
Abstract
In the UK there are limited data about university students’ risky sexual behaviour. A cross-sectional web-survey was conducted to investigate factors associated with high-risk sex among students at two UK universities. High-risk sex was reported by 25% of 1108. High personal sexually transmitted infection (STI) risk perception and permissive attitudes towards casual sex were associated with high-risk sex for both men (odds ratio [OR]: 12.12; 95% confidence interval [CI]: 4.10–35.81; OR: 2.49; 95%CI: 1.11–5.56, respectively) and women (OR: 22.31; 95% CI: 9.34–53.26; OR: 3.02; 95% CI: 1.82–5.01, respectively). For men, drinking alcohol (OR: 17.67; 95% CI: 1.90–164.23) and for women age and frequent drinking (OR: 2.02; 95% CI: 1.05–3.89; OR: 1.89; 95% CI: 1.08–3.31, respectively) were associated with high-risk sex. However, perceiving an average student as more likely to contract STIs (men, OR: 0.34; 95% CI: 0.16–0.75) or HIV (men, OR: 0.44; 95% CI: 0.20–0.96; women, OR: 0.42; 95% CI: 0.28–0.63) and finding it difficult to discuss sexual matters (women, OR: 0.60; 95% CI: 0.39–0.91) were negatively associated with high-risk sex. Most of the factors found were similar to other populations, but some psychosocial factors showed complex patterns of association that require further investigation.
Keywords
Introduction
Sexually transmitted infections (STIs) have remained a priority health area in the United Kingdom (UK). 1 At population level contracting STIs results in considerable morbidity or mortality2–4 and for healthcare providers, treatment and prevention efforts often leads to huge healthcare costs.5–7 Worldwide 8 and UK9,10 estimates consistently show that young people under 25 years old have the highest incidence and prevalence of most commonly diagnosed STIs, primarily attributed to high-risk sexual lifestyles.10–12 Most UK university students fall into this age group but there are limited data about their sexual behaviour. The dearth of literature in this important public health population in the UK has been noted earlier. 13 However, among the general British population repeat cross-sectional probability sample surveys exist (National Survey of Sexual Attitudes and Lifestyles [Natsal]) for men and women aged 16–59 years (Natsal-1), 16–44 years (Natsal-2) and 16–74 years (Natsal-3). 14
It is argued that university students are among the most sexually-active population groups 15 with several studies in the USA16–18 and the UK 19 showing a high proportion of at least 70% reporting being sexually active. Most importantly, a significant proportion of sexually active students engage in risky sex such as inconsistent condom use during penetrative vaginal or anal sex and having multiple sexual partners.17,19–22 Engaging in these behaviours theoretically increases the risk of acquiring STIs.
Currently there is great emphasis on social determinants of health.23,24 For sexual health, age, gender, religion, ethnicity, socio-economic status, area of residence and psychoactive substance use/misuse have been identified as some of the important factors that influence risky sex across populations.1,4,25–30 The general pattern in countries such as the UK and USA tends to show that younger people, men, less-religious individuals, some Black and minority ethnic groups, those of lower socio-economic status and/or urban residence and those who use/misuse alcohol and other drugs tend to report risky sexual behaviours. Interventions aimed at reducing risky sex in populations also tend to recommend the use of programmes with strong theoretical underpinnings. 31 Most theories of health behaviour have identified risk perception, self-efficacy, attitudes and behavioural intentions as key concepts that determine protective behaviours among populations.32–34
Our study is important because it is currently unclear if some of the factors listed above are associated with high-risk sex among UK university students. An understanding of the sexual behaviour of students is also important because it remains the key determinant of STI transmission. 35 Our study aimed to investigate the social and psychosocial factors associated with high-risk sexual behaviour among a sample of UK university students.
Methods
Participants and procedure
In November 2007, all registered students at two universities in a city in the north of England were invited to participate. A web-survey was considered ideal because it increases self-disclosure and uninhibited responses, 36 thus increasing the likelihood of collecting accurate sensitive sexual behaviour data.
Two weeks before survey activation, pre-notification posters were placed around the two university campuses. All students at one of the two universities were invited to participate via an email message (email group). Permission to send an email invitation to the other institution was declined by the local Research Ethics Committee due to concerns about the volume of email requests sent to students for research purposes. Consequently students from this institution were invited via an intranet announcement message (intranet group).
A study information sheet was included on the website and to activate the survey participants had to consent by clicking a radio button on the homepage. When the first survey page was activated participants were automatically assigned an anonymous identifier number. The survey was active for six weeks. Two weeks after activation one reminder email was sent to the email group but web administrators for the intranet group failed to broadcast a reminder. Fifteen cash prize draws of £100 were offered to all participants.
The questionnaire and measures
The questionnaire was adapted from Natsal-2. 12 The tool was modified into a self-completion web-survey and a pilot study was conducted with 20 university students. In general web-surveys should be short to complete, 37 therefore several survey items from the original Natsal-2 tool were dropped. Included items were those identified in the literature and in consultation with experts (clinicians, public health and sex survey practitioners) as key STI risk markers or important confounders. Household classification items from Natsal-2 were dropped, because these are less accurate proxy measures of social class for university students 38 and there is evidence suggesting that education attainment is more strongly associated with sexual behaviours than socio-economic status. 14
The main outcome of interest for our study was a sexual behaviour risk score coded as 1 (high-risk) or 0 (low-risk) behaviour. To be classified as having high-risk a participant had to report both having had two or more sexual partners and, inconsistently used condoms in the past year. Those reporting either; “no multiple partners” (1 or no sexual partner) or consistent condom use in the past year were classified as low-risk. This definition is similar to that of unsafe sex used by NATSAL 2000. 12
Statistical analyses
Data were analysed using SPSS (version 19) and statistical significance was considered as p ≤ 0.05. Initially, the relationship between high-risk sex and each potential explanatory variable were explored using Chi square or Fisher’s exact tests. Following this initial stage, stepwise logistic regression analysis was used to investigate the relative strength of these relationships. Gender was treated as an effect modifier because of the known sexual behaviour differences between men and women. 12 All statistically significant variables in the bivariate analyses were included in the stepwise regression models, age (for men) was also included because of its theoretical significance. 39 Initially both forward and backward stepwise procedures were used to find the model that best predicted high-risk sex.
Ethical approval
The study was approved by the University of Sheffield Research Ethics Committee.
Results
Of the approximately 49,891 students registered at the two universities at the time of the survey 3511 responded, thus providing a 7% conservative estimate of the response rate. The estimated response rate by mode of survey invitation is 13% (3101/23,194) for the email group and 1% (289/26,697) for the intranet group.
Participant characteristics.

aAll missing values relate to item non-response and exclude those who viewed the survey webpage but did not answer any question.
All subsequent analyses in this paper are based on those participants with linkable data (n = 1504). The majority were single (96%), drank alcohol (86%), aged under-25 years (83%), White ethnicity (82%), UK born (78%), women (60%) and did not belong to a religion (60%) (Table 1).
High-risk sexual behaviour
The valid data for the classification of risk behaviour were based upon respondents who did not have a missing value for either number of partners or consistency of condom use in the past year (n = 1108). Thus 25% (n = 281) of the eligible responding students were classified as having high-risk sexual behaviour. Twenty-seven percent of the total eligible women (n = 680) and 24% of eligible men (n = 422) were classified as having high-risk sexual behaviour.
Distribution of independent variables across risk groups.

aFisher’s exact test.
bReported one of these: prefer not to have sex; one regular partner but not living together; not married, but living with a partner, and no other sex partners; married with no other sex partners.
cReported one of these: no regular partners but casual partners when I feel like it; a few regular partners; not married, but living with a partner and with some sex activity outside the partnership; married, with some sex activity outside the marriage; have no idea.
Logistic regression
These data were further analysed using multiple logistic regression to examine which factors were jointly associated with high-risk sex. Although initially both stepwise models were used, ultimately the backward models were used as the final models because they had better data fit compared with the forward models as shown by the Hosmer and Lemeshow Goodness of Fit Tests (men: x2 = 2.96, degrees of freedom [df] = 6, p = 0.815 vs. x2 = 7.09, df = 5, p = 0.214, respectively; women: x2 = 5.72, df = 6, p = 0.456 vs. x2 = 10.26, df = 8, p = 0.247, respectively).
Final multivariate model of factors associated with high-risk sexual behaviour.
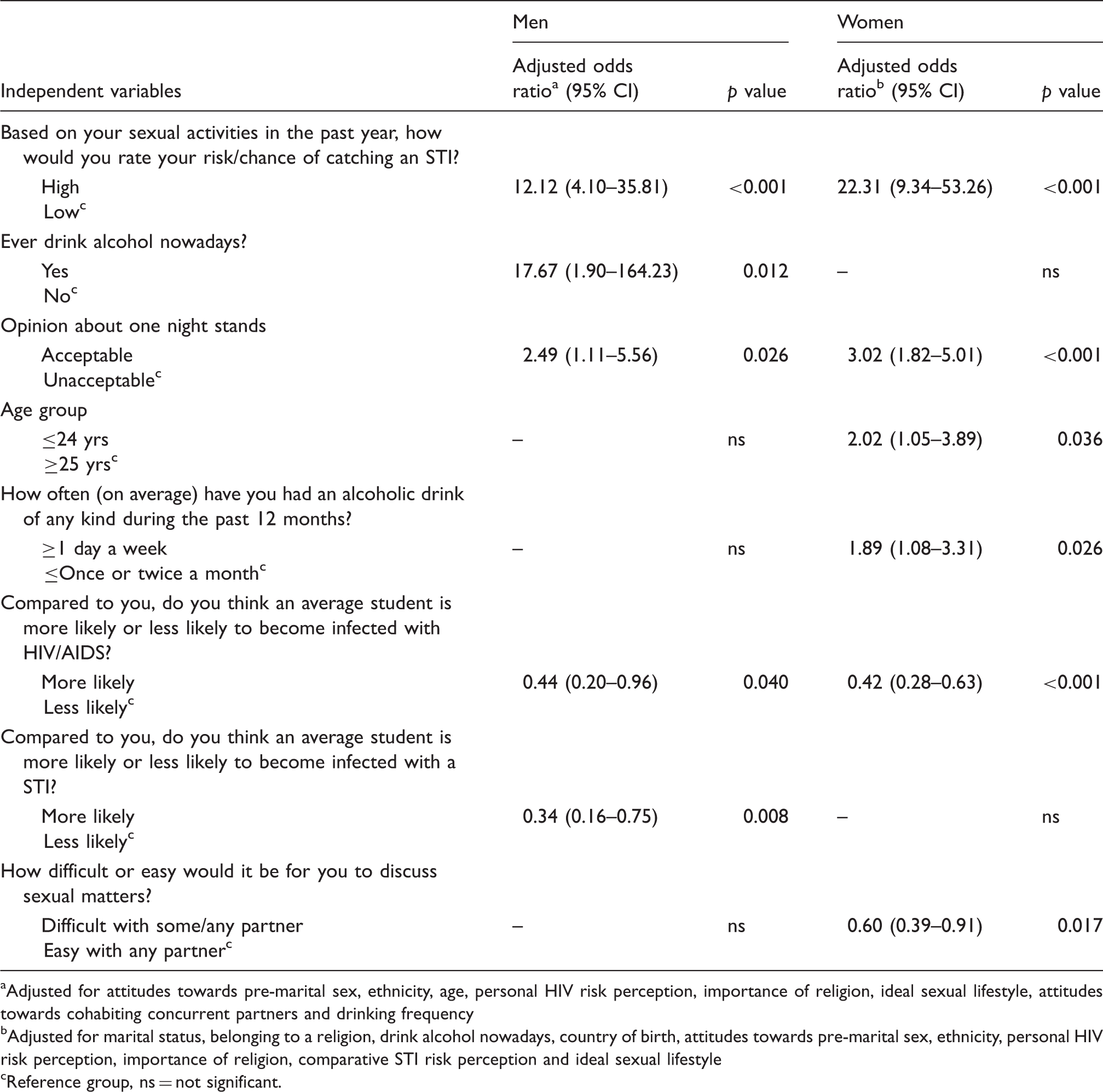
aAdjusted for attitudes towards pre-marital sex, ethnicity, age, personal HIV risk perception, importance of religion, ideal sexual lifestyle, attitudes towards cohabiting concurrent partners and drinking frequency
bAdjusted for marital status, belonging to a religion, drink alcohol nowadays, country of birth, attitudes towards pre-marital sex, ethnicity, personal HIV risk perception, importance of religion, comparative STI risk perception and ideal sexual lifestyle
cReference group, ns = not significant.
For women, factors associated with high-risk sex were: high personal STI risk perception (OR: 22.31; 95% CI: 9.34–53.26), permissive views about casual sex (OR: 3.02; CI: 1.82–5.01), younger students (OR: 2.02; CI: 1.05–3.89) and regular alcohol drinking (OR: 1.89; CI: 1.08–3.31). Finding it difficult to “discuss sexual matters with a partner” was negatively associated with high-risk sex (OR: 0.60; CI: 0.39–0.91). Perceiving an average student as more likely to contract HIV was also negatively associated with high-risk sex (OR: 0.42; CI: 0.28–0.63).
Discussion
A significant proportion of students with valid data reported high-risk sexual behaviour that increases their chances of contracting STIs. Our findings show a mixed pattern of risk factors associated with high-risk sex among students who responded to our survey. For example, high perceived personal STI risk and permissive attitudes towards casual sex were associated with high-risk sex for both men and women. However, younger age and regular alcohol drinking were associated with high-risk sex for women and ever drinking alcohol was associated with high-risk sex for men only. Interestingly, perceiving an average student as more likely to contract STIs (men) or HIV (men and women) and finding it difficult to discuss sexual matters with a partner were associated with low-risk rather than high-risk sex.
We tested the accuracy hypothesis 32 and found that high personal STI risk perception was strongly associated with high-risk sex for both men and women. This seems to be consistent with the idea that people who engage in risky behaviours have higher actual and perceived risk. 32 However, caution is needed when interpreting our findings because the majority of respondents who were classified as having high-risk sexual behaviour profile perceived themselves as being at low risk of contracting STIs. This may simply indicate that these students do not realise that their behaviours are risky 40 and this would be worrying because it may lead some to misjudge their need to take appropriate preventative action. In this scenario interventions that focus on improving knowledge or awareness of risky behaviours seem useful. However, interpretation of the relationship between risk perception and risky sex is complex especially when using cross-sectional data because the association can operate in the other direction such that people who engage in risky sexual behaviour might be expected to be those who also feel less worried about the likelihood of contracting STIs. 32 Therefore, a better understanding of the reasons for inaccurate risk perceptions is needed to enable us to recommend appropriate interventions to alter these errors.
One possible explanation could be the existence of optimistic bias 41 – the concept that, in general, people believe that they are less at risk compared to others around them. It is assumed that such belief lowers feelings of vulnerability thus affecting risk-reduction activities. 41 However, our findings seem to contradict this because a significant number of students who responded perceived themselves to be more at risk of contracting STIs (men only) and HIV (men and women) when compared with their peers. Our findings seem to be consistent with new evidence that suggests that optimistic bias is limited to certain contexts and it may not be as widespread as once thought.42,43
Alcohol consumption has been shown to be widely associated with risky sexual behaviour18,26,44–46 and our findings support this pattern for both men and women. However, infrequent alcohol use is not always associated with risky sex. 47 Our findings should be interpreted in the context of the ‘global-level of analysis’ used. That is, in these studies participants are typically asked their overall involvement in high-risk behaviour and this is related to general measures of alcohol use (like, “ever drink alcohol?”). 44 Although such studies typically show a strong association, they are considered methodologically limited because of their inability to establish co-occurrence of alcohol use and risky sex on the same occasion.44,48,49 Establishing such co-occurrence strengthens, but does not guarantee, an explanation of the causal mechanisms of this relationship.26,48
UK population estimates show that younger people are more likely to engage in risky sexual behaviour and this is collaborated by the disproportionately high STI rates in this group.9,10 Our findings partly support this trend, because for women the odds of engaging in high-risk sex were twice as high for younger students than older students. However, a reverse pattern whereby older students are more likely to report risky behaviour than their younger counterparts has been shown by others.50–52
Socio-cognitive theories postulate that preventive behaviour is largely influenced by cognitive process such as attitudes and beliefs. 53 Our study found that having permissive attitude towards casual sex was strongly associated with high-risk sex for both men and women. This finding is consistent with other studies that have shown that having liberal sexual attitudes is associated with risky sex.20,54,55 This suggests that students value and find casual sex highly desirable. This presents major challenges because prevention messages that solely focus on reducing casual sex may not be easily acceptable to students.
Interestingly, our findings suggest that feeling confident about the ability to ‘discuss sexual matters with a partner’ was associated with high-risk rather than low-risk sex for women. It is suggested that high levels of self-control increases the likelihood of participating in low-risk sex. 33 However, the direction of this relationship is complex especially when using cross-sectional data. For example, those who engage in high-risk sex in our study might have higher self-efficacy for discussing sexual matters than those who engage in low-risk sex simply as a consequence of their greater sexual experience.
Year and level of study were not associated with high-risk sex and this effect is similar to another UK study that used STI diagnosis as a risk indicator. 51 Although country of origin, religion, ethnicity and ideal sexual lifestyle were statistically bivariately associated with high-risk sex, during multivariate analyses these variables lost their statistical significance. This suggests that these factors might not be strongly associated with high-risk sex among students or are correlated with other factors in the regression. Interpretation of some of these findings should be considered with great caution because of the small numbers of non-UK-born students and those of non-White ethnicity. Our data did not show any difference in percentages of students who found it acceptable to have concurrent sexual relationships in cohabiting relationships compared with non-cohabiting relationships, suggesting that cohabitation may not be a reliable indicator of low-risk sex among students.
A key strength of our study is its web-survey methodology, which is acknowledged to be cost effective for large samples and tends to minimise social desirability biases often associated with self-reporting of sensitive behaviour.25,36,56 Although there is evidence showing gender similarities27,57 or diminishing differences 14 for some sexual behaviours, it is possible that the small gender differences we found in our risk estimates are partly due to the use of web-survey methods. Our study also suggests that email invitations and reminders can improve response rates for web-surveys compared with intranet banner advertisements. However, securing ethical approval for email invitations can be very difficult. Nonetheless, since UK university students have almost universal access to the internet, this methodology has great potential for delivering sexual health information 58 and monitoring temporal patterns of students’ risky sexual behaviour.
The prevalence estimate of high-risk sex in our study is limited by the self-selection nature of participants and low response rates. In addition, a technical programming error in our study resulted in some survey data being rendered unusable for this study, although a comparison between linkable and non-linkable data showed very small differences on key survey items. Nonetheless, the likelihood of differences in the responses of early and late respondents cannot be totally discounted. The cross-sectional nature of our data also potentially compounded the complex associations found for some psychosocial factors. Therefore, future studies should consider exploring these relationships using longitudinal designs.
The prevalence estimates of STIs among UK students is potentially low.51,52 This should not be viewed as evidence for inaction, because public health primarily focuses on intervening much earlier to ‘promote health’ and secondly to prevent onset of diseases. 59 At an individual level, primary and secondary prevention interventions aimed at reducing the number of sexual partners and consistent condom use could be useful for this university population. The former interventions aim to keep those uninfected from acquiring infection and the latter attempts to reduce the risk of those already infected infecting their partners. 60 Such interventions would be consistent with UK policy ambitions of prioritising prevention efforts to reduce sexual health burden. 1
Our findings show a mixed picture of factors associated with high-risk sex. However, most of these factors are similar to those observed in other populations in the UK and other countries. However, some of the psychosocial factors showed complex patterns of association that are ostensibly inconsistent with some key health behaviour theoretical concepts. Due to methodological limitations these patterns are tentative and require further investigation. The use of different proximate indicators for risky sex by different studies also greatly complicates the interpretation and understanding of similarities and differences of factors associated with risky sex across studies. Thus future studies should consider directly comparing university students and other important public health population groups in the same study. Our study provides useful baseline data which may be used to inform interventions that focus on reducing high-risk sex among UK university students.
Footnotes
Acknowledgements
We thank all students who participated; Mr Laurence Cornford (University of Sheffield) for programming the web-survey, Mr Alistair McGowan (University of Sheffield) for descrambling the web-survey data that were saved out of sequence; Dr Tracey Dibble, Tony Atkin, Ford Hickson and Catherine Mercer for their advice during design of the study and selection of key survey items; Dr Claudia Estcourt and Dr Georgina Jones for their constructive comments and advice on the final full research report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Sheffield Health and Social Research Consortium (Grant number: ZG64).