
Abstract
Chronic erythematous lesions of the penis may result from a variety of underlying causes that form a part of differential diagnosis. They are difficult to diagnose only upon clinical examination and may necessitate performing a biopsy to confirm the diagnosis and also identify the coexisting disease. We report a case of erythroplasia of Queyrat (EQ) with Zoon's balanitis and discuss the classification of the lesion through the analysis of overlapping histological features. A middle-aged uncircumcised man presented with two long-standing erythematous prepucial penile lesions unresponsive to antibiotics. Biopsy performed to establish the diagnosis revealed non-invasive severe dysplastic changes in the epithelium that is typical of EQ. Subepithelial histological features were characteristic of Zoon's balanitis. The extent and nature of inflammatory infiltrate in the dermis described in the literature is quite varied in EQ and in the spectrum of non-cicatricial balanoposthitis. The overlap of histological findings could result in the diagnostic dilemma of a coexistent lesion, as described in this case report.
Introduction
Erythroplasia of Queyrat (EQ) originally described by Tarnovsky in 1891 represents one of the precancerous conditions accepted as a distinct entity. 1 This condition is uncommon in our population. Identification of this condition is important owing to the risk of invasive cancer and to institute timely appropriate treatment.1,2 The presentation of EQ may mimic other dermatological conditions that affect the penis. One such condition that closely resembles the presentation of EQ is Zoons balanitis circumscripta plasmacellularis (BCP), which is an idiopathic benign dermatosis. Both the conditions are seen in middle age and elderly uncircumcised men.1,3,4 They appear as solitary or multiple erythematous plaques involving the glans penis and prepuce. Histopathology of the lesion is essential in making a diagnosis. However, the pathological findings although distinct for EQ, may vary in Zoon's BCP.4–7 The occurrence of EQ with coexistent Zoon's BCP is rare and there are very few cases reported in the literature. 6
We report a case of EQ with coexistent Zoon's BCP and describe the clinicopathological findings.
Case Report
A 50-year-old uncircumcised male attended a sexually transmitted infection (STI) clinic with a chronic non-healing penile ulcer of four years duration. The present condition started as a single small papule on the inner side of the prepuce. It began as a painless, non-tender lesion gradually increasing in size and later developed focal erosions. After two years, a second lesion appeared which had a warty surface and was located on the inner aspect of the prepuce a few centimeters away from the initial lesion. The patient complained of secondary dysuria upon contact with urine. There was no history of multiple partners. Complete blood count, liver function test and renal function tests were normal. Serology for syphilis was non-reactive (Venereal Disease Research Laboratory/microhae-magglutination test for Treponema pallidum). A swab study of the lesion revealed Staphylococcus epidermidis. The patient was initially diagnosed clinically as having an STI (granuloma inguinale) and was treated with antibiotics without any response.
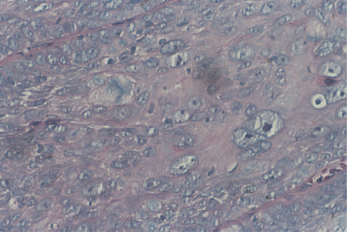
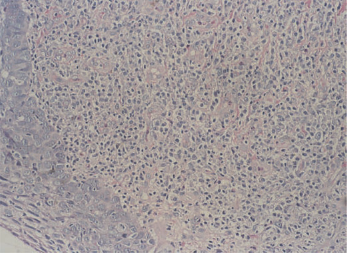
On examination, two lesions were observed on the inner aspect of the prepuce (Figure 1). One appeared as a glistening velvety erythematous plaque having ‘Cayenne Pepper spots’ and measured 2 × 2 cm. Borders, though irregular, were well demarcated and non-tender. The second lesion, located 1 cm superior to the first one, measured 1×1 cm. It is a non-tender was erythematous nodule with warty surface. Inguinal lymph nodes showed minimal enlargement. Biopsy was performed on both the lesions upon taking an informed consent. Histopathology (Figures 2-4) revealed acanthosis, elongated and widened rete ridges and full thickness epithelial atypia. Some of the epithelial cells show marked pleomorphism and vacuolation of the cytoplasm and mitoses. The epithelium showed focal erosions and exocytosis and a few extravasated erythrocytes. The upper dermis showed dense band-like lympho-histiocytic infiltrates mixed with plasma cells, dilated capillaries, a few extravasated red cells and haemosiderin deposits. There was no evidence of tumour invasion. A diagnosis of EQ with Zoon's balanitis was made.
Penile lesions on the inner aspect of the prepuce. Larger one is an erythematous glistening plaque and the smaller one is an erythematous fleshy lesion with a warty surface Marked dysplastic changes in the epithelium (× 40) Dysplastic epithelium with focal erosions and dense subepithelial inflammatory infiltrates (× 4) Lympho-histiocytic infiltrates with many plasma cells. Overlying epithelium shows dysplasia and mitosis (×10)

Discussion
Genital dermatological lesions may be due to STI or non-STI-related causes. Most often in clinical practice genital lesions are considered to be of STI origin and are treated following a confirmed or presumptive diagnosis by performing routine clinical examination and laboratory tests. The differential diagnosis for EQ includes Zoon's balanitis, lichen planus, fixed drug eruption and psoriasis. Biopsy is an essential investigation in establishing a diagnosis.1,3
Zoon's balanitis clinically closely resembles EQ. Both of them occur in middle aged or elderly patients. Histological features are distinctive but few variations are described in the literature.4,8 Alessi et al. describe the presence of a thick band of lympho-histiocytic infiltrates with plasma cells, vascular prominence, extravasation of red blood cells and haemosiderin deposits in the upper dermis that are typical of Zoon's balanitis are also noted in our patient. Epidermal changes of Zoon's balanitis show an early slight thickening of the epidermis, parakeratosis and in more advanced cases atrophy of the epidermis, superficial erosions, a scattering of neutrophils in the upper reaches of the epidermis, scant spongiosis. The epidermal changes in our case were quite distinctive of EQ with focal erosions and exocytosis. EQ is a premalignant condition having 10-33% risk of becoming an invasive malignancy.1,2 Therefore, accurate identification has prognostic implications.
Zoon's BCP is a nonspecific inflammatory condition possibly due to disturbed preputial ecology or mild trauma and irritation. 9 The description of its histopathological features in literature vary considerably. The overlap of histological findings in cases of balanoposthitis can cause confusion in making a diagnosis. Alessi et al. 7 have proposed reclassifying the spectrum of changes as inflammatory non-cicatricial balanoposthitis. Further, Zoon's balanitis may be found in isolation or superimposed on lesions of other diseases and may modify the histological picture to a varying extent. Histological features of EQ described in the literature also mention the inflammatory component in the dermis, hence establishing that a coexistent lesion is complex. However, in our case the extent of inflammatory infiltration and other findings in the upper dermis were strongly in favour of Zoon's balanitis. Hence, diagnosis of a coexistent EQ with Zoon's balanitis was made, considering the clinical presentation and analysis of overlapping histopathological findings.