
Abstract
Increasing azithromycin treatment failure in sexually transmitted Mycoplasma genitalium infection, is linked to macrolide resistance and second-line treatment relies on the fluoroquinolone, moxifloxacin. We recently detected fluoroquinolone and macrolide resistance-associated mutations in 15% and 43%, respectively, of 143 initial M. genitalium PCR-positive specimens.
For a subset of 33 Western Sydney Sexual Health Centre patients, clinical information and results of sequence analysis of M. genitalium macrolide and fluoroquinolone target genes – the 23S rRNA gene, and parC and gyrA, respectively – were used to examine whether mutations were associated with treatment failure. Macrolide resistance-associated mutations correlated with microbiological (p = 0.013) and clinical (p = 0.024) treatment failure, and fluoroquinolone resistance-associated mutations with microbiological moxifloxacin treatment failure (p = 0.005). We describe the first reported cases of clinical and microbiological moxifloxacin treatment failure. Failure of first- and second-line antibiotic treatment of M. genitalium infection is occurring and likely to increase with current treatment strategies.
Keywords
Introduction
Mycoplasma genitalium is a sexually transmissible pathogen that causes non-gonococcal urethritis (NGU), cervicitis and rectal infections in men who have sex with men. 1 It has been detected in up to 25% of men with symptomatic NGU, 1 although lower rates, from 4.5% to 9%, have been reported in Australian studies.2,3 In NGU due to M. genitalium, increasing rates of treatment failure have been reported in the United States and Australia.4,5 A single dose of azithromycin (AZM) 1 g is recommended for empiric treatment of NGU before identification of the aetiological agent, but microbiological cure was achieved in only 40% of AZM-treated men with M. genitalium infection in a recent randomised NGU treatment trial. 4 An extended azithromycin 1.5 g regimen (500 mg on day 1, then 250 mg daily on days 2–5) was more effective than a single 1 g dose in one study, 6 and produced similar cure rates in another, 7 although the two regimens have not been directly compared in a randomised controlled trial. Clinical and microbiological treatment failures are associated with the presence of mutations in the 23S rRNA gene of M. genitalium, which may be selected following exposure to AZM or transmitted sexually. 5 Treatment with the fluoroquinolone antibiotic, moxifloxacin (MXF), has successfully cured M. genitalium infections following AZM treatment failure and is widely used as second-line treatment for proven M. genitalium infection or persistent NGU. 4 Mutations in the fluoroquinolone target gene parC, which are associated with fluoroquinolone resistance in other mollicutes, were present in M. genitalium clinical strains from Japanese patients following fluoroquinolone treatment 8 and strains that are resistant to both AZM and MXF, in vitro, have been described. 1 However, to date there have been no clinical reports of MXF treatment failure associated with these mutations in M. genitalium infection.
In a recent study, we detected mutations, which have been previously associated with macrolide or fluoroquinolone resistance (in M. genitalium and/or other mollicutes) in DNA extracts of 43% and 15%, respectively, of 143 initial samples from patients with M. genitalium infection, attending sexual health clinics in Sydney, Australia, from 2008 to 2011. 9 In the present study, we investigated whether these resistance-associated mutations were associated with treatment failure in a subset of these patients.
Methods
Detection of antibiotic resistance-associated mutations in M. genitalium
Laboratory methods have been described in detail previously. 9 Briefly, residual clinical specimens, in which M. genitalium DNA had been detected by an in-house PCR targeting mgpB, 10 were frozen at −20℃ and later used to determine the prevalence of macrolide and fluoroquinolone resistance-associated mutations in the 23S rRNA gene, and parC and gyrA, respectively. Target genes were amplified, sequenced, aligned against the corresponding M. genitalium G37 sequences (GenBank accession # NC_000908.2) and analysed using NCBI BLAST and UniPro UGENE 1.11 bioinformatics software (UniPro, Novosibirsk, Russia).
Case review
During the study period from 2008 to 2011, clinical guidelines for M. genitalium testing at Western Sydney Sexual Health Centre (WSSHC) were changed. From 2008 until March 2010, patients were usually tested for M. genitalium only when initial NGU treatment with AZM 1 g had failed, but from April 2010 onwards, M. genitalium PCR was performed routinely on specimens from men presenting with NGU. At this time, second-line treatment for M. genitalium-associated NGU was the extended AZM 1.5 g regimen, and MXF was recommended only for confirmed M. genitalium infection after AZM 1.5 g had failed, although some clinicians prescribed MXF prior to confirmation of M. genitalium persistence. This retrospective study included patients who had already received antibiotics for their current symptoms, so we considered that the prevalence of macrolide resistance-associated mutations in initial samples would not be representative of the true prevalence of macrolide resistance among local M. genitalium strains. Therefore, we aimed to investigate the relationship between previous antibiotic treatment and resistance-associated mutations in initial patient samples, and whether resistance-associated mutations predicted treatment failure. Clinical data were retrieved from the medical records of the subset of patients whose samples were analysed in our previous study, 9 who attended WSSHC. Data recorded included previous antibiotic treatment, gender of partner/s, history of sexual contact overseas or sex-worker contact, symptoms and signs of NGU, antibiotic treatment, any negative (as well as all positive) M. genitalium PCR tests and evidence of clinical and microbiological cure or treatment failure. Microbiological cure was defined as a negative M. genitalium PCR test following treatment. Clinical cure was defined as resolution of symptoms and signs of urethritis. We defined “treatment” as antibiotic treatment given at the same time or following initial testing for M. genitalium, and “pre-treatment” as antibiotic treatment given prior to initial testing for M. genitalium. Baseline resistance refers to resistance-associated mutation(s) detected in the initial M. genitalium test samples.
Clinical and microbiological data were analysed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp. 2012 Armonk, NY), to identify clinical factors associated with the presence of resistance-associated mutations. P values were calculated using Fisher’s exact test, except where otherwise stated.
We report, in detail, four patients in whom microbiological failure of MXF treatment for M. genitalium infection was associated with the presence of fluoroquinolone resistance-associated mutations in DNA extracts of genital or urine specimens.
This study was approved by the Human Research Ethics Committee of the Western Sydney Local Health District.
Results
During the period February 2008 to November 2011, approximately 400 patients with NGU were treated at WSSHC, 137 (34%) of whom were tested for M. genitalium infection. In all, 53 patients were diagnosed with M. genitalium infection, and clinical information and sequencing results for all three M. genitalium targets (the 23S rRNA gene, parC and gyrA) were available for 34 episodes of infection in 33 patients. They were the study group and represented 61% of patients diagnosed with M. genitalium infection at WSSHC during this time period. Of the remaining 20 (non-study group), who all attended in 2010–11, 13 were not included because their samples were missing and seven because target genes could not be amplified. A case number was allocated to each patient in the study period sequentially, according to date of presentation, from earliest to latest.
Characteristics of study patients compared with all other patients with M. genitalium infection attending Western Sydney Sexual Health Centre during the study period.
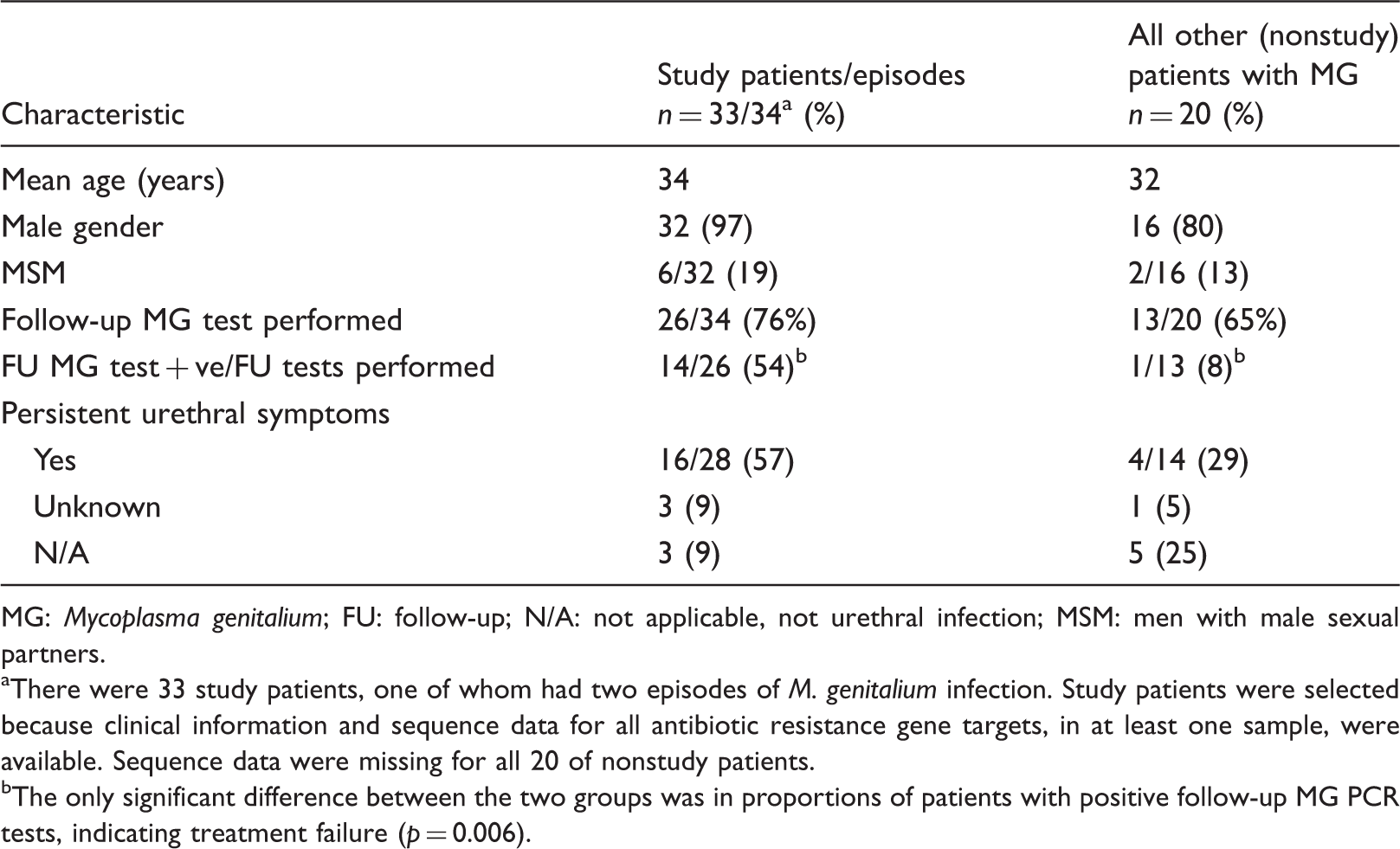
MG: Mycoplasma genitalium; FU: follow-up; N/A: not applicable, not urethral infection; MSM: men with male sexual partners.
There were 33 study patients, one of whom had two episodes of M. genitalium infection. Study patients were selected because clinical information and sequence data for all antibiotic resistance gene targets, in at least one sample, were available. Sequence data were missing for all 20 of nonstudy patients.
The only significant difference between the two groups was in proportions of patients with positive follow-up MG PCR tests, indicating treatment failure (p = 0.006).
Among study group patients, 30 were men with NGU, one of whom had two episodes; 25 of these men had only female partners, four had only male partners and one had both male and female partners. The other three patients were partners of three men with NGU: two female partners with cervical or urethral infection and one male partner with asymptomatic rectal infection.
Macrolide resistance-associated mutations in initial M. genitalium-positive samples, and the relationship with AZM pre-treatment
Initial samples from two patients were recorded as positive in M. genitalium PCR but one was missing and DNA amplification failed in the other. Macrolide resistance-associated mutations were detected in 15 (47%) initial samples from the remaining 32 patients, of whom 12 had received AZM 1 g pre-treatment for current symptoms prior to M. genitalium testing. This history was significantly associated with baseline macrolide resistance mutation (p < 0.001). These mutations were not associated with sexual contact with a sex worker or overseas (p = 0.502) or with male-to-male sexual contact (p = 0.645). Four (20%) of 20 samples from patients who had not received AZM pre-treatment contained macrolide resistance-associated mutations, representing transmitted macrolide resistance.
Initial treatment failure in relation to baseline and emergent macrolide resistance
Microbiological treatment failure following AZM 1 g was documented in 14 of 26 episodes (54%) in which one or more follow-up M. genitalium PCRs were performed. Time from treatment to follow-up test ranged from 12 to 273 days, median 46 days, IQR 29–93 days.
The presence of a baseline 23S rRNA gene mutation was strongly associated with microbiological (p = 0.013) and clinical (p = 0.024) AZM 1 g treatment failure.
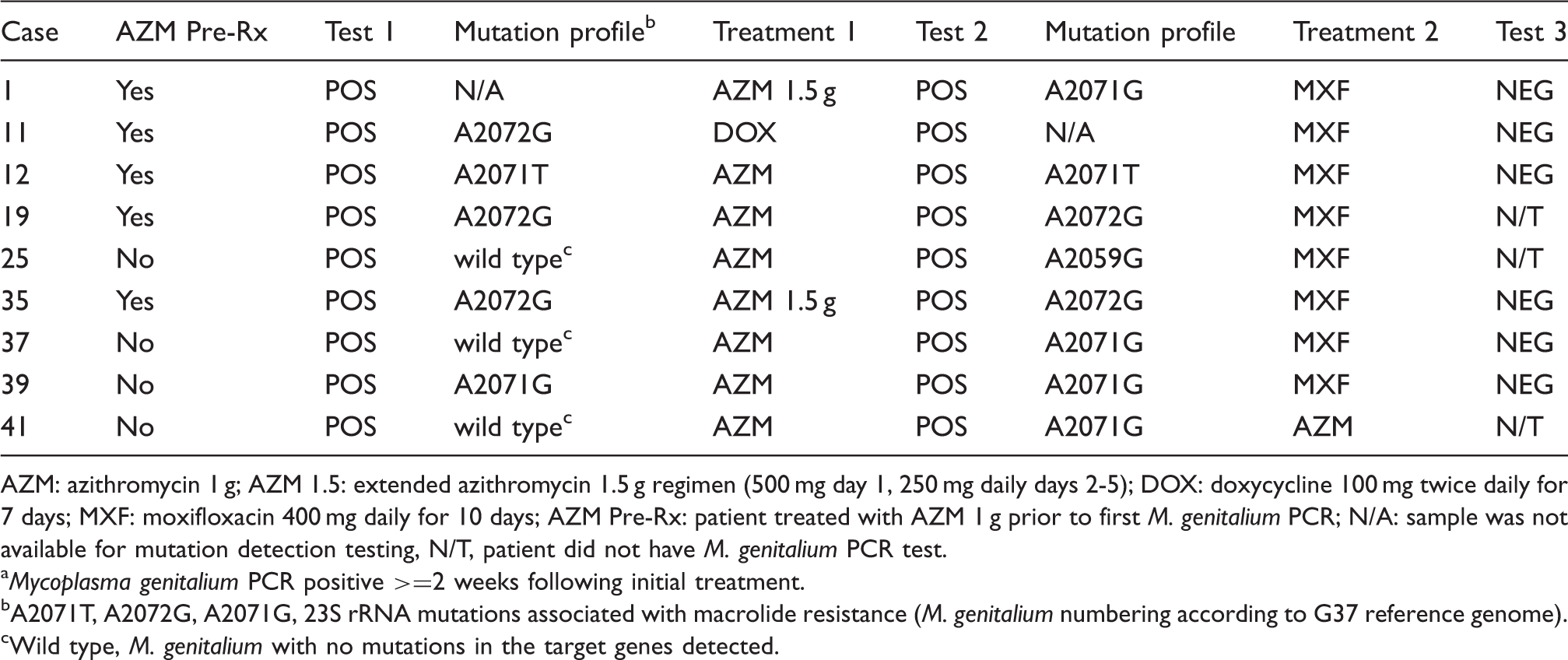
AZM: azithromycin 1 g; AZM 1.5: extended azithromycin 1.5 g regimen (500 mg day 1, 250 mg daily days 2-5); DOX: doxycycline 100 mg twice daily for 7 days; MXF: moxifloxacin 400 mg daily for 10 days; AZM Pre-Rx: patient treated with AZM 1 g prior to first M. genitalium PCR; N/A: sample was not available for mutation detection testing, N/T, patient did not have M. genitalium PCR test.
Mycoplasma genitalium PCR positive >=2 weeks following initial treatment.
A2071T, A2072G, A2071G, 23S rRNA mutations associated with macrolide resistance (M. genitalium numbering according to G37 reference genome).
Wild type, M. genitalium with no mutations in the target genes detected.
Relationship between presence of a fluoroquinolone resistance mutation and MXF treatment failure
Cases with fluoroquinolone resistance-associated mutations.
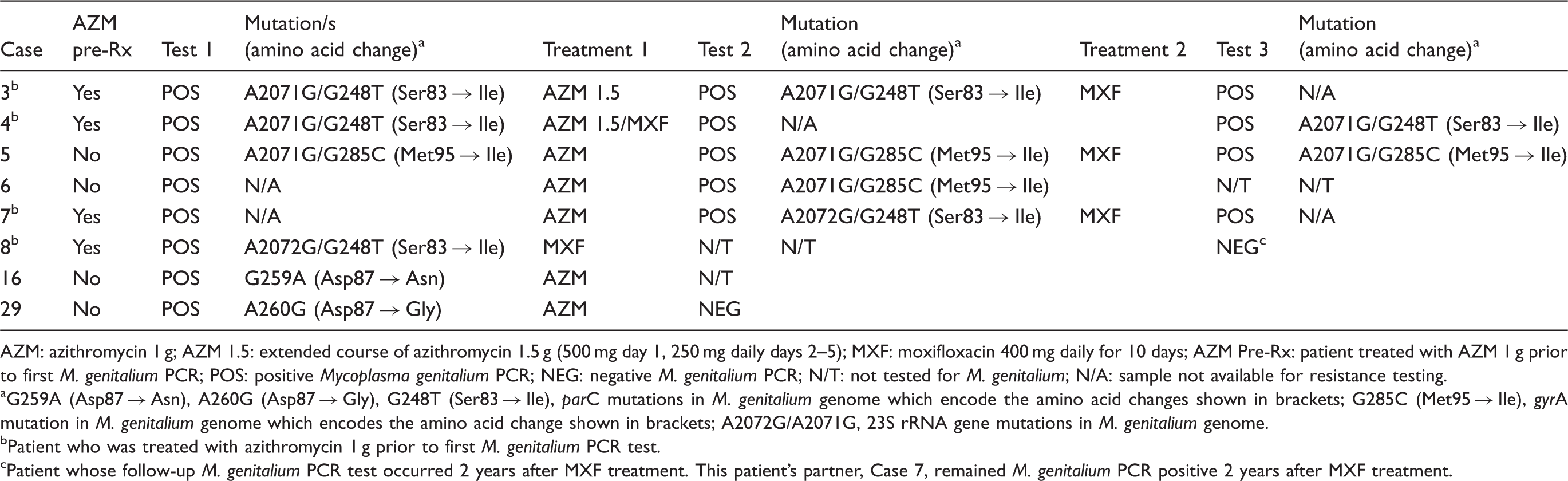
AZM: azithromycin 1 g; AZM 1.5: extended course of azithromycin 1.5 g (500 mg day 1, 250 mg daily days 2–5); MXF: moxifloxacin 400 mg daily for 10 days; AZM Pre-Rx: patient treated with AZM 1 g prior to first M. genitalium PCR; POS: positive Mycoplasma genitalium PCR; NEG: negative M. genitalium PCR; N/T: not tested for M. genitalium; N/A: sample not available for resistance testing.
G259A (Asp87 → Asn), A260G (Asp87 → Gly), G248T (Ser83 → Ile), parC mutations in M. genitalium genome which encode the amino acid changes shown in brackets; G285C (Met95 → Ile), gyrA mutation in M. genitalium genome which encodes the amino acid change shown in brackets; A2072G/A2071G, 23S rRNA gene mutations in M. genitalium genome.
Patient who was treated with azithromycin 1 g prior to first M. genitalium PCR test.
Patient whose follow-up M. genitalium PCR test occurred 2 years after MXF treatment. This patient’s partner, Case 7, remained M. genitalium PCR positive 2 years after MXF treatment.
Cases of MXF treatment failure
Mutation profiles for these patients are included in Table 3, with corresponding case numbers. All patients were reportedly adherent to treatment regimens.
Case 4
A 20-year-old man with female sexual partners was treated with AZM 1 g for urethral symptoms in 2008. One week later he presented to WSSHC, was diagnosed with NGU and M. genitalium PCR was positive. He was treated with an extended AZM 1.5 g regimen and, when this had failed, with MXF 400 mg daily for 10 days, one month after initial presentation. Although he reported no sexual activity from initial treatment until his last recorded visit, he remained symptomatic and positive for M. genitalium by PCR at three further visits. The same resistance mutations (Table 3) were detected in his initial sample and another collected four months after MXF treatment.
Case 5
In 2008, a 31-year-old man who has sex with men was diagnosed with post-gonococcal urethritis, received treatment with AZM 1 g and tested positive for M. genitalium by PCR on a first-void urine (FVU) sample. Urethral symptoms persisted and M. genitalium was detected three months later; he was treated with MXF 400 mg daily for 10 days but M. genitalium was again detected two months later. The same macrolide and fluoroquinolone resistance mutations (Table 3) were detected in all three FVU samples collected before and after treatment with AZM and MXF. His 21-year-old male partner (case 6) had asymptomatic rectal infection with the same mutation profile.
Case 7
A 45-year-old heterosexual man was treated with AZM 1 g for NGU, but one month later was re-treated with AZM 1 g and tested positive for M. genitalium. Six weeks later, when M. genitalium was again detected, he and his partner were treated with MXF 400 mg daily for 10 days. Urethral symptoms persisted and M. genitalium was detected when he returned more than two years later. The sample obtained prior to MXF treatment contained macrolide and fluoroquinolone-associated mutations, but amplification of antibiotic resistance targets, from samples collected before AZM and after MXF treatment, was unsuccessful. However, it seems likely that these mutations were responsible for persistence of NGU and M. genitalium infection. M. genitalium with the same mutation profile was detected in an FVU sample from his female partner (case 8).
Case 3
A 32 year-old man with NGU was treated with AZM 1 g in 2008. A month later, he was treated with an extended AZM 1.5 g regimen because of persistent symptoms and M. genitalium PCR on FVU was positive. He continued to have sex with his untreated female partner despite remaining symptomatic. M. genitalium PCR was still positive six weeks later and he was then given MXF 400 mg daily for 10 days. He reported no further sexual contact until M. genitalium PCR was again positive seven weeks later. He was asymptomatic at that visit, and M. genitalium PCR was negative five months later. Macrolide and fluoroquinolone resistance mutations were detected in specimens collected after the extended AZM regimen and before treatment with MXF.
Discussion
The detection of fluoroquinolone resistance-associated mutations among patients with M. genitalium NGU is of great concern, given that MXF is widely used as second-line treatment and alternative treatments have not been evaluated. These mutations appear to be circulating in the community despite the lack of local evolutionary pressure – fluoroquinolones are not recommended for treatment of any sexually transmitted infections in Sydney and are not widely used in the community for treatment of other infections.
Several cases of MXF treatment failure occurred among patients who acquired M. genitalium infection with fluoroquinolone resistance-associated mutations from 2008 to 2011. However, the association between genotypic fluoroquinolone resistance and treatment failure should be confirmed with phenotypic resistance testing, which was not done in this study. MXF was universally effective in cases due to M. genitalium strains lacking fluoroquinolone resistance-associated mutations. In patients in whom a macrolide resistance-associated mutation (either sexually acquired or induced by treatment with AZM) was also present, failure of both first- and second-line treatment occurred.
High and increasing rates of AZM 1 g treatment failure4,5 suggest that MXF will be used more commonly for treatment of M. genitalium infections. If so, both fluoroquinolone resistance-associated mutations – currently 15% 9 – and clinical treatment failures are likely to increase. Fluoroquinolone resistance-associated mutations have also been reported in other populations,1,8 but MXF treatment failure can be attributed to re-infection. In several of these cases, M. genitalium infection eventually resolved despite microbiological treatment failure. The natural history of M. genitalium infection among men with urethritis has not been well-described, apart from its association with chronic NGU. 1 Among a cohort of African female sex workers, 55% of infections cleared, without specific treatment, within three months and 93% within 12 months, while infection recurred in 39%, 11 demonstrating both spontaneous clearance and persistence of M. genitalium infections. Recurrent infections may be due to re-infection, but PCR testing can fail to detect persistent infections due to the relatively small organism load associated with M. genitalium infection. 12
In this small study, macrolide resistance-associated mutations were strongly associated with microbiological and clinical AZM treatment failure. Macrolide resistance was transmitted in 20% of patients with no history of previous antibiotic treatment, and emerged following AZM 1 g treatment in 25% of those with initial wild type M. genitalium infection. Previous AZM 1 g treatment was also significantly associated with 23S rRNA gene mutations in baseline samples; this history should be specifically sought to guide treatment decisions. The high prevalence of macrolide resistance in M. genitalium strains detected in study group patient samples is attributable to the extent of previous AZM 1 g treatment. Therefore this small study does not reflect the true prevalence of macrolide mutation-associated resistance among M. genitalium strains in the community. However, increasing rates of M. genitalium treatment failure are being reported even in studies that exclude participants with a history of recent antibiotic treatment. 4 The prevalence of fluoroquinolone resistance-associated mutations in our study patients (19%) was similar to that in all initial samples from patients in Sydney 9 and did not appear to be related to prior antibiotic treatment; therefore it is likely to represent the true prevalence among sexual health clinic patients.
Syndromic treatment of NGU requires an antibiotic that is effective against M. genitalium infection but, although AZM 1 g is becoming increasingly ineffective,4,5 current alternatives have major disadvantages. Use of doxycycline for initial NGU treatment before results of M. genitalium testing are known would prolong infection and transmission. Use of AZM 1 g along with a rapid molecular assay to detect macrolide resistance at the time of M. genitalium testing has been suggested 5 but would be beyond the resources of many services. Although it would reduce time to second-line treatment, this strategy would be ineffective for M. genitalium infections harbouring fluoroquinolone resistance-associated mutations. The extended AZM 1.5 g regimen has not been directly compared with AZM 1 g for treatment of M. genitalium and so cannot be recommended for initial NGU treatment. More information regarding the prevalence of, and risk factors for, fluoroquinolone resistance among M. genitalium strains is needed. Effective first- and second-line treatment of M. genitalium infection requires new therapies, and additional research on the natural history and sequelae of M. genitalium infection will inform clinical management.
We confirmed recent findings 5 that macrolide resistant M. genitalium strains are sexually transmitted and may emerge following AZM 1 g treatment of wild-type M. genitalium infection. The current practice of treating NGU with AZM 1 g is therefore likely to be driving increasing macrolide resistance among M. genitalium and causing increasing AZM treatment failure. In this environment, circulating fluoroquinolone resistance-associated mutations predict the increasing failure of second-line treatment with MXF.
Footnotes
Acknowledgements
Laboratory work was supported by a NSW Health capacity building infrastructure grant to the CIDM-Public Health, Westmead, Australia.