
Abstract
Despite recent declines in HIV incidence, sub-Saharan Africa remains the most heavily affected region in the global HIV/AIDS epidemic. Estimates of HIV prevalence in African military personnel are scarce and inconsistent. We conducted a serosurvey between June and September 2007 among 4043 Armed Forces personnel of the Democratic Republic of Congo (FARDC) stationed in Kinshasa, Democratic Republic of Congo (DRC) to determine the prevalence of HIV and syphilis infections and describe associated risk behaviours. Participants provided blood for HIV and syphilis testing and responded to a demographic and risk factor questionnaire. The prevalence of HIV was 3.8% and the prevalence of syphilis was 11.9%. Women were more likely than men to be HIV positive, (7.5% vs. 3.6% respectively, aOR: 1.66, 95% C.I: 1.21–2.28, p < 0.05). Factors significantly associated with HIV infection included gender and self-reported genital ulcers in the 12 months before date of enrollment. The prevalence of HIV in the military appears to be higher than the general population in DRC (3.8% vs. 1.3%, respectively), with women at increased risk of infection.
Keywords
Introduction
Despite recent declines in HIV incidence, sub-Saharan Africa remains the most heavily affected region in the global HIV/AIDS epidemic. It is estimated that sub-Saharan Africa currently accounts for nearly 70% of the world’s HIV infections with a prevalence of more than 22.5 million. 1
In addition to high-risk sexual behaviours, the disproportionate burden of HIV experienced by this region has been attributed to a number of economic, social, and political factors including poverty, civil unrest, and increased mobility.2,3 Moreover, certain occupations involving frequent migration such as migrant labour, mining, truck driving, and military involvement are associated with an increased risk of contracting HIV and other sexually transmitted infections (STIs). 4 Migratory lifestyles characterised by long periods of familial separation provide an opportunity to engage in casual sex with multiple partners and commercial sex workers. 2
Recent studies have shown that the HIV prevalence of adults aged 15–49 in the Democratic Republic of Congo (DRC) is lower than the overall sub-Saharan African estimate (1.3% vs. 5.2%). 5 However, HIV prevalence among DRC’s most-at risk-populations (MARPs) are significantly higher, which includes sex workers (14.7% in Kinshasa and 23.3% in Lubumbashi) and conflict-afflicted populations (3.1% to 6.7%).1,6–8 Reports documenting the high rates of non-partner sexual violence in mathematical modeling scenarios show the potential for an increase in annual HIV incidence by 7%, impacting up to 10,000 women and girls in the DRC under extreme conditions. 9 Past publications have suggested (non-empirically) that the HIV prevalence in the Congolese military could be as high as 60%.10–14 Additionally, reports based on predictions may have overestimated the prevalence of HIV in the Congolese military.10–12,14 These estimates were generated in 1999, while the DRC was actively engaged in a multi-country civil war. In addition, the confidentiality of information regarding the size and structure of the FADRC may contribute to inaccurate estimates of disease prevalence within the military.
Estimates of HIV prevalence in African military personnel are limited and inconsistent. Some research has suggested that HIV rates are higher in military populations, while other studies indicate that rates are, instead, comparable to the general population.15,16 The sexual behaviours of soldiers have significant implications for the spread of HIV and other STIs, who appear to be at an increased risk of infection.17,18 Military personnel tend to be young men, spending considerable amounts of time away from home, and have access to a large number of sexual partners, including commercial sex workers and internally displaced women.15,19–21
In a 2008 study of military personnel in Ethiopia, participants self-reported their military background, work-associated travel, sexual history and risk behaviours. Higher military rank, higher numbers of sex partners, and month-long travel in the past year were factors associated with an elevated risk of HIV infection and other STIs compared to those in the general population. 2 In a recent survey of Nigerian naval personnel, about 20% of men had sexual contact with a commercial sex worker in the past six months and 40% had not used a condom. 22 Studies have also suggested that military personnel are often paid more consistently than other government employees, leading to increased financial stability and the ability to purchase sex, placing them at higher risk of HIV infection.22–24
Preliminary HIV genetic analysis using specimens collected from DRC military personnel suggest high HIV heterogeneity, yet a fairly low prevalence of infection. 25 Although these results are similar to previous studies in the general population,26–28 scant data are available on the risk factors and prevalence of STIs, including HIV and reasons behind the high genetic diversity of the disease, in the Armed Forces personnel of the Democratic Republic of Congo (FARDC). Further analysis was conducted to estimate the HIV prevalence in the FARDC and evaluate risk factors associated with HIV and other STIs.
Methods
Population selection
From June to September 2007, a single-stage 30-cluster sample survey was conducted among active FARDC personnel stationed in Kinshasa. The military population is currently estimated to be 155,000 persons, 2.7% (4185) of which are women, who participate in both administrative roles and in field operations. 29 A complete list of companies based in Kinshasa obtained from the Ministry of National Defense was used to randomly select individual companies to serve as study sites. In each selected unit (company), every active duty man and woman (officers and enlisted) was offered enrollment in the study, and informed consent was required for participation. The study protocol was approved by Human Subjects Protection Organisations at both the Kinshasa School of Public Health and United States Army Medical Research and Material Command.
Questionnaire, specimen collection and testing
All participants were provided with HIV testing and counseling, and a detailed explanation of the purpose, confidentiality and procedures of the study. Trained interviewers administered a 60-min questionnaire that included socio-demographic characteristics, duration and location of military service, sexual behaviours and self-reported STI symptoms within the past 12 months. Participants were asked to return for their HIV and syphilis test results one week later.
Blood samples were processed and separated into buffy coat and plasma on the same day and kept at −20°C at the DRC National AIDS Program Laboratory in Kinshasa. Buffy coat samples conserved at −80°C were used for HIV genetic testing. 26 Plasma was tested for HIV antibody following the DRC national testing algorithm; a rapid test (Determine HIV-1/2 from Abbott, IL, USA) followed by an ELISA test (Enzygnost HIV1/2 integral from Dade Behring, Dresden, Germany). Specimens were classified as HIV positive if reactive on both tests. Discordant or indeterminate samples were retested by two ELISA tests, Enzygnost HIV 1/2 and Vironostika (bioMerieux SA, Marcy, l’Etoile, France), and classified as positive if reactive for both of the ELISA tests. Individuals testing positive for HIV and returning for results were referred to the military health centre. Samples were tested for syphilis using the Determine Syphilis rapid test, 30 and results were available to participants within 48 h. Individuals testing positive for syphilis infection were treated on site with a single shot of benzathine penicillin G, and referred to a health centre for follow-up.
Statistical analysis and variable selection
Data analysis for this paper was conducted using SAS software, version 9.2. 31 Participants with missing HIV status or basic data from the questionnaire were excluded from the analysis. Frequency distributions of socio-demographic and behavioural characteristics were calculated for men and women separately. Due to the low number of women participants, data on HIV prevalence for socio-demographic and risk factor subgroups could not be stratified by gender. For variable categorisation, categories found in the 2007 Demographic and Health Survey (DHS) analysis were used when possible – including age group, number of sexual partners and birth region; mobility was defined as number of posts outside Kinshasa during the preceding five years, and questions which were believed to be ambiguous in the original wording of the question were not included for further analysis. Associations between selected variables and HIV infection were first explored with complete case analysis using logistic regression. Best subset selection was used for model selection, after testing a number of other model selection methods, and the multiple imputation method was used to account for missing data (all assumptions were met, and individuals missing data were not significantly different from those not missing data). The final model was analysed using 20 imputations. The final model selected includes variables adjusted for age, gender, time in the garrison, mobility, numbers of sex partners, genital ulcer and active syphilis infection.
Results
Socio-demographic characteristics
Socio-demographic characteristics of survey participants (n = 3919).
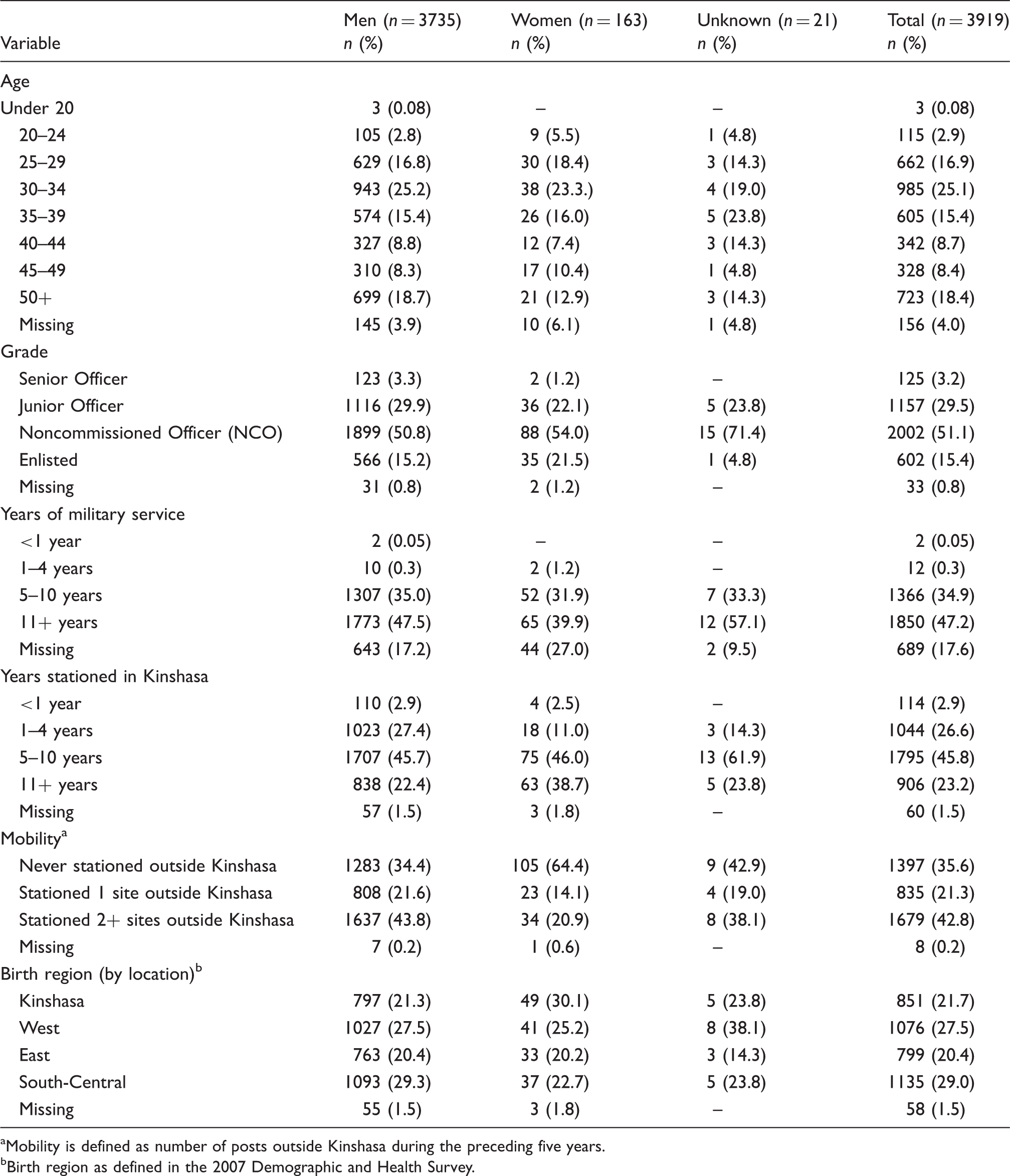
Mobility is defined as number of posts outside Kinshasa during the preceding five years.
Birth region as defined in the 2007 Demographic and Health Survey.
Sexual activity and risky behaviour among military personnel stationed in Kinshasa (n = 3919).
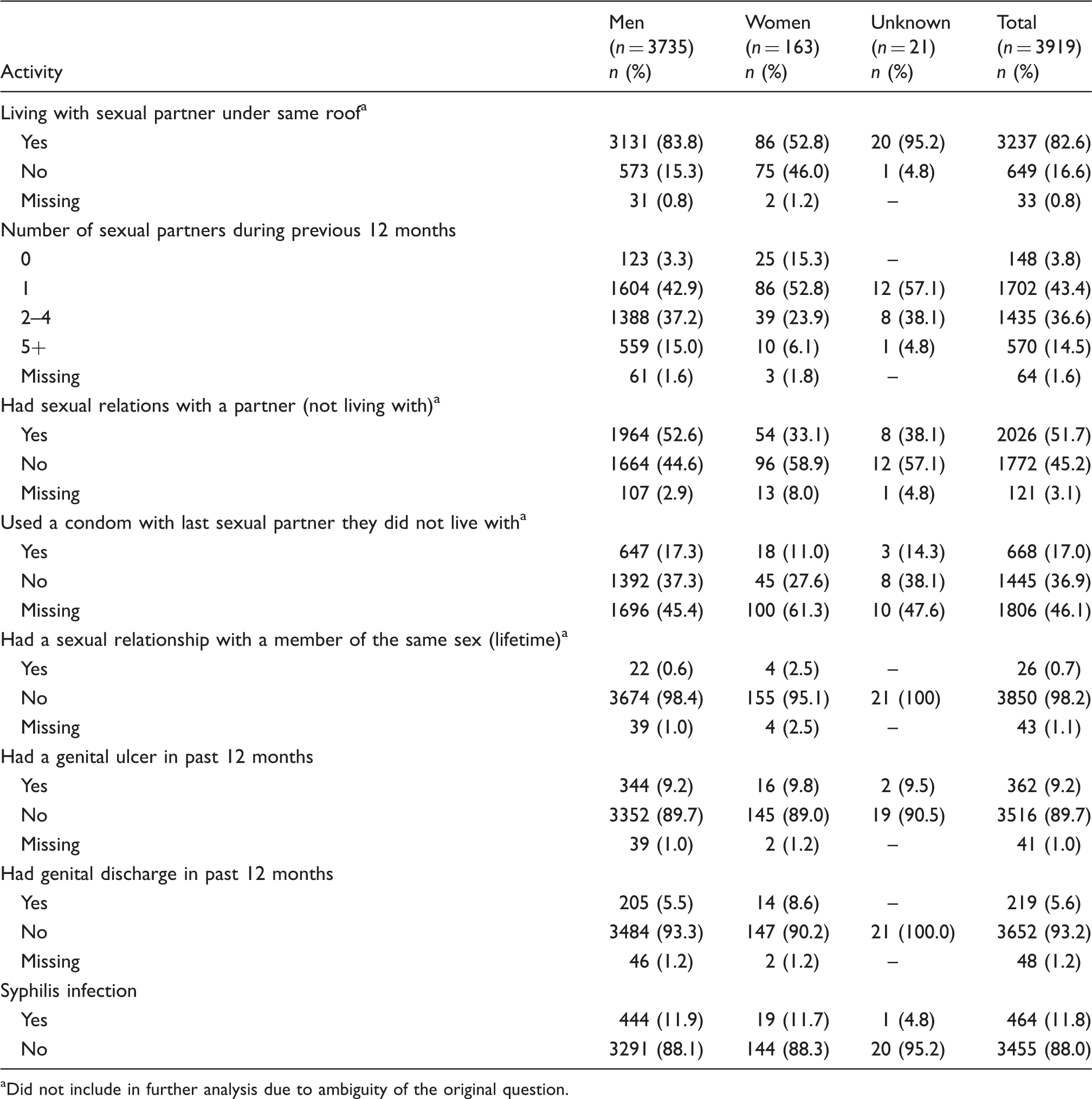
Did not include in further analysis due to ambiguity of the original question.
Prevalence of HIV and syphilis
Demographic risk factors for HIV infection.
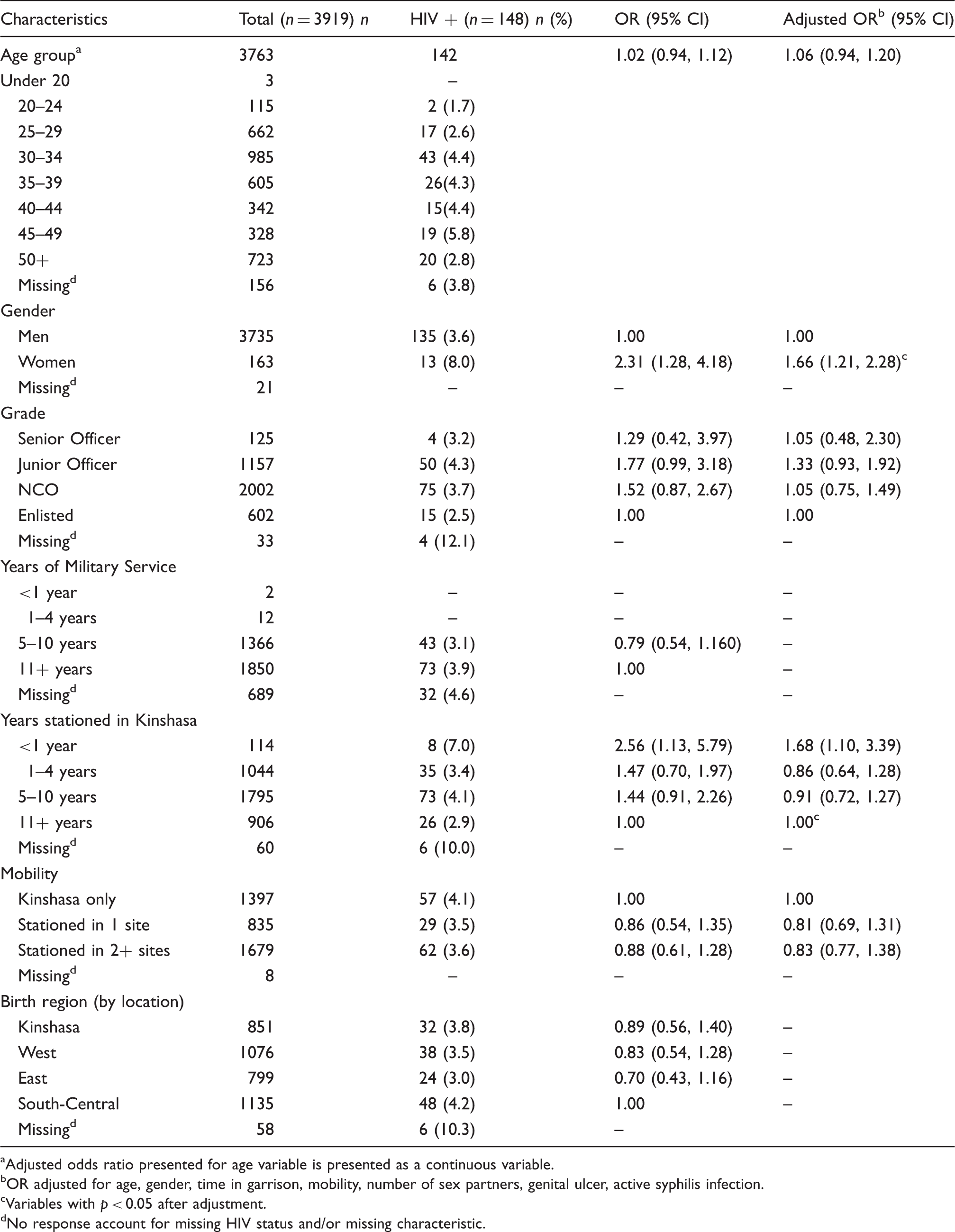
Adjusted odds ratio presented for age variable is presented as a continuous variable.
OR adjusted for age, gender, time in garrison, mobility, number of sex partners, genital ulcer, active syphilis infection.
Variables with p < 0.05 after adjustment.
No response account for missing HIV status and/or missing characteristic.
Risk factors for HIV infection
Sexual risk factors for HIV infection.
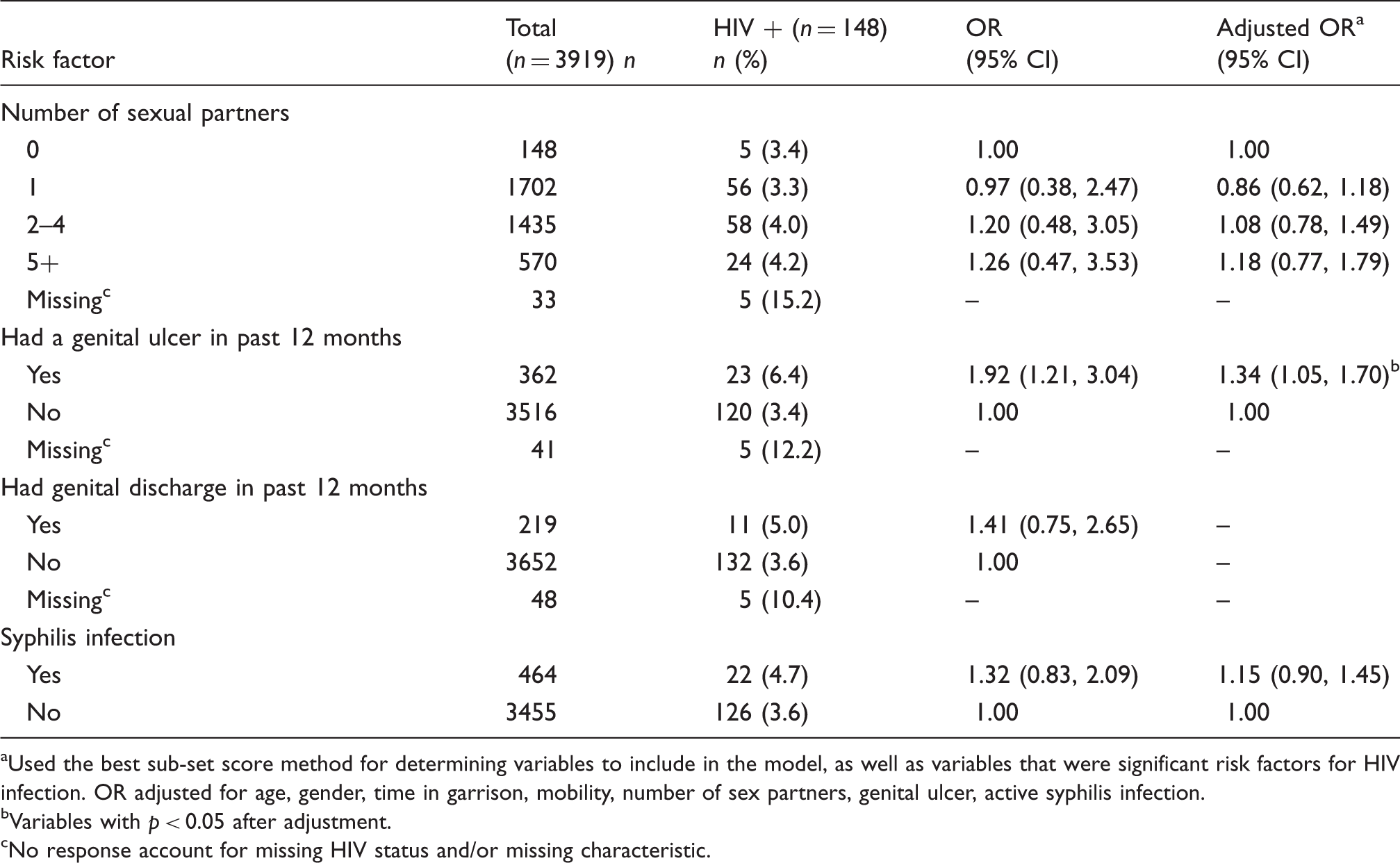
Used the best sub-set score method for determining variables to include in the model, as well as variables that were significant risk factors for HIV infection. OR adjusted for age, gender, time in garrison, mobility, number of sex partners, genital ulcer, active syphilis infection.
Variables with p < 0.05 after adjustment.
No response account for missing HIV status and/or missing characteristic.
When looking at age, participants aged 45–49 had the highest percentage of those testing positive for HIV compared to other age groups (Table 3). Additionally, those stationed for less than one year in the Kinshasa garrison were at highest risk of testing positive for HIV compared to those assigned for longer time periods (Table 3). However, these soldiers were not necessarily new recruits; based on the available data for those in this category (n = 88, data not presented), all had been in the military for at least five years.
While the HIV prevalence increased with the number of sexual partners reported in the past 12 months (no partners: 3.4% vs. 5+ partners: 4.2%), there were no significant differences in the adjusted odds ratios (aOR = 1.18, 95% C.I. 0.77, 1.79) for HIV infection (Table 4). After adjusting for other variables, there was a significant association between those reporting a genital ulcer in the past 12 months and HIV infection. FARDC reporting a genital ulcer had 1.34 times the odds (95% C.I. 1.05, 1.70) of HIV infection when compared to those who did not report a genital ulcer (Table 4). However, the association between syphilis and HIV infection was not significant; those testing positive for syphilis had 1.15 times the odds (95% C.I. 0.90, 1.45) of HIV infection compared to those testing negative for syphilis (Table 4).
Discussion
This is the first cross-sectional study to quantify the seroprevalence of HIV (3.8%) in the FARDC. The estimated prevalence in this military population is slightly higher than that reported in the general population (1.3%). 5 The sex-specific prevalence of HIV among women was twice that of men (8.0% vs. 3.6% respectively), which is consistent with previous reports. 26 Overall, the age trend seen in military personnel was similar to that seen in the general population; however, based on a limited amount of HIV-positive persons, those under 24 were found to have an elevated prevalence compared to general population estimates (1.7% vs. 0.5%, respectively). 5
Personnel reporting five or more partners in the past year appeared to have a slightly elevated (but non-significant) risk of testing positive for HIV compared to those reporting no partners in the past year. In the 2007 Demographic and Household Survey (DHS) survey, participant groups reporting no partners during the 12 months had the highest percentage of HIV-positive individuals compared to those reporting two or more partners (1.9% vs. 1.1% respectively). 5 Similarly, DHS results showed little difference between HIV prevalence in individuals reporting no high-risk sexual partners and those reporting two or more high-risk sexual partners (1.5% vs. 1.7%). 5 However, previous research has shown that risk of HIV increases as the number of sexual partners increases, especially in cases where the partners are considered a high-risk group. 2 Military personnel may seek the services of sex workers, and in Kinshasa, sex workers have the highest prevalence of HIV in DRC.7,8,22,32 There are several hypotheses that may explain this inconsistency. The number of sexual partners may have been under-reported. If the reporting is accurate, then the true prevalence in the population may indeed be low and is not affected by the number of partners or partner type. It is also possible that the sample size was inadequate to detect a significant difference given the low prevalence of HIV in the population.
The current study estimates the prevalence of syphilis at 11.8% in this military population. There was no significant difference in general between men (11.9%) and women (11.7%), and between other demographic or behavioural correlates in this analysis. Recent estimates of syphilis in child soldiers (aged <18) in the eastern Congo showed a prevalence of 3.4%, with an even distribution in men and women. 33 Additionally, estimates ranged between 0.4% and 4.0% in a recent report on river dwelling persons and internally displaced women in the eastern part of DRC. 34 However, a 2004 study of 525 women in antenatal clinics in Kinshasa (the same location as the current study) identified no active syphilis infections, and a more recent study in 2011 of women in antenatal clinics (n = 1840) found a screening prevalence of 2.0%, suggesting that the prevalence of syphilis in women residing in Kinshasa may be very low.35,36
Self-reported data on two common STI symptoms (genital ulcers and genital discharge in the past 12 months) were collected during the interview. Self-reported genital discharge was not significantly associated with HIV infection in the analysis; however, aOR for reporting a genital ulcer in the past 12 months was significantly associated with HIV infection. Genital ulcerations as a result of STIs, including syphilis, chancroid and genital herpes, have been associated with an increased risk in acquiring HIV. 37 Our estimated 3.8% prevalence suggests that STI symptoms may be a better predictor of HIV infection than the number of reported sexual partners.
This was a cross-sectional study; therefore the length of time with HIV infection could not be ascertained for any seropositive participant. Thus it is unclear whether infection occurred before or after enlistment. However, as of 2007, new recruits entering the FARDC are expected to be screened for HIV at the time of their enlistment, and are excluded from service if seropositive. 38 Longitudinal studies with consistent follow-up are necessary to explore the changing HIV epidemic in DRC’s military population. A lack of reliable time-trend data for prevalence estimates of HIV in the DRC and other African countries makes it difficult to generalise when comparing changes in risk-related behaviours and HIV acquisition among populations. 6
Furthermore, the study does not represent a random sample of the entire Congolese military, but rather a convenience sample of those stationed in Kinshasa, an urban area. Results may not be generalisable to the entire military population. And the small sample size of women in the study (n = 164, 4.2%) is not representative of the entire military population (2.7%), and may be too small to detect a difference. In addition, the current study’s questionnaire did not include questions regarding the participant’s partner type.
While the prevalence of HIV infection has remained low and has been fairly stable over the past few decades in comparison to surrounding countries, it is important to continuously monitor the HIV/STI prevalence in high-risk populations in DRC. The high genetic heterogeneity of HIV found in DRC, high-risk sexual behaviours and increased mobility of the military population could result in changes to the HIV epidemic, especially if changes included increased risk due to the high-risk behaviours with the general population. 21 This study should be expanded to all regions of the country where military personnel are assigned, particularly those stationed in the eastern portion of DRC where ongoing conflict persists, to determine differences in infection rates and risk behaviours. Interventions targeting military personnel are critical components of national and international HIV/AIDS prevention and treatment strategies, and baseline information is essential in building these programmes.3,39
Study approval
The study protocol was approved by Human Subjects Protection Organizations at both the Kinshasa School of Public Health and United States Army Medical Research and Material Command.
Footnotes
Acknowledgements
We thank the government of the Democratic Republic of Congo, Ministry of Public Health and the Ministry of National Defense of the Democratic Republic of Congo for permission to undertake this study and the US Embassy in DRC for their continued support. We are sincerely grateful to the study participants, the field team and staff at Global Viral Forecasting (GVF) Cameroon for their technical support and professional commitment.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Department of Defense HIV/AIDS Prevention Program (DHAPP), Naval Health Research Center, San Diego, CA. CFD was supported, in part, by funds from the National Institutes of Health (NIH) Fogarty International Center (FIC) AIDS International Training and Research Program (2 D 43 TW000010-16/17). NDW is supported by the NIH Director’s Pioneer Award (DP1-OD000370). GVF is supported by the DoD HIV/AIDS Prevention Program (DHAPP), the Henry M. Jackson Foundation for the Advancement of Military Medicine,