand PrEP from his partner, although inconsistently. His medical history included recurrent genital herpes simplex virus infection, for which he was receiving suppressive acyclovir therapy. He had no known allergies, no concomitant medications, and no other chronic illnesses.
About 1 month prior, in August 2025 (day −39), he was diagnosed with lymphogranuloma venereum for which he completed a course of 21 days of doxycycline (100 mg twice daily). All other tests, including HIV, Syphilis, Hepatitis A, B, and C serologies were negative.
Two days before his scheduled PrEP visit in October (day −2), he attended our clinic because his steady partner had been diagnosed with syphilis. As their last sexual contact occurred before his recent doxycycline course, no additional preventive treatment was given. The patient also reported upcoming travel to Thailand, for which he received a combined hepatitis A and B vaccine (Twinrix®), as no prior hepatitis vaccination was documented. Laboratory testing was deferred because a PrEP visit, which includes routine laboratory testing, was scheduled 2 days later.
Timeline of laboratory tests results and vaccination.
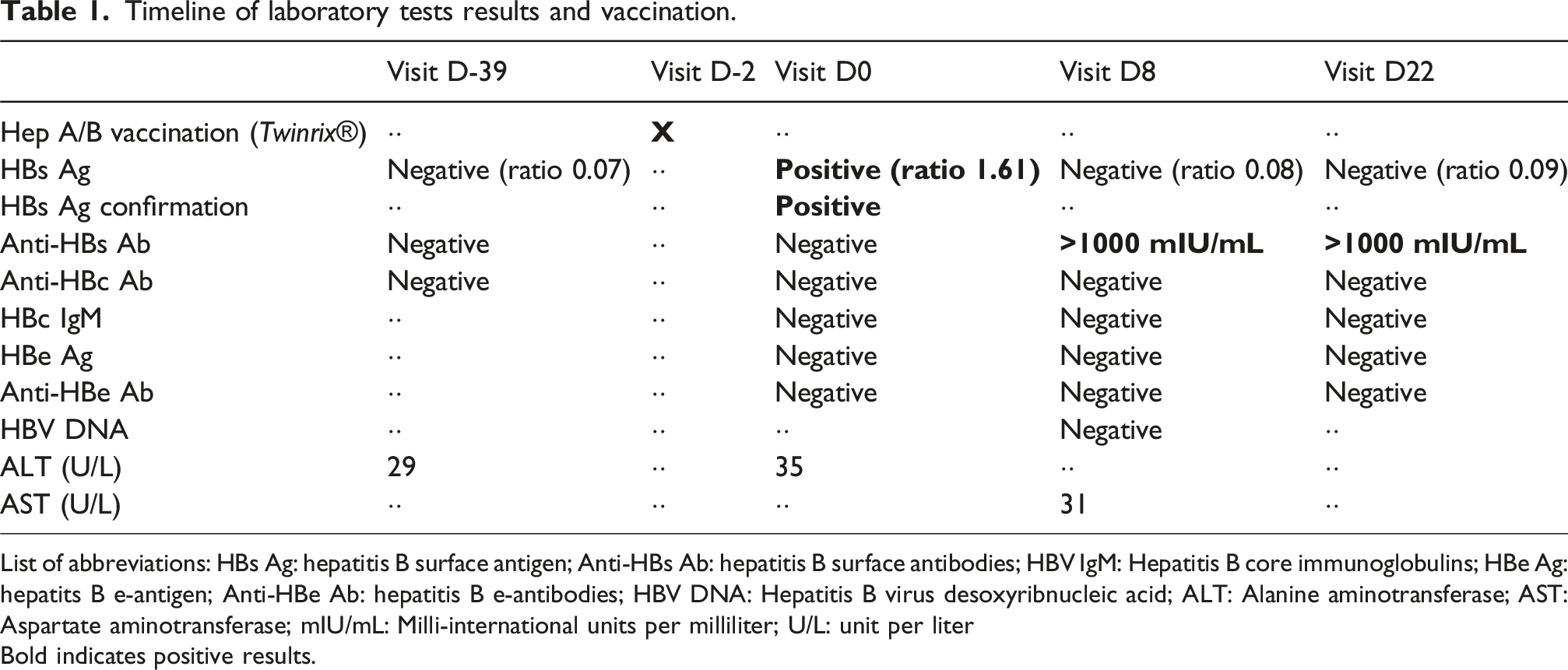
List of abbreviations: HBs Ag: hepatitis B surface antigen; Anti-HBs Ab: hepatitis B surface antibodies; HBV IgM: Hepatitis B core immunoglobulins; HBe Ag: hepatits B e-antigen; Anti-HBe Ab: hepatitis B e-antibodies; HBV DNA: Hepatitis B virus desoxyribnucleic acid; ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; mIU/mL: Milli-international units per milliliter; U/L: unit per liter
Bold indicates positive results.
Given the close temporal relationship between vaccination and testing, together with the expected evolution of HBV serological and molecular markers, transient HBsAg detection following vaccination was considered the most likely explanation. The absence of HBV DNA does not favor an acute HBV infection. The weakly positive HBsAg result and the absence of anti-HBcore antibodies suggests post-vaccination status rather than natural immunity. Transient antigenemia after vaccination has been reported, particularly among hemodialysis patients and in one traveler receiving hepatitis B immunization.1–3 A plausible explanation is that the HBsAg detected in this case was not produced endogenously by infected hepatocytes, but represented circulating recombinant HBsAg derived from the Twinrix vaccine, which contains yeast-derived (Saccharomyces cerevisiae) recombinant surface antigen. 4 As HBsAg was detected only 2 days after vaccination, this mechanism is far more likely than acute hepatitis B infection, in which HBsAg typically becomes detectable only after several weeks. 5 Current diagnostic assays detect this recombinant yeast-derived antigen just as readily as hepatocyte-derived HBsAg, and they cannot differentiate between the two.4,6 A large retrospective analysis in about 10.000 patients found transient HBsAg positivity in individuals who received HBV vaccination in the prior 14 days, without evidence of HBV infection in the follow-up, reflecting circulating recombinant surface antigen rather than true viral infection. In this study, the peak cut-off index occurred withing 2-5 days after vaccination. 1 However, one case was reported when blood sampling was performed 6 h after vaccination. Other series of cases reports found transient HBsAg positivity in hemodialysis patients who recently received hepatitis B vaccination up to 20 days prior to testing.2,3
We report, to our knowledge, the first documented case of transient HBsAg positivity following vaccination in an individual receiving HIV pre-exposure prophylaxis (PrEP) with tenofovir disoproxil fumarate/emtricitabine (TDF/FTC). This is particularly relevant given the antiviral activity of tenofovir against HBV. Observational studies have suggested that TDF-based PrEP confers protection against HBV acquisition. 7 Consequently, incident HBV infection during PrEP use is considered uncommon; however, our patient reported inconsistent adherence to the prescribed regimen. Concerns have been raised that intermittent PrEP use among individuals with chronic HBV infection could precipitate viral reactivation or flares following treatment interruption, which could lead to fatal cases of liver failure. 8 Moreover, there are concerns that HBV infection under intermittent TDF dosages could lead to TDF resistance in HBV.
This case highlights the diagnostic challenge posed by isolated HBsAg positivity detected shortly after hepatitis B vaccination, a situation that may be encountered in PrEP users, including those with intermittent use. We do not advocate the systematic avoidance of HBsAg testing in the period following vaccination, as testing may remain clinically indicated in specific settings. Rather, clinicians should be aware of the possibility of transient, vaccine-related HBsAg antigenemia and actively enquire about recent hepatitis B vaccination when unexpected isolated HBsAg positivity is identified. In such circumstances, results should be interpreted with caution and confirmed by repeat serological testing after an appropriate interval, for example at least 28 days after vaccination, before initiating further diagnostic investigations, contact tracing, or changes to clinical management. Increased awareness of this phenomenon can help prevent misdiagnosis of acute HBV infection, unnecessary testing and follow-up, patient anxiety, and inappropriate interruption of PrEP, which could otherwise increase the risk of HIV acquisition.
CPD questions
CPD question 1 – Interpretation of HBV serology
A 36-year-old man starting HIV PrEP has isolated HBsAg positivity detected 2 days after receiving a combined hepatitis A/B vaccine, with normal liver enzymes and no symptoms. Which of the following findings most strongly supports transient post-vaccination HBsAg antigenemia rather than acute HBV infection? A. Elevated ALT and AST levels B. Presence of anti-HBc IgM antibodies C. Undetectable HBV DNA with negative anti-HBc antibodies D. Persistently positive HBsAg after 3 months
Correct answer: C.
Explanation
Transient HBsAg positivity after vaccination is characterized by isolated HBsAg detection, absence of anti-HBc antibodies (total and IgM), undetectable HBV DNA, and normal liver enzymes. Acute HBV infection would typically involve detectable HBV DNA and anti-HBc IgM antibodies.
CPD question 2 – Timing and mechanism of transient HBsAg positivity
What is the most likely mechanism responsible for transient HBsAg positivity shortly after hepatitis B (or combined hepatitis A/B) vaccination? A. Early replication of wild-type HBV suppressed by tenofovir B. Cross-reactivity of anti-HBs antibodies with diagnostic assays C. Circulation of recombinant yeast-derived HBsAg from the vaccine D. Reactivation of occult HBV infection
Correct answer: C
Explanation
Hepatitis B vaccines (including Twinrix®) contain recombinant HBsAg produced in Saccharomyces cerevisiae. This circulating antigen can be detected by standard HBsAg assays, which cannot differentiate vaccine-derived antigen from infection-related antigen.
CPD question 3 – Clinical management in PrEP users
In a PrEP user with unexpected isolated HBsAg positivity detected shortly after hepatitis B vaccination, what is the most appropriate clinical approach? A. Stop PrEP immediately and initiate contact tracing B. Diagnose acute HBV infection and start antiviral therapy C. Repeat HBV serology after an appropriate interval before further action D. Perform liver biopsy to exclude occult HBV infection
Correct answer: C
Explanation
Awareness of vaccine-related transient HBsAg positivity is essential. Repeat testing after vaccination (e.g. ≥28 days) allows confirmation of HBsAg clearance and avoids unnecessary anxiety, investigations, misdiagnosis of acute HBV infection, and inappropriate interruption of PrEP.
Footnotes
Author’s contributions
TV: Writing - Original Draft; CVG: Writing - Review & Editing; DVDB: Writing - Review & Editing; UMK, BJV: Writing - Review & Editing; CK: Writing - Review & Editing. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.