
Abstract
A 64-year-old Japanese woman was diagnosed as having Bowen’s disease on the vulva. The histopathological findings revealed papillomatosis, koilocytosis and clumping cells with atypical nuclei. Human papillomavirus DNA was not detected on polymerase chain reaction using consensus primers. The lesion was successfully treated with topical imiquimod 5% cream after two months. Histopathologically, no atypical cells were observed after treatment. Imiquimod can be a potential treatment modality for lesions that are difficult to treat with surgical excision.
Keywords
The immunomodulatory substance imiquimod has been used to treat skin disorders, such as condyloma acuminatum and actinic keratosis. In genital Bowen’s disease, treatment options such as excision and cryosurgery could bring about severe pain and persistent skin damage. We herein report a case of genital Bowen’s disease successfully treated with 5% imiquimod cream.
Case report
A 64-year-old woman noted small nodules on the vulva three years previously that had slowly increased in both size and number. The patient had been suffering from interstitial pneumonia and diabetic nephropathy. The patient had a history of cigarette smoking. A physical examination revealed multiple erosive reddish-to-white plaques on the vulva (Figure 1(a)). Black pigmented flecks were seen around the lesion. We suspected a diagnosis of extramammary Paget’s disease and performed a skin biopsy. A histopathological examination revealed hyperkeratosis, parakeratosis and acanthosis. Atypical keratinocytes had proliferated throughout the epidermis, and clumping cells were occasionally observed. The patient was diagnosed as having genital Bowen’s disease. Since genital Bowen’s disease is frequently associated with high-risk human papillomavirus (HPV), we performed HPV typing using consensus primers, L1C1/L1C2 and GP5+/GP6+, as described elsewhere, after obtaining the patient’s informed consent; however, no HPV DNA was detected.1–3 Furthermore, a gynaecological examination revealed no abnormal findings. Since her general medical condition was poor and it was difficult to perform surgical excision, the lesion was treated with 5% imiquimod cream topically three times a week, and the plaques disappeared clinically after two months (Figure 1(b)). We performed a skin biopsy again and confirmed that no tumour cells were present histopathologically.
Clinical appearance before and after treatment. (a) Multiple erosive reddish-to-white plaques around the patient’s left labium majus. Black pigmented flecks were observed around the lesion. The closed arrow indicates the lesion at which the first skin biopsy was performed. (b) The lesion after two months of imiquimod treatment. Almost all of the erythematous plaques and pigmented flecks had disappeared. The closed arrow indicates the lesion at which the second skin biopsy was performed.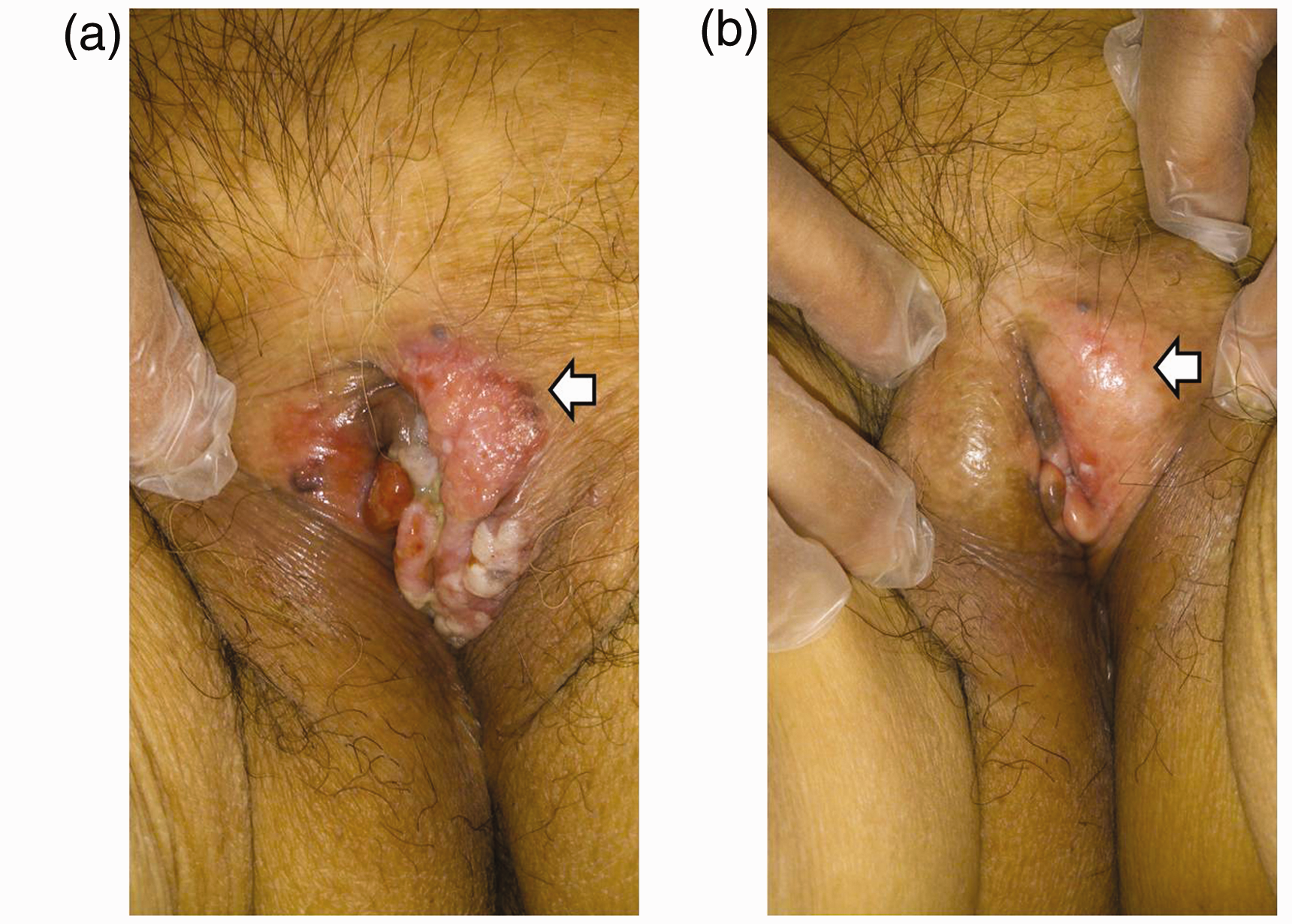
Discussion
Imiquimod 5% cream is a topical immune response modifier that has been approved in most pharmaceutical markets to treat anogenital warts, actinic keratosis and superficial basal cell carcinoma. Imiquimod is a heterocyclic imidazoquinoline with antiviral and antitumour effects. Imiquimod itself does not have antiviral or antiproliferative actions; its efficacy is ascribed to the stimulation of innate and acquired immunity.4,5
Patel et al. conducted a double-blind, placebo-controlled, randomised trial to evaluate the preliminary efficacy and safety of 5% imiquimod cream for the treatment of Bowen’s disease. They reported that 11 of 15 patients (73%) in the imiquimod group achieved resolution of Bowen’s disease; however, none in the placebo group, with no episodes of relapse during the 9-month follow-up period. 6 In our patient, the lesion was located around the labium majus, and it was difficult to perform surgical excision. Topical imiquimod cream can be a potential treatment modality for Bowen’s disease patients who are unsuitable for other treatments, such as surgery.
Bowen’s disease in the genital area and finger is frequently associated with high-risk types of HPV, such as HPV type 16, 56 and 58.2,7–9 Weisenseel et al. 10 reported a case of HPV type 73 associated with periungual Bowen’s disease that was successfully treated with topical imiquimod. On the other hand, no HPV-DNA was detected in our patient. Therefore, as Yanagishita et al. 5 reported, we considered that the Bowen’s disease lesion was resolved by the imiquimod treatment irrespective of HPV infection, possibly due to the antitumour effects by activating innate and acquired immunity. It is unclear whether HPV-positive Bowen’s disease is more responsive to topical imiquimod 5% cream than HPV-negative disease. The association between HPV infection and the effectiveness of imiquimod cream needs further investigation.
The name vulvar intraepithelial neoplasia (VIN) is sometimes used instead of genital Bowen’s disease. The term VIN is used to denote high-grade squamous lesions, subdivided into usual-type VIN lesions (including warty, basaloid and mixed VIN) and differentiated VIN lesions. Usual-type VIN is commonly associated with carcinogenic genotypes of HPV and other risk factors for HPV persistence, such as cigarette smoking and an immunocompromised status, whereas differentiated VIN is usually not associated with HPV and instead presents more often with vulvar dermatologic conditions, such as lichen sclerosus. Imiquimod has been reported to be a first-line treatment for VIN as long as the presence of invasion can be reasonably excluded. 11 The present case appeared to involve differentiated VIN associated with lichen sclerosus; however, we were unable to confirm the characteristic findings of lichen sclerosus histopathologically. Since the differentiated VIN associated with lichen sclerosus is more likely to occur in patients with squamous cell carcinoma of the vulva than usual-type VIN, 11 we should continue to follow the present patient for as long as possible.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.