
Abstract
Since the pathogen ecology differs between Caribbean regions, specific differences in the most frequent clinical presentations of acquired immunodeficiency syndrome (AIDS) may be expected. We therefore conducted the present retrospective cohort study in order to describe the main AIDS-defining events in Guadeloupe and to compare them with those observed in Metropolitan France and in French Guiana. We discuss the local pathogen ecology, the diagnostic limitations of hospitals in overseas territories and the drivers of the epidemic.
Introduction
Guadeloupe (French West Indies) is part of the French territories with the highest incidence of HIV/AIDS.1,2 The standards of healthcare in Guadeloupe are similar to those of metropolitan France. All patients infected by human immunodeficiency virus (HIV) may receive free antiretroviral treatments (including the most recent drugs) regardless of their nationality or their socio-economic status. Radiology, viral loads, CD4 counts, HIV genotyping and antiretroviral drug monitoring are available for routine care. There is a reference university hospital with laboratories specialized in parasitology-mycology, bacteriology and a Pasteur institute for the diagnosis of tuberculosis (Pasteur Institute of Guadeloupe). Although, the system is equivalent to that of France, the pathogen ecology in this Tropical Caribbean island may differ significantly from metropolitan France, as was described in French Guiana. 3 The objective of the present study was therefore to describe the 10 most frequent AIDS-defining illnesses in Guadeloupe between 1997 and 2009 and to compare their ranking and incidence with the most frequent AIDS-defining illnesses in French Guiana and in mainland France.
Patients and methods
The HIV-positive patients followed in the University hospital of Pointe-à-Pitre and Basse Terre hospital since 1 January 1988 and St Martin Hospital since 1 January 1992 until 31 December 2009 were enrolled in the Guadeloupe section of French Hospital Database for HIV (GFHDH). The French Hospital Database for HIV (FHDH) is a large prospective cohort study of HIV-infected patients who are aged >15 years and have been treated in a network of 68 French university hospitals. The enrollment criteria are documented HIV-1 or HIV-2 infection and written informed consent. Trained research assistants use French Ministry of Health DMI2 software to collect and record, on standardized forms, clinical and biological data at the time of study inclusion and at each visit or hospital admission for an HIV-related clinical event or a new treatment prescription or at least every 6 months. Diagnoses are coded according to the 10th International Classification of Diseases. 4 All patients (newly diagnosed and known HIV patients) followed between 1997 and 2009 were included.
Time-independent variables such as sex, nationality and transmission routes, and time-dependent variables such as age, weight, clinical events, therapeutic data, HIV-1 viral loads, CD4 and CD8 counts are routinely entered in the database by trained Clinical Studies Technicians. Patients included in the GFHDH have given informed consent to the use of their data. Their identity is encrypted before the data are sent to the Ministry of Health and the Institut National de la Recherche Médicale (INSERM), which centralize data from Regional Coordination of the Fight Against HIV (COREVIH) throughout France. This data collection is approved by the Commission Nationale Informatique et Libertés (CNIL), a national committee that oversees research data, in order to protect patients’ personal data. The data were analysed with STATA 10.0 (Stata Corp LP, College Station, TX, USA). We calculated the incidence rate of specific causes of AIDS in the HIV-infected individuals that were followed-up in clinical centers in Guadeloupe between 1997 and 2009, using survival times (st) functions in Stata.
In addition, general characteristics of AIDS patients in Guadeloupe, Metropolitan France and French Guiana were compared using data from the mandatory AIDS reporting system available on the Institut National de Veille Sanitaire (INVS). 5
The patient characteristics in the Guadeloupe FHDH at the time of AIDS were also studied: numbers, sex, age, CD4 count, antiretroviral treatment at the time of diagnosis and knowledge of a positive HIV test within 15 days of their AIDS diagnosis.
Results
Epidemiological characteristics of patients with AIDS in Guadeloupe, mainland France and French Guiana: 2004–2009 a .
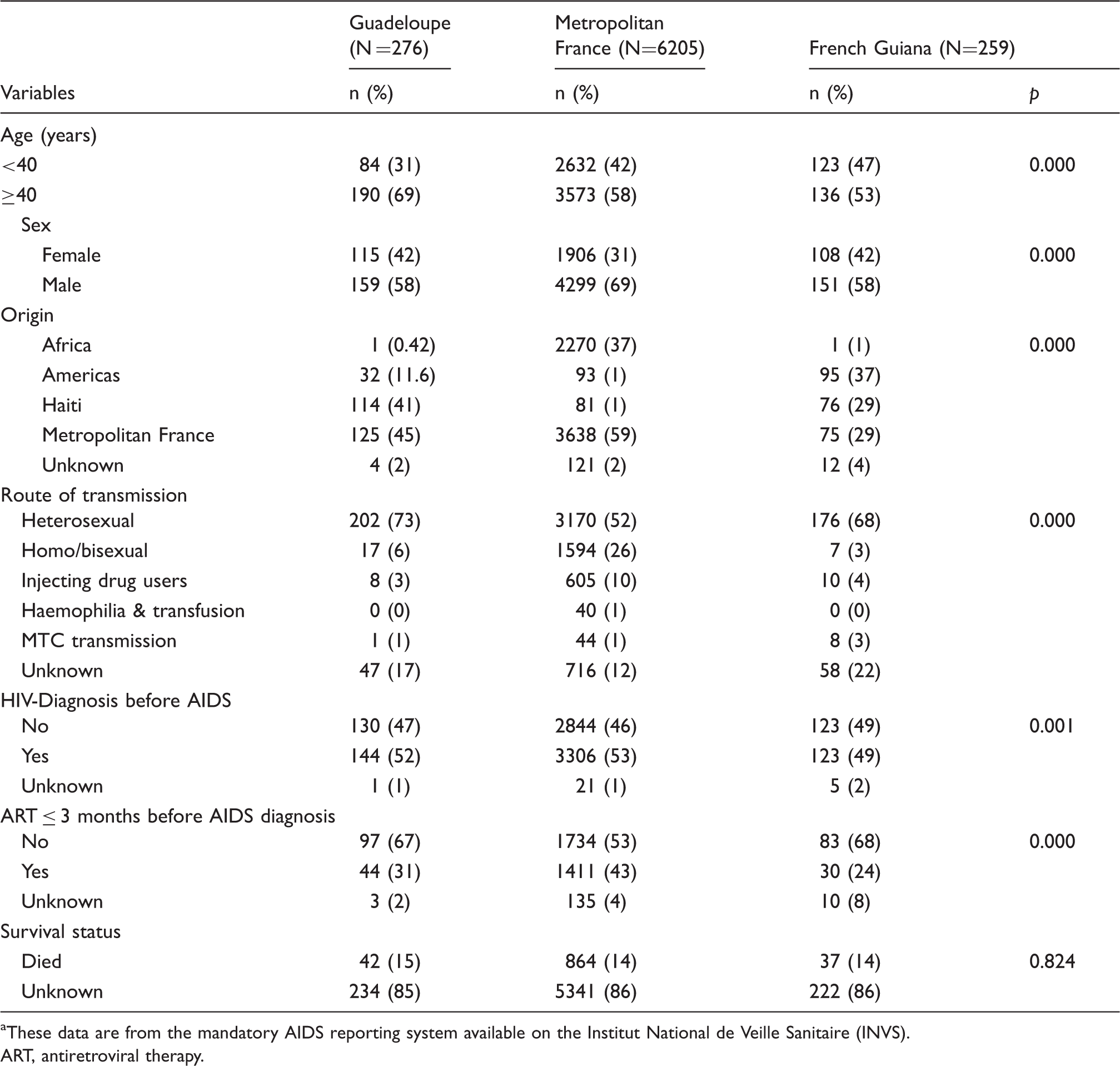
These data are from the mandatory AIDS reporting system available on the Institut National de Veille Sanitaire (INVS). ART, antiretroviral therapy.
Top 10 of opportunistic diseases in the HAART era in Guadeloupe, Metropolitan France a and French Guiana (incidence rates per 1000 person–years): 2000–2008.
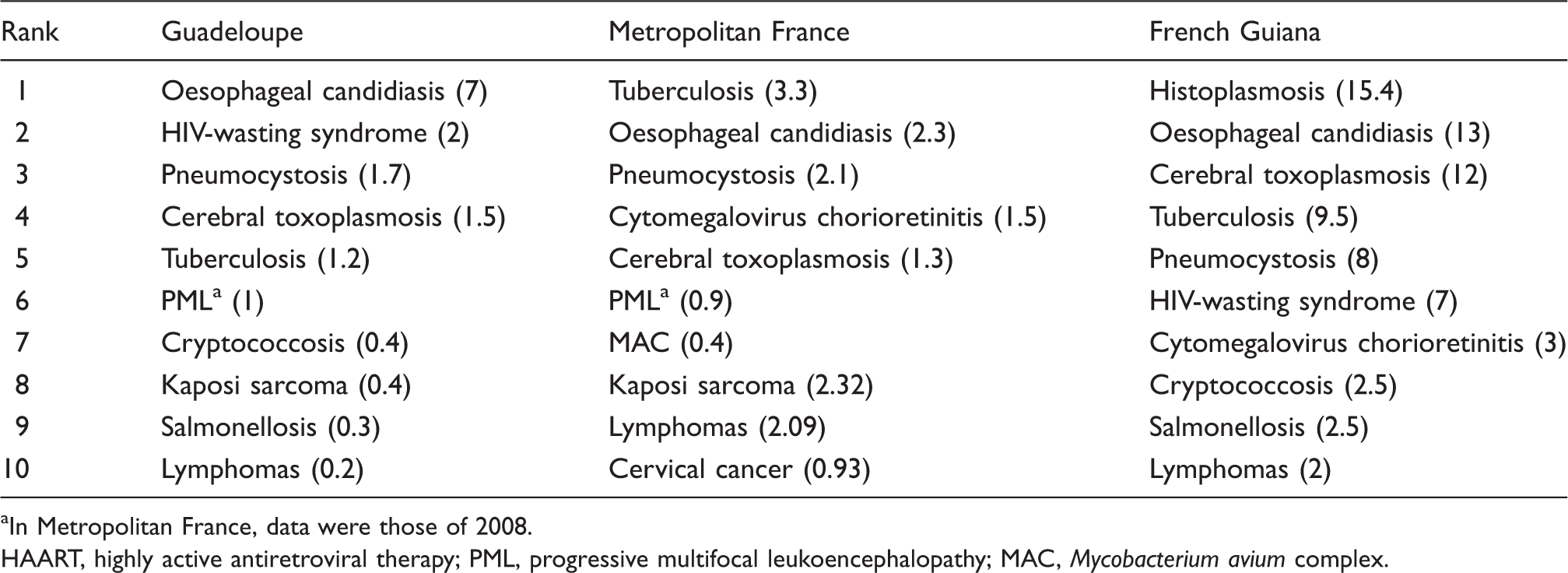
In Metropolitan France, data were those of 2008. HAART, highly active antiretroviral therapy; PML, progressive multifocal leukoencephalopathy; MAC, Mycobacterium avium complex.
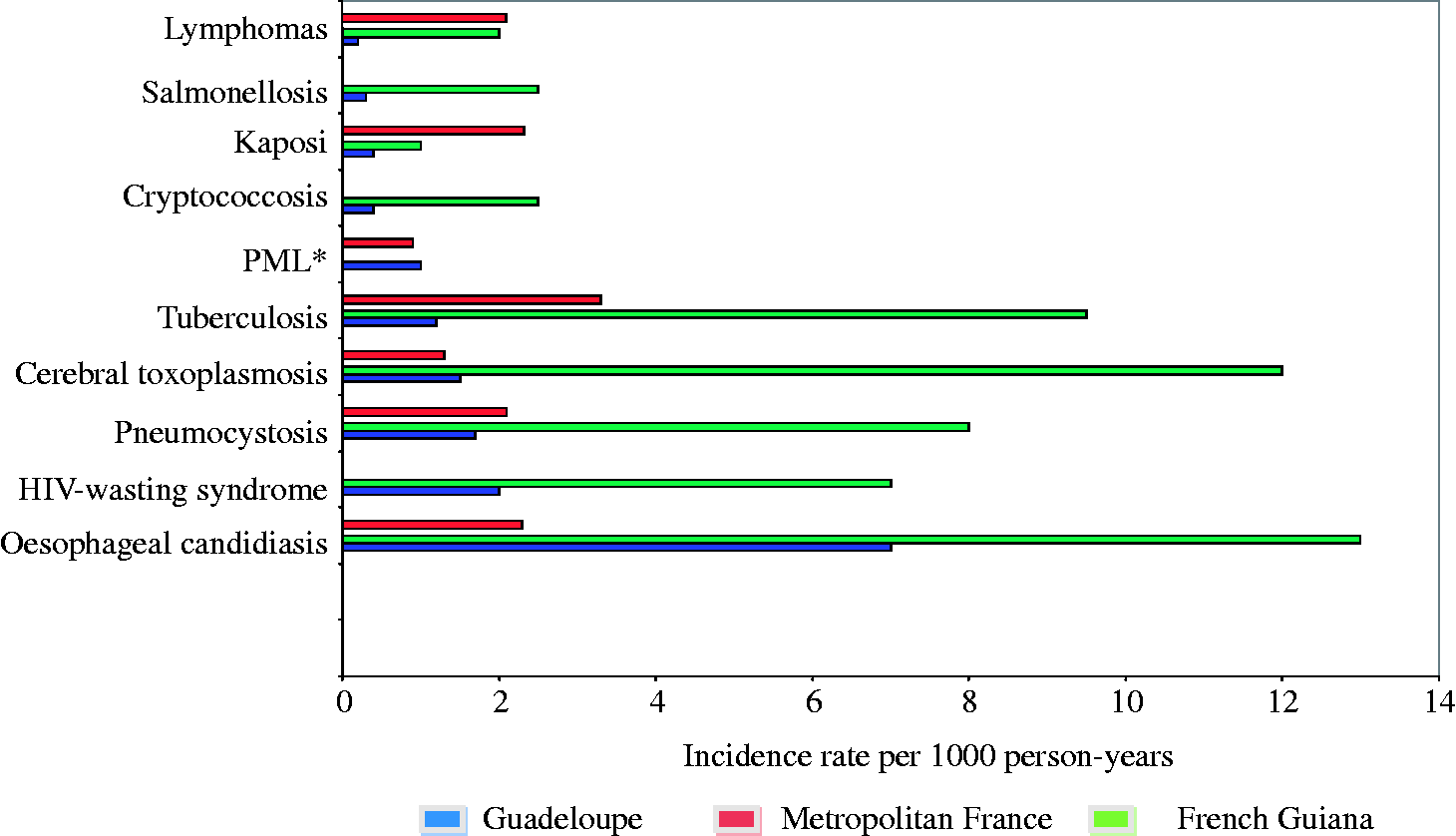
Main opportunistic diseases after the availability of HAART in Guadeloupe, Metropolitan France and French Guiana.
Characteristics of each AIDS-defining disease among HIV-infected patients: “1997−2009 hospital cohort in Guadeloupe”.

Discussion
The present results give an overview of what AIDS is in Guadeloupe, where the diagnostic facilities are that of a rich country. This description may be useful for surrounding countries with fewer resources and for the Caribbean region which would be expected to share the same pathogen ecology. The three major AIDS-related diseases in this cohort study were oesophageal candidiasis, HIV wasting syndrome and pneumocystosis. The close examination of the top AIDS-defining events in Guadeloupe, Metropolitan France6,7 and French Guiana 8 show interesting differences. Population origins differ between France, Guadeloupe and French Guiana, and frequent genetic predispositions or resistances may have hypothetically influenced some opportunistic infections. There are greater similarities in population origins between Guadeloupe and French Guiana, but the ranking differences were more complex. Guadeloupe in some aspects seemed closer to metropolitan France than French Guiana, but in other aspects the situation looked closer to that of French Guiana. First, there were differences that may have reflected differences in the drivers of the epidemic: Whereas Kaposi’s disease was at the eighth rank in Guadeloupe and metropolitan France, it was much rarer in French Guiana. This is presumably because in French Guiana transmission of the disease is mostly heterosexual, whereas in Guadeloupe and metropolitan France men who have sex with men are epidemiologically more important (see Table 1). Although there are a lot of migrations in the Caribbean, and tuberculosis is frequent in Caribbean countries, tuberculosis was the fifth cause of AIDS in Guadeloupe, the fourth in French Guiana, whereas it was the number 1 cause of AIDS in metropolitan France. The more rural setting in the overseas French territories and the importance of migrations from sub-Saharan Africa in metropolitan France may explain this difference. Beyond the ranking of incidences itself, the value of the incidence rates were instructive. Indeed, in terms of crude incidence rates, the incidence of tuberculosis in French Guiana was higher than in metropolitan France despite being ranked fourth in French Guiana. This emphasises the importance of the HIV/AIDS problem in French Guiana, the most affected French territory as reflected in Figure 1.
These French overseas territories are characterized by an important immigration from countries with high TB incidence and high HIV prevalence.9,10 French Guiana and Guadeloupe have significant immigration from Haiti where TB is prevalent; 11 however, TB incidence in the island of Guadeloupe is much lower than in continental French Guiana or even in metropolitan France. Genotyping studies 12 in the overseas French territories have calculated that recent infections are much more frequent in French Guiana (49.3%) than in Guadeloupe (27.2%) and that TB cases in foreign patients were of diverse South American sources in French Guiana whereas they mostly were from Haiti in Guadeloupe (see Table 1 and ref. 12).
It is noteworthy that cytomegalovirus (CMV) chorioretinitis was not in the top ten AIDS-defining illnesses in Guadeloupe, whereas it was for French Guiana and metropolitan France. The local epidemiology of CMV infection or local diagnostic barriers could explain this difference. Although in Guadeloupe and metropolitan France progressive multifocal leukoencephalopathy (PML) were the sixth cause of AIDS, it was absent from the top 10 in French Guiana. Because French Guiana does have the facilities to make that diagnosis, it is arguable that the epidemiology of the JC virus may be different in French Guiana, where population density is very low. This could be tested by looking at the prevalence of JC virus in French Guiana. Guadeloupe and French Guiana had non-typhi salmonelloses and cryptococcosis among the top 10 causes of AIDS. Temperature and humidity presumably facilitate the growth of these pathogens in these tropical areas. A striking feature of AIDS in Guadeloupe is that the HIV wasting syndrome was the second cause of AIDS. In French Guiana it was the sixth cause of AIDS and in metropolitan France it did not appear in the top 10. This raises the question of undiagnosed opportunistic infections in the overseas French territories, such as Mycobacterium avium complex (MAC) infectious or disseminated histoplasmosis. It is noticeable that MAC infections are not listed in the top 10 causes of AIDS, neither in Guadeloupe nor in French Guiana. In French Guiana, the arrival of a mycologist showed a marked decrease in the incidence of HIV wasting syndrome and a marked increase of histoplasmosis diagnoses that were probably overlooked before the upgrading of the diagnostic possibilities.
This finding could also reflect the presence of other pathologies or tropical pathogens. Thus, although, the health system in French overseas territories is French, its diagnostic facilities may not reach the level of larger French hospitals. Further studies, should focus on these wasting syndromes to determine why they are more frequent than in France.
One of the weaknesses of the present study was that we used crude incidence rates and not standardized rates for comparisons because this would have required to have similar stratum-specific (CD4 or Age) incidences and a reference AIDS population, which were not available to us. Possibly one of the confounding factors would be marked differences in CD4 counts at the time of diagnosis which could possibly have changed the rankings of opportunistic infections. Nevertheless, we still believe that the ranking of crude incidences is instructive in itself, notably for clinicians who should know the local most frequent causes of AIDS to guide diagnostic investigations and therapeutic strategies. Another weakness is that we compared data from 2000 to 2008 for Guadeloupe and French Guiana but only 2008 in France. The number of patients in France, being much larger than that in Guadeloupe or French Guiana, mean that this large data set should allow accurate estimations. On the contrary, in Guadeloupe and French Guiana it seemed more prudent to use a longer period in order to have more robust estimates. Nevertheless, this may have introduced some biases, notably if some of the AIDS-related illnesses could have become more frequent (i.e. increase in the incidence of tuberculosis). Finally, whereas in metropolitan France one-third of the patients were not aware of their HIV status when they developed AIDS, 5 this figure was closer to 2/3 in Guadeloupe, thus reflecting very late diagnosis in this population.
In conclusion, despite some limitations, a better knowledge of what causes AIDS in Guadeloupe is valuable for clinicians making diagnostic and therapeutic decisions and to effectively guide public health interventions. The comparative description of the main causes of AIDS raises interesting questions about the local ecology of pathogens, our diagnosis facilities and the drivers of our epidemic.
Footnotes
Acknowledgments
The authors would like to thank the members of the Guadeloupean HIV Cohort Study for data collection.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.