
Abstract
Balanoposthitis can be caused by a disparate range of conditions affecting the penile skin. This guideline concentrates on a selected group of conditions and offers recommendations on the diagnostic tests and treatment regimens needed for the effective management of balanoposthitis.
Keywords
Introduction
The main objective of this guideline is to aid recognition of the symptoms and signs and complications of penile skin conditions that may present to a variety of clinical specialists in Europe, including dermatology, sexual health or urology. This guideline concentrates on a selected group of conditions, which may be managed by clinicians practising in these disciplines, either alone or in conjunction with other specialists. It is not intended as a comprehensive review of the treatment of all forms of balanitis. It is aimed primarily at people aged 16 years or older.
This guideline offers recommendations on the diagnostic tests and treatment regimens needed for the effective management of balanoposthitis and includes the following penile conditions:
Candidal balanitis Anaerobic balanitis Aerobic balanitis Lichen sclerosus Lichen planus Zoon’s (plasma cell) balanitis Psoriasis and circinate balanitis Eczema (including irritant, allergic and seborrhoeic) Non-specific balanoposthitis Fixed drug eruptions
Premalignant conditions:
Erythroplasia of Queyrat Bowen’s disease Bowenoid papulosis
Aetiologies
Conditions affecting the glans and prepuce 1 .
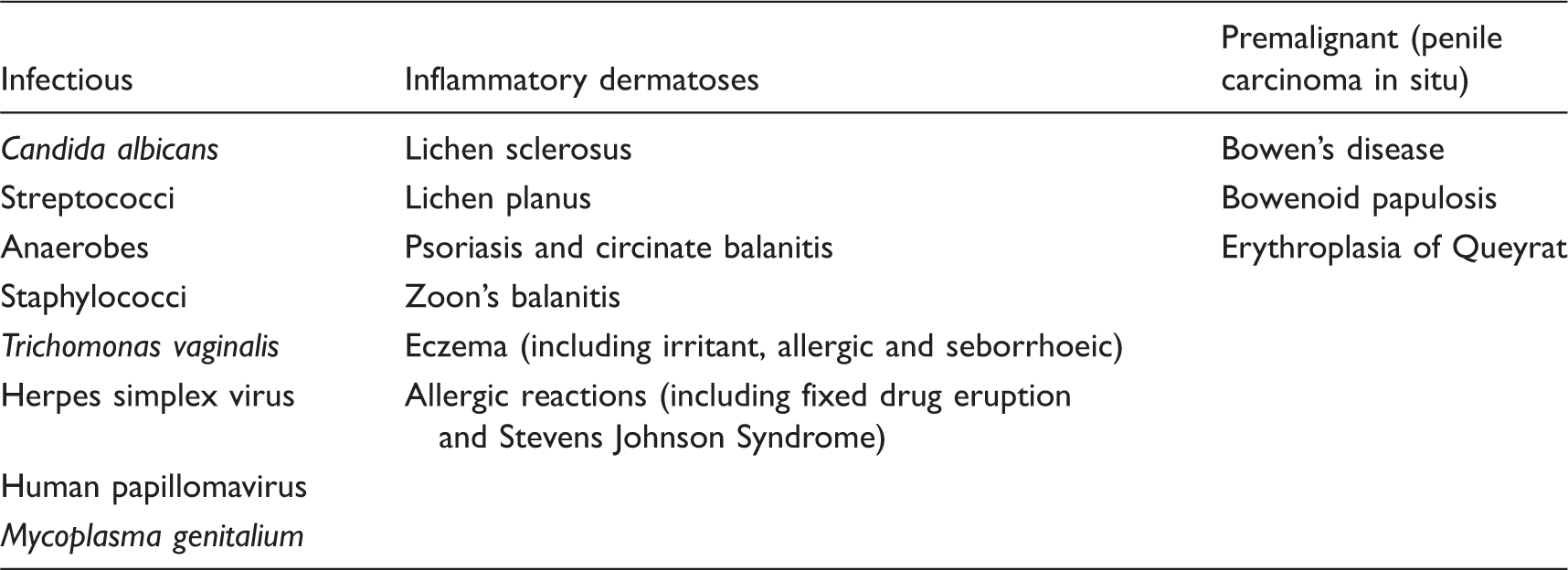
Other, rarer dermatoses are not included in this table. Infections, especially with candida, may be secondary to primary inflammatory dermatoses.
General management of the patient with balanitis 2
Clinical features
Symptoms and signs vary according to aetiology and specific conditions are covered in more detail individually. Descriptions of the typical appearances of certain balanitides are given separately in the management section.
Diagnosis
Balanitis is a descriptive term covering a variety of unrelated conditions, the appearances of which may be suggestive but should never be thought to be pathognomonic and biopsy
3
is sometimes needed to exclude pre-malignant disease. The following investigations are intended to aid diagnosis in cases of uncertainty:
Sexual history taken, with specific questioning on sexual risk taking. Sub-preputial swab for Candida spp and bacterial culture – should be undertaken in most cases to exclude an infective cause or superinfection of a skin lesion or dermatosis. Urinalysis for glucose – appropriate in some cases but especially if candidal infection is suspected. Herpes simplex virus (HSV) nucleic acid amplification test or culture for HSV – if ulceration present. Dark ground examination for spirochaetes and/or Treponema pallidum (TP) nucleic acid amplification test (where available) – if an ulcer is present, or alternatively syphilis serology with follow-up at 3 months. Culture/wet prep or nucleic acid amplification test for Trichomonas vaginalis – particularly if a female partner has an undiagnosed vaginal discharge. Full routine screening for other sexually transmitted infections (STIs) – particularly screening for Chlamydia trachomatis infection/non-specific urethritis if a circinate-type balanitis is present. Dermatology opinion for dermatoses and suspected allergy. Biopsy – if the diagnosis is uncertain and the condition persists3,4
Management
The aims of management are to minimise sexual dysfunction, to minimise urinary dysfunction, to exclude penile cancer, to treat pre-malignant disease and to diagnose and treat STIs. Predisposing factors include both poor hygiene and overwashing, over-the-counter (OTC) medications as well as non-retraction of the foreskin.
Many cases of balanitis seen in practice are a simple intertrigo; i.e. inflammation between two layers of skin with bacterial or fungal overgrowth. Rapid resolution can be achieved most frequently in practice by advising the patient to keep his foreskin retracted if possible, having advised him of the risk of paraphimosis. Saline baths are also useful, and medicated OTC talcum powders are helpful in drying the area. This advice is simple, but compliance may be challenging.
Many patients will present having tried antifungal creams, often obtained OTC. The experience is of relapse with these agents, and the simple measures have a more durable effect when compliance is lasting.
General advice
Avoid soaps while inflammation is present
5
Advise about risks of condom failure if creams are being applied Patients should be given a detailed explanation of their condition with particular emphasis on any implications for their health (and that of their partner where a sexually transmissible agent is found).
Management of specific balanitides
Infective balanitides
A range of infective agents have been isolated more frequently in men with balanoposthitis, and may not be easily differentiated by clinical findings. 6 Agents include Candida spp, Staphylococcus spp, 7 Streptococcus spp8,9 and more recently Mycoplasma genitalium. 10
Candidal balanitis (less than 20% of cases of balanoposthitis)
Clinical features
Symptoms: erythematous rash with soreness and/or itch Appearance: blotchy erythema with small papules which may be eroded, or dry dull red areas with a glazed appearance. Older age has also been identified as a risk factor.
11
Diagnosis
Sub-preputial culture (n.b. isolation of candida on culture does not prove causality, as it may represent colonisation of other underlying dermatoses) Consider urinalysis for glucose. Investigation for other causes e.g. HIV or other causes of immunosuppression if balanitis is severe or persistent. Many dermatologists believe that this primary diagnosis is very rare (apart from in diabetes mellitus [DM] and even in HIV) and that candida is almost always an opportunistic pathogen, signifying an underlying dermatosis.
Management
Recommended regimens
Apply twice daily until symptoms have settled.
Alternative regimens
Fluconazole 150 mg stat orally
12
(Ib, A) – if symptoms severe. Nystatin cream
13
100,000 units/g – if resistance suspected, or allergy to imidazoles (IIa, B). Topical imidazole with 1% hydrocortisone – if marked inflammation is present (IV, C). Although there has been an increase in reports of drug resistance in serious candidal infection, there is no new evidence pertaining to treatment of candidal balanitis.
Sexual partners
As there is a high rate of candidal infection in sexual partners, they should be offered testing for candida or empiric anti-candidal treatment to reduce the reservoir of infection in the couple.
Follow-up
Not required unless symptoms and signs are particularly severe or an underlying problem is suspected.
Anaerobic infection 14
Clinical features
Symptoms: foul smelling sub preputial inflammation and discharge, in severe cases associated with swelling and inflamed inguinal lymph nodes. Appearance: preputial oedema, superficial erosions; milder forms also occur.
Diagnosis
Gram stain may show Fusiform/mixed bacterial picture. Sub-preputial culture (to exclude other causes e.g. Trichomonas vaginalis). Gardnerella vaginalis is a facultative anaerobe which may be isolated. Swab for HSV infection if ulcerated.
Management
Advice about genital hygiene.
Recommended regimen
Metronidazole 400–500 mg twice daily × 1 week (IV, C). The optimum dosage schedule for treatment is unknown. Milder cases may respond to topical metronidazole.
Alternative regimen
Co-amoxiclav 375 mg three times daily × 1 week. Clindamycin cream applied twice daily until resolved.
These treatments have not been assessed in clinical trials (IV, C).
Aerobic infection
Clinical features
Variable inflammatory changes including uniform erythema ± oedema.
Diagnosis
Sub-preputial culture Streptococci spp and Staphylococcus aureus have both been reported as causing balanitis. Other organisms may also be involved.
Management
Treatment is usually topical. Severe cases may require systemic antibiotics.
Recommended regimens (IV, C)
Trimovate cream applied once daily Erythromycin 500 mg qds × 1 week Co-amoxiclav 375 mg three times daily × 1 week
Alternative regimens
Depends on the sensitivities of the organism isolated. Treatment is usually topical. Severe cases may require systemic antibiotics while awaiting culture results.
Sexually transmitted infections
Lichen sclerosus 4,16
Aetiology
An inflammatory scarring skin condition, possibly of autoimmune pathogenesis, but may be due to chronic occluded contact with urine in the uncircumcised. The condition occurs in all ages. It is probably responsible for many cases of phimosis in childhood. 4
Clinical features 4 , 17
Symptoms
Itching, soreness, splitting, haemorrhagic blisters, dyspareunia, problems with urination. May be asymptomatic.
Signs
Typical appearance: white patches on the glans, often with involvement of the prepuce. There may be haemorrhagic vesicles, purpura and rarely blisters and ulceration. Architectural changes include blunting of the coronal sulcus, phimosis or wasting of the prepuce, and meatal thickening and narrowing.
Complications
Phimosis Urethral stenosis Malignant transformation to squamous cell carcinoma. The risk has been quoted as a high as 10%.
4
In established penile cancer the association with lichen sclerosus is thought to be about 50% (the other 50% being associated with HPV).
18
Extra-genital disease can occur. In contrast with females perianal disease is uncommon.
Diagnosis
Typical clinical features Biopsy: This initially shows a thickened epidermis which then becomes atrophic with follicular hyperkeratosis. This overlies a band of dermal hyalinisation with loss of the elastin fibres, with an underlying perivascular lymphocytic infiltrate. Biopsy should only be carried out by experienced practitioners. A negative biopsy does not exclude lichen sclerosus, and a positive biopsy does not exclude squamous cell carcinoma or carcinoma in situ elsewhere. The choice of the area biopsied is important both in terms of the risks and in getting an adequately representative sample. Histological interpretation can be difficult and needs clinico-pathological correlation.
Management 16 , 19
Recommended regimens
Ultrapotent topical steroids16,20,21 (e.g. clobetasol proprionate) applied once daily until remission, then gradually reduced. Intermittent use (e.g. once weekly) may be required to maintain remission. A double-blind study in children showed response to topical mometasone furoate, particularly in early cases without scarring.
22
(Ia, A) In view of the immunosuppressive effects of potent steroids, patients with a history of genital warts should be warned about the risk of a relapse; consider prophylactic aciclovir in patients with a history of genital HSV infection. Secondary infection should be treated.
Alternative regimens
Although topical calcineurin inhibitors have been claimed to be efficacious20,23 (pimecrolimus applied twice daily, Ib, A), there is concern about the risk of malignancy.
24
Surgery may be indicated to address symptoms due to persistent phimosis or meatal stenosis (III, B). This may include circumcision, 25,26 meatotomy or urethroplasty. Circumcision is indicated for failed topical medical treatment.
Follow-up
Patients with a persistent requirement for topical treatment should be circumcised. Patients with atypical or persistent lesions should receive more specialist input.
27
Patients should be advised to contact the general practitioner or clinic if the appearances change (IV, C).
Lichen planus 4
Aetiology
Lichen planus is an inflammatory disorder with manifestations on the skin, genital and oral mucous membranes. More rarely it affects the conjunctiva and oesophagus. It is an inflammatory condition of unknown pathogenesis, but it is thought to have an immunological basis.
Clinical features
Symptoms: Change in appearance, more rarely itch and soreness/dyspareunia. Clinical appearance: Purplish well-demarcated plaques (can be on glans and prepuce and on the shaft of the penis); alternatively erosive lesions on the mucosal surfaces. Natural history: Mucosal lichen planus is a chronic condition with remissions and exacerbations, in contrast to cutaneous lichen planus which tends to resolve spontaneously after 12–18 months.
Diagnosis
Clinical features of purplish lesions, or supporting evidence of lichen planus lesions elsewhere on the body. This particularly includes the mouth in cases of erosive (penogingival) disease. Biopsy: irregular saw-toothed acanthosis, increased granular layer and basal cell liquefaction. Band-like dermal infiltrate (mainly lymphocytic). The condition may be associated with pre-cancerous change.
27
Management 4 , 28
Recommended regimen
Moderate to ultrapotent topical steroids depending on severity (for both mucosal and cutaneous disease) (III, B).
Alternative regimens
Topical and oral ciclosporin have been used for erosive disease29,30 (IV, C). Topical calcineurin inhibitors have also been tried in lichen planus of the vulval and oral mucosa (pimecrolimus applied twice daily, Ib A),
31
but no specific reports in penile disease (noting the caution as for lichen sclerosus) (IV, C). Circumcision: May be the treatment of choice for some cases of erosive lichen planus
32
(IV, C).
Follow-up
Patients with a persistent requirement for topical treatment should be circumcised. Atypical or persistent disease should receive more specialist input. Patients should be advised to contact the general practitioner or clinic if the appearances change (IV, C).
Zoon’s (plasma cell) balanitis 4
Aetiology
Zoon’s balanitis is a disease of older men who are uncircumcised. It is thought to be due to irritation, partially caused by urine, in the context of a ‘dysfunctional prepuce.’ It is generally regarded as a benign condition. Zoonoid inflammation clinically and histologically very frequently complicates other dermatoses, including pre-cancer and cancer.
Clinical features
Symptoms: Change in appearance. Rarely bloodstained discharge. Rarely dyspareunia. Clinical appearance: Includes well-circumscribed orange-red glazed areas on the glans and the inside of the foreskin, with multiple pinpoint redder spots – ‘cayenne pepper spots.’ These are in a symmetrical distribution.
Diagnosis
Clinical features of symmetrical, well-marginated, erythema of the glans and foreskin; however, clinical distinction from other inflammatory and pre-malignant conditions is difficult and a high index of suspicion is recommended. Biopsy: early cases show epidermal thickening but this is followed by epidermal atrophy, at times with erosions. There is epidermal oedema (often mild) and a predominantly plasma cell infiltrate in the dermis with haemosiderin deposition and extravasated red blood cells.
33
Caveat: Zoonoid inflammation complicates other dermatoses and ‘positive’ biopsy findings do not confirm the diagnosis or exclude neoplasia.
Management 4
Recommended regimens
Alternative treatments
Follow-up
Dependent on clinical course and treatment used, especially if topical steroids are being used long-term. Penile biopsy should be performed if features are atypical or do not resolve with treatment. It should be remembered that there are cases where even biopsies failed to identify pre-malignant disease.
33
Psoriasis4,39
Clinical features
Symptoms: Change in appearance, soreness or itching. Appearance: In the circumcised male psoriasis on the glans is similar to the appearance of the condition elsewhere, with red scaly plaques. In the uncircumcised scaling is lost and the patches appear red and glazed.
Diagnosis
Is supported by evidence of psoriasis elsewhere. Biopsy may be necessary, particularly in the glazed pattern of psoriasis which can look similar to pre-malignant conditions and other inflammatory conditions. The typical histological appearances include parakeratosis and acanthosis with elongation of rete ridges. There are collections of neutrophils in the epidermis. Maceration and secondary infection can modify appearances.
Management
Recommended regimen
Moderate potency topical steroids
40
(± antibiotic and antifungal) (IV, C). Emollients
Alternative regimens
Topical Vitamin D preparations (calcipotriol or calcitriol applied twice daily)
41
(IV,C). Topical bethamethasone dipropionate/calcipotriol ointment may be well tolerated in treatment of anogenital psoriasis, but potent steroids may not be indicated
40
(IV,C). Topical tacrolimus has been used in small studies
42
but should not be used as first-line therapy (IV, C). Topical pimecrolimus can also be useful.
Circinate balanitis 4
Aetiology
This characteristic presentation may occur in isolation or be seen in Reiter’s disease – a post-infective syndrome, triggered by urethritis or enteritis in genetically predisposed individuals. It consists of skin problems, joint problems and ocular problems, with other systems affected more rarely. There is overlap with psoriasis in some cases. It has been reported in association with HIV infection.
Clinical features
Signs
Typical appearance: greyish white areas on the glans which coalesce to form ‘geographical’ areas with a white margin. It may be associated with other features of Reiter’s syndrome but can occur without.
Diagnosis
On clinical appearance in association with other features of Reiter’s syndrome. Biopsy: spongiform pustules in the upper epidermis, similar to pustular psoriasis.
Management
Further investigation
Screening for STIs. Syphilis can also give rise to similar features.
15
Consider testing for HLAB27. A positive test can confirm a diagnosis and provide important information about the risk of associated disease, such as urethritis, gastrointestinal disease and arthritis.
Recommended regimen
See under ‘Psoriasis’ Treatment of any underlying infection
Sexual partners
If an STI is diagnosed, the partner(s) should be treated as per the appropriate protocol.
Follow-up
May be needed for persistent symptomatic lesions. Associated STIs should be followed up as per appropriate guidelines.
Eczema 4
Irritant/allergic balanitides
Aetiology
Symptoms can be associated with irritants, such as more frequent genital washing with soap, a history of atopy or exposure to topical agents suggesting delayed hypersensitivity. In a very small number of cases, a history of a precipitant may be obtained.
Clinical features
Appearance: ranges from mild non-specific erythema to widespread oedema of the penis.
Diagnosis
Patch tests: referral to a dermatologist is useful if allergy is suspected. Biopsy: eczematous with spongiosis and non-specific inflammation. Culture: to exclude superinfection.
Management
General advice
Recommended regimen
Hydrocortisone 1% applied once or twice daily until resolution of symptoms (IV, C).
Alternative regimen
In more florid cases more potent topical steroids may be required and may need to be combined with antifungals and/or antibiotics.
Follow-up
Not required, although recurrent problems are common and the patients need to be informed of this.
Seborrhoeic dermatitis
Aetiology
Hypersensitivity to Pityrosporum ovale.
Clinical features
Mild itch or redness (less likely to have scaling at this site).
Diagnosis
Supported by classical findings at other sites (nasolabial folds, scalp, ears, brows).
Management
Recommended regimen
Antifungal cream with a mild to moderate steroid.
Alternative regimens 4
Oral azole e.g. itraconazole (IV, C) Oral tetracycline (IV, C) Oral terbinafine may be effective
43
(Ib, A)
Non-specific balanoposthitis 4
Aetiology
Unknown
Clinical features
Chronic symptomatic presentation with relapses and remissions or persistence. No unifying diagnosis and poor response to a range of topical and oral treatments.
Diagnosis
Failure to respond to maximal topical steroid and antifungal treatments (including potent steroids). Non-specific histology on biopsy. Non-specific histology at circumcision. No evidence of underlying infective cause (e.g. Chlamydia or mycoplasma).
Management
Circumcision is curative.
Fixed drug eruption
Aetiology
An uncommon condition, but the penis is one of the more commonly affected areas of the body. Precipitants include tetracyclines, salicylates, paracetamol, phenolphthalein and some hypnotics. Rarely a fixed drug eruption can occur when the sexual partner has taken the drug and it is assumed the toxic component of the drug is passed on through vaginal fluid.
44
Clinical features
Appearance: lesions are usually well demarcated and erythematous, but can be bullous with subsequent ulceration. As the inflammation settles the skin becomes brown.
Diagnosis
History: a drug history is essential. Rechallenge: This can confirm the diagnosis but can precipitate more severe reactions and should only be done with fully informed consent of the patient. Biopsy: Hydropic degeneration of the basal layer and epidermal detachment and necrosis with pigmentary incontinence.
Management
Condition will settle without treatment Topical steroids – e.g. mild to moderate strength twice daily until resolution
45
(IV, C). Rarely systemic steroids may be required if the lesions are severe.
Follow-up
Not required after resolution. Patients should be advised to avoid the precipitant.
Pre-malignant conditions
There are three clinical presentations of penile carcinoma in situ (PCIS). 46 They are all strongly related to human papillomavirus infection 47 or lichen sclerosus. Erythroplasia of Queyrat and Bowen’s disease are considered together as they are similar but affect the non-keratinised and keratinised skin, respectively. All may progress to frank squamous cell carcinoma (SCC), but the risk is much less in Bowenoid papulosis, unless there is immunosuppression such as in HIV. SCC presents as an asymmetrical, irregular ulcer or nodule and may coexist with PCIS and lichen sclerosus.
Clinical features 48 , 49
Erythroplasia of Queyrat (PCIS of the glans)
Typical appearance: red, velvety, well-circumscribed area on the glans. May have raised white areas, but if indurated suggests frank squamous cell carcinoma.
Bowen’s disease (PCIS of keratinised skin or shaft)
Typical appearance: Scaly, discrete, erythematous plaque.
Diagnosis
Biopsy: essential – shows squamous carcinoma in situ.
Management
Recommended regimen
Surgical excision - Local excision is usually adequate and effective
49
(III, B). Mohs’ surgery can increase cure rates.
Alternative regimens
Follow-up
Obligatory because of the likelihood of recurrence (5–10%), although optimum length of follow-up is uncertain.
Bowenoid papulosis
Typical appearance: Clinically very similar to genital warts. Lesions range from discrete papules to plaques that are often grouped and pigmented.
Diagnosis
Biopsy: the diagnosis should be confirmed by biopsy.
Management 4
Recommended regimen
Alternative regimens
Follow-up
Obligatory because of the likelihood of recurrence (5–10%), although optimum length of follow-up is uncertain.
Other skin conditions
A range of other skin conditions may affect the glans penis. These include erythema multiforme and immuno-bullous disorders, including pemphigus and dermatitis artefacta. 55
A dermatologist’s opinion should be sought for diagnosis and management of these conditions.
Proposed review date
September 2018
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
List of contributing organisations
IUSTI Europe European Academy of Dermatology and Venereology (EADV) European Dermatology Forum (EDF) European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Union of European Medical Specialists (UEMS) European Centre for Disease Prevention and Control (ECDC) European Office of the World Health Organisation (WHO-Europe)