
Abstract
Genital warts are very common in the under-18 years old population, yet treatment with imiquimod is currently off-label. We looked at 50 cases of genital warts in patients aged under 18 years who had been treated with Imiquimod to see if this treatment was effective, and it was.
INTRODUCTION
Imiquimod is an immune response modifier that activates the patient's own immune system to bring about clearance of genital warts. It is widely used in genitourinary medicine clinics and as it is a self-applied therapy for use at home, it is popular with patients. 1 It is, however, only licensed in the UK in adult patients (aged 18 years old or over). In the USA, imiquimod is licensed for patients aged 12 years and older. 2 A literature search conducted looking for evidence of off-label (i.e. not licensed for use in children or use outside of the terms of the product license) use of imiquimod in the under 18s produced a few papers. 3–6 The majority of the articles are case reports describing the use of the immunomodulator in children, the youngest being a six-month-old baby with successful clearance of warts and minimal side-effects.
A significant number of adolescents attend sexual health services – in 2007, 19,034 patients under 19 years were diagnosed with genital warts and this had risen from 14,687 in 2003. 7 With such a huge caseload it is inevitable that medical staff use imiquimod in adolescents. Drug trials in adolescents are time consuming, expensive and require rigorous ethical approval, and so it is unlikely that industry-funded trials will ever take place. We reviewed our use of imiquimod in a group of adolescents to look at tolerability, outcome and success rates.
We chronologically selected 50 patients less than 18 years of age from January 2006 to date, who had been prescribed imiquimod.
RESULTS
Patients were aged 13–17 years with the majority (28) being 17 (Figure 1). There were 40 female and 10 male patients. Three of the women were diabetic. Thirty-five patients required only one box, nine patients required two boxes, two patients required three, two patients required four, one patient required seven and one patient required 11 boxes (Figure 2). Imiquimod alone was the first treatment choice in 21 cases and in two cases was used at the same session in conjunction with cryotherapy or trichloroacetic acid (TCAA).

Age of 50 patients studied
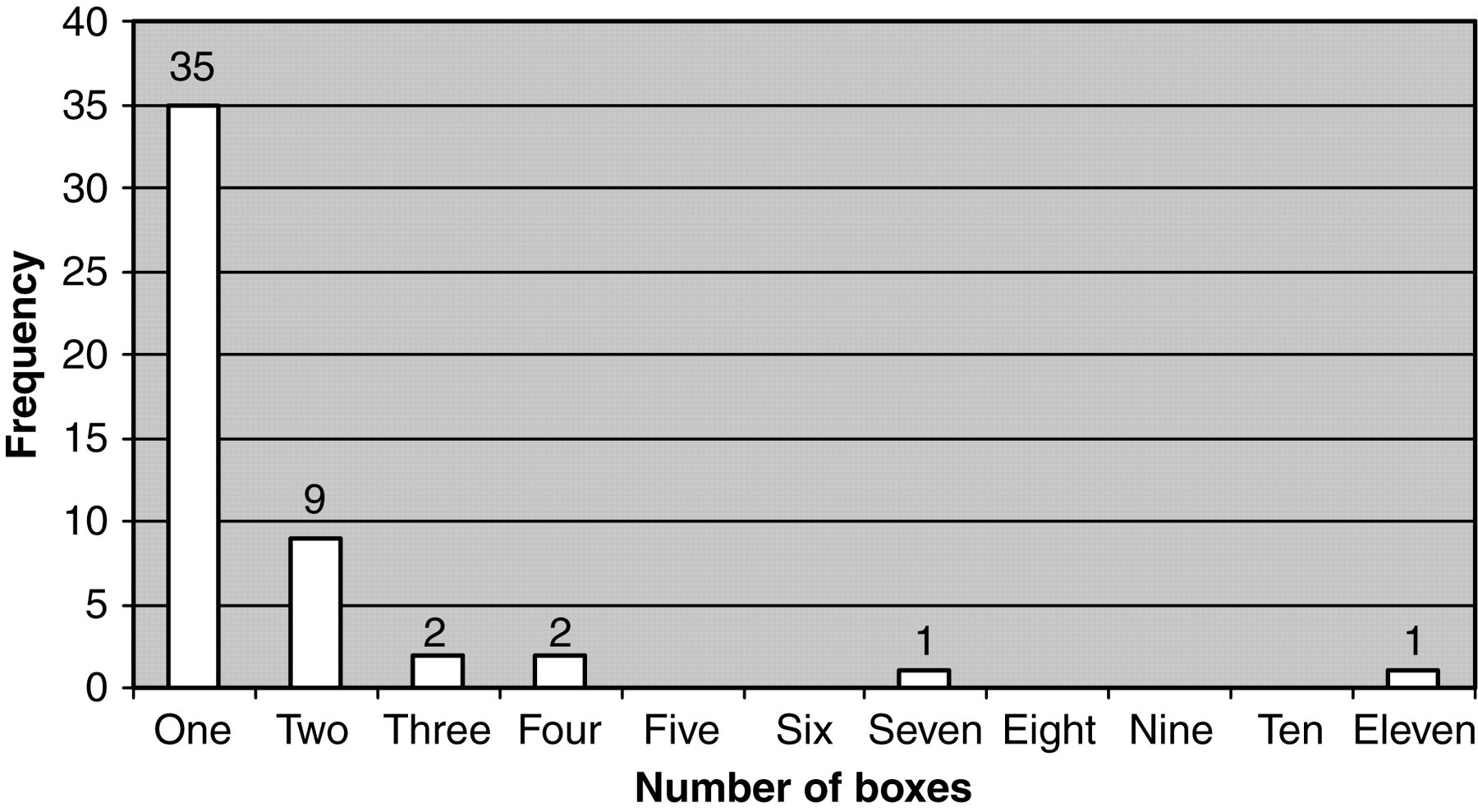
Number of boxes of imiquimod needed
Of the 45 patients successfully treated with imiquimod, only three reported any recurrence since imiquimod use. Of these three patients, one had a recurrence nine months later – cleared with podophyllotoxin, another had a recurrence 18 months later – cleared with imiquimod and the third patient had a recurrence three years later – cleared with combination of imiquimod and cryotherapy/TCAA acid. These could also have been due to re-infection with a different human papillomavirus (HPV) type.
Only five patients were unable to tolerate imiquimod and switched to alternative therapy. However, all five rapidly cleared their warts after further sessions of either cryotherapy or TCAA or, in the case of two patients, one tube of podophyllotoxin cream, to eradicate some non-keratinized residual warts. All five cleared their warts within three months of initial clinic presentation. Of the 45 patients successfully treated with imiquimod, 66% had full clearance in less than two months and 86% had full clearance in less than six months.
The side-effects were as expected using Imiquimod. Of the 45 patients, three reported slight soreness and one patient noted headaches after imiquimod use. These patients continued with the treatment until wart clearance.
The 17-year-old woman who required 11 boxes of imiquimod had no unusual features, i.e. she was not immuno-suppressed or diabetic. She did, however, have extensive vaginal warts as well as vulval warts. The warts reduced slowly over a one-year period with intermittent imiquimod use and in total her treatment took 15 months.
The youngest patient was 13-years-old and diabetic. Her older sister had been treated by us for genital warts. On presentation, she had thrush and extensive vulval warts (Figure 3). In children and very young adolescents, referral to paediatric surgery for clearance under general anaesthetic is preferred. However, this patient was deemed mature enough and was keen to use home therapy initially. After treating the thrush she applied imiquimod and at eight weeks the warts had resolved (Figure 4). The slight erythema seen in Figure 4 cleared and one year later there were no recurrences. Child protection services reviewed the case, but no issues were uncovered.

Before imiquimod treatment

After eight weeks of imiquimod treatment
DISCUSSION
Our review showed Imiquimod to be just as effective in the under-18 years old population. It is notable that so many of the patients cleared with just one box of imiquimod and almost 70% were clear within two months.
Combining destructive therapy like TCAA or cryotherapy with imiquimod treatment can speed up the process. 8 However, some young teenagers have high anxiety about being in the clinic and have low pain threshold, and so it is often inappropriate and unnecessary. The five patients who developed significant erythema from imiquimod may, of course, still have benefited from the treatment, as in all five further therapy with other modalities achieved wart clearance within three months of first visit.
In Australia, the use of Gardasil (a quadrivalent human papillomavirus [HPV] vaccine containing HPV types 6, 11, 16 and 18) has resulted in a 48% reduction in new female genital wart presentations. The UK decision to use Cervarix, which does not protect against genital warts, will ensure that genital warts continue to be a major financial burden on the National Health Service and sexual health services in particular. To cope with this ever-increasing workload, good home therapies in all age groups are necessary. Our review shows that imiquimod works well in the under 18s, is well tolerated and brings about rapid resolution. Such off-label use by medical staff is common but can it be used in a patient group directive (PGD)? The National Prescribing Centre states that ‘medicines can be used outside the terms of their Summary of Product Characteristics (SPC) (and so outside their license) provided such use is supported by best clinical practice. 9 The PGD should clearly state when the product is being used outside the terms of the SPC and why this use is necessary.’ We conclude that imiquimod works, is well tolerated in adolescents and can become part of a PGD.