
Abstract
A retrospective analysis of 86 HIV-1 vertically-infected Vietnamese children with a follow-up period >24 months after initiating antiretroviral therapy (ART) was performed from 2008 to 2012, to assess the outcome of first-line ART in resource-limited settings. Of the 86 children, 68 (79.1%) were treated successfully (plasma HIV-1 viral load [VL] <1000 copies/ml), and 63 (73.3%) had full viral suppression (VL <400 copies/ml) after 24 months of ART. No significant difference between successfully treated patients and failure groups was observed in VL, CD4+ T-cell count or clinical stage at baseline; age at ART start; or ART regimen. All 14 children with VL >5000 copies/ml, one of four children with VL 1000–5000 copies/ml and none with VL <1000 copies/ml developed reverse transcriptase inhibitor (RTI)-resistance mutations by 24 months of ART. Y181C and M184V/I were the most dominant non-nucleoside and nucleoside RTI-resistance mutations, respectively (13/15, 86.7%). These findings suggest that VL testing after 24 months of ART can be used to efficiently differentiate ART failures among HIV-1 vertically-infected children in resource-limited settings.
Keywords
Introduction
Globally, 3.3 million children (<15 years of age) were infected with HIV at the end of 2011, 1 and most (98%–99%) of them were from resource-limited settings, where an estimated 65% of pregnant women living with HIV received antiretroviral drugs for preventing mother-to-child transmission (PMTCT) in 2012. 2 An estimated coverage rate of antiretroviral therapy (ART) among children in need of ART was 34% in 2012. 2 The aim of ART is to suppress HIV to an undetectable level; this is the main approach in managing the clinical course of HIV infection. 3 Reports from low- and middle-income countries have demonstrated the benefits of paediatric ART.4–7 ART has been proven to effectively reduce morbidity, mortality and hospital admission in HIV-1-infected infants and children.8,9 HIV-infected infants and children now survive to adolescence and adulthood, and the challenges of providing HIV care are evolving into the challenges of providing both acute and chronic/lifelong care. 10
During long-term treatment, several factors must be assessed, including clinical response, immunological response, viral suppression and drug resistance mutations.3,11–13 According to the 2013 World Health Organization (WHO) guidelines, treatment failure is defined as (1) clinical failure, indicated by new or recurrent WHO stage 3 or 4 condition after 6 months of ART; (2) immunological failure, indicated by fall of CD4+ T-cell counts to pre-treatment level or below (CD4+ T-cell count of less than 200 cells/µl or percentage CD4+ T-cell count less than 10% for children younger than five years of age and CD4+ T-cell count of less than 100 cells/µl for children aged five years and above); or (3) virologic failure, indicated by plasma viral load above 1000 copies/ml based on two consecutive viral load measurements after 3 months with adherence support. 10 Although viral load (VL) testing and drug resistance testing are mainly used to identify cases of therapy failure and choose second-line regimens in developed countries, they are still not commonly available in resource-limited settings because of high cost. Their unavailability leaves clinical and immunological markers as the only means of assessing treatment failure in such settings.11,14–16
In Vietnam, by the end of 2011, the estimated number of HIV-1-infected individuals exceeded 197,000, of whom 3900 (1.98%) were children. 17 A national ART prophylaxis programme for PMTCT was introduced in 2006, 18 and an estimated coverage rate of PMTCT increased from 9.2% in 2006 to 32.3% in 2009. 19 ART has been used to treat HIV-1-infected children since 2006. As of the end of 2011, over 3200 children were on ART. 17 However, only a few studies about ART outcome among HIV-1-infected children in Vietnam are available, such as cross-sectional studies among children with drug-naïve or treatment-experienced ART failure in Southern Vietnam.20,21 No reports have documented the long-term outcome of ART among Vietnamese children.
In the current study, we examined the response to first-line ART, evaluated clinical and immunological criteria to define virologic treatment failure and determined the profile of drug-resistance mutations among HIV-infected Vietnamese children after two years of ART in order to determine appropriate marker(s) for monitoring children on ART in resource-limited settings.
Subjects and methods
Study setting and subjects
Characteristics of HIV-1-infected Vietnamese children on ART.
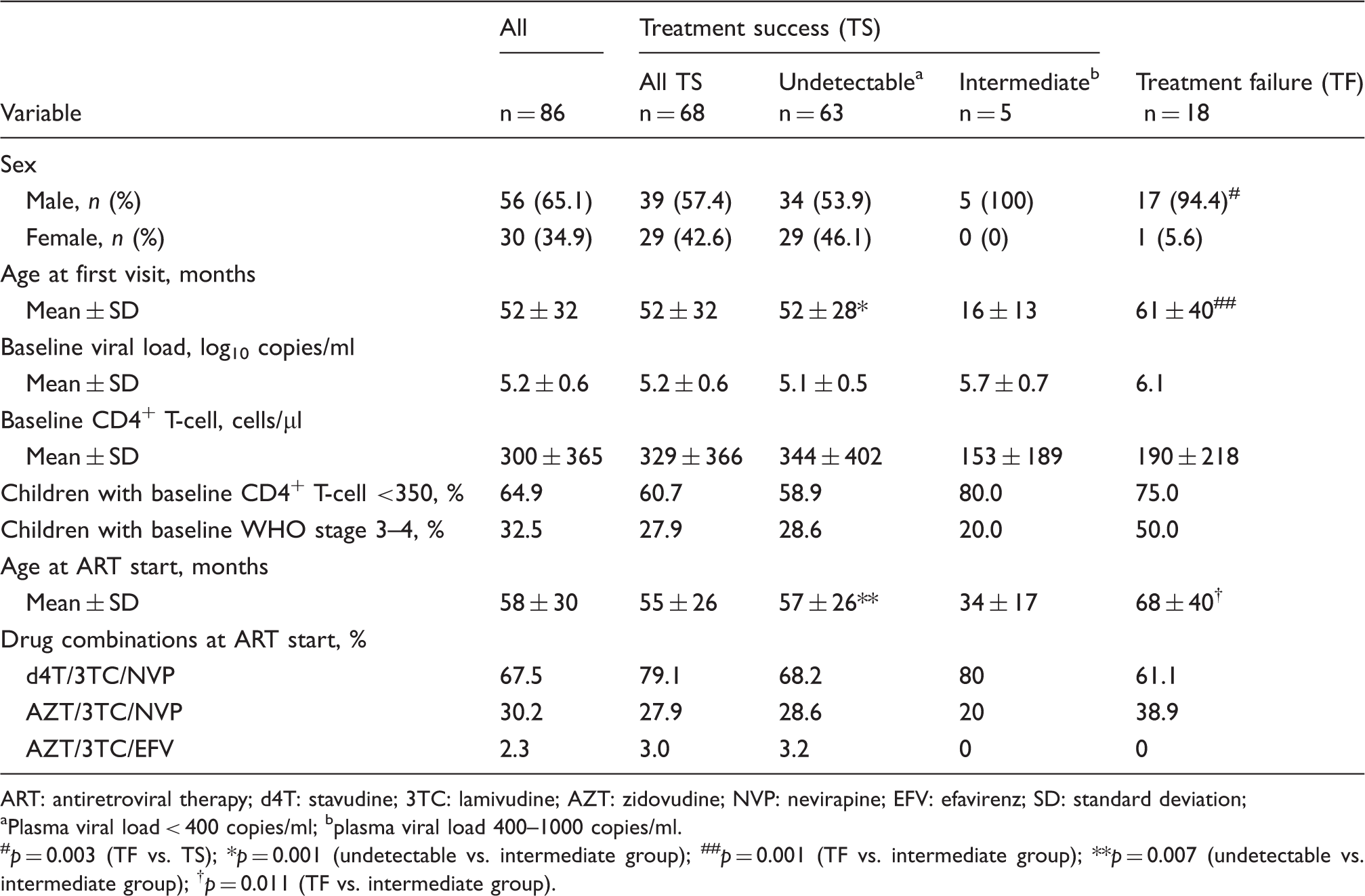
ART: antiretroviral therapy; d4T: stavudine; 3TC: lamivudine; AZT: zidovudine; NVP: nevirapine; EFV: efavirenz; SD: standard deviation;
Plasma viral load < 400 copies/ml; bplasma viral load 400–1000 copies/ml.
#p = 0.003 (TF vs. TS); *p = 0.001 (undetectable vs. intermediate group); ##p = 0.001 (TF vs. intermediate group); **p = 0.007 (undetectable vs. intermediate group);
First-line ART in this study consisted of two nucleoside reverse transcriptase inhibitors (NRTIs: stavudine [67.5%] or zidovudine [32.5%] and lamivudine [100%]) and one non-nucleoside reverse transcriptase inhibitor (NNRTI: mostly nevirapine [97.7%]), as described in the Vietnam Ministry of Health treatment guidelines (Table 1). 22 During the study period, the national guideline of HIV/AIDS treatment in Vietnam was changed from version 2005 to version 2010. Of the 86 participants, 55 children started ART under the criteria of the 2005 guideline: two children at the age of <18 months with WHO clinical stage 3–4 and/or % CD4+ T-cells < 20%; and 53 children at the age of >18 months with WHO clinical stage 3–4 and/or % CD4+ T-cells <15%. The remaining 31 children started ART under the criteria of the 2010 guideline: one child at the age of <12 months with confirmed HIV infection (RNA/DNA based), who was at five months of age and in WHO clinical stage 4; and 30 children at the age of >12 months with WHO clinical stage 3–4 and/or CD4+ T-cells < 20% (12–35 months of age) or <15% (≥36 months of age). 22 In the current study, ‘Treatment success’ was defined as VL ≤1000 copies/ml and ‘Treatment failure’ as VL >1000 copies/ml at 24 months after ART initiation. 10
Two children had joined the PMTCT programme with single-dose nevirapine (200 mg) for their mothers and multi-dose zidovudine for the children, who were given three doses (ID: 1110) and 27 doses of zidovudine (2 mg/kg/6 h; ID: 1372), respectively, but not given nevirapine syrup because it was not available. The two children were born in September 2006 and in October 2008 and started ART at the age of 20 and 24 months, respectively.
Laboratory methods
Peripheral CD4+ T-cell counts were determined with quarterly use of a Partec Flow Cytometry (Munster, Germany) and biannual quantification of VL using the Amplicor HIV-1 Monitor kit version 1.5 or Cobas Taqman HIV-1 test (Roche Diagnostics, Alameda, CA) with a detection limit of 400 copies/ml according to the manufacturer’s instructions. Sample plasma for the Cobas Taqman HIV-1 test (detection limit, 40 copies/ml) was diluted to 1:10, resulting in a detection limit of 400 copies/ml.
HIV-1 RNA was extracted from 100 µl of plasma using SMITEST EX-R and D (Genome Science Laboratories, Fukushima, Japan) according to the manufacturer’s instructions. The HIV-1 reverse-transcriptase (RT) gene was amplified, and population sequencing was performed as previously described.23–27 The HIV-1 RT nucleotide sequences obtained from each child biannually during the first 24 months of ART were analysed for previously reported drug-resistance mutations using the Stanford university HIV database (http://hivdb.stanford.edu/pages/algs/HIVdb.html/) and the mutation panel from the International AIDS Society USA (IAS-USA), November 2011 (http://www.iasusa.org/resistance_mutations). The REGA HIV-1 subtyping tool (http://hivdb.stanford.edu/) was used to determine HIV-1 subtype..
Statistical analysis
Pairwise comparisons were made in demographic, virologic and immunological parameters between treatment success and treatment failure groups using Student’s t-test, the chi-squared test or Fisher’s exact test.
Results
Outcome of anti-retroviral therapy
Changes of VL after ART initiation are shown in Figure 1. Of the 86 children studied, VL was suppressed to ≤1000 copies/mL after 24 months of ART in 68 (79.1%) children (Treatment success [TS] group). Of the 68 successfully treated children, VL was suppressed to an undetectable level (VL<400 copies/mL) in 63 children (TS-undetectable group); five children had a detectable VL (400–1000 copies/mL; TS-intermediate group). In the remaining 18 children (20.9%), VL was not suppressed to ≤1000 copies/mL after 24 months of ART (Treatment failure group). Although baseline VL was slightly higher in treatment failure group (106.1 copies/ml) than in success group (105.2 copies/ml), there was no significant difference between the two groups (Table 1, Figure 1).
Changes in plasma viral load after initiating antiretroviral therapy (ART) among HIV-1-infected children. UD (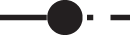 ): plasma viral load (VL) suppressed less than 400 copies/ml after 24 months of ART; Int (
): plasma viral load (VL) suppressed less than 400 copies/ml after 24 months of ART; Int ( ): VL remained 400-1000 copies/ml after 24 months of ART; TF (
): VL remained 400-1000 copies/ml after 24 months of ART; TF ( ): VL > 1000 copies/ml by 24th month of ART.
): VL > 1000 copies/ml by 24th month of ART.
Of the 86 children studied, 55 started ART under the criteria of 2005 guideline and nine of the 55 children (16.4%) failed treatment after 24 months of ART, while the remaining 31 started ART under the criteria of 2010 guideline and nine of the 31 children (29.0%) failed treatment. There was no significant difference in treatment failure rate between the two ART-initiating criteria (p = 0.165). In this study, most of the children (93.0%, 80/86) started ART after 24 months of age (Age at ART start <12 months of age [n = 1], 12–24 months [n = 5], 24–48 months [n = 28] and over 48 months [n = 52]), and there was no significant difference in treatment failure rate among those age groups (0% [0/1], 20% [1/5], 17.9% [5/28] and 23.1% [12/52], respectively; p = 0.966).
Characteristics of children who carried drug-resistant HIV-1 mutations after 24 months of first-line ART.
ART: antiretroviral therapy; d4T: stavudine; 3TC: lamivudine; AZT: zidovudine; NVP: nevirapine; ABC: abacavir; LPVr: lopinavir/ritonavir; VL: viral load; mo: months.
d4T was withdrawn from stock.
AZT adverse event, thrombocytopenia.
Child 1377 was treated with d4T/3TC/NVP for 9 months, with AZT/3TC/NVP from 9 to 15 months after initiation of ART, and with ABC/3TC/LPVr (second-line ART) thereafter.
VL at 15 months of ART was used to assess the outcome of ART.
No deaths occurred during follow-up. However, one child (ID: 1321) had to change from a zidovudine-containing regimen to a stavudine-containing regimen because of a zidovudine-associated adverse event (an episode of thrombocytopenia). Another child (ID: 1377) was treated with stavudine-containing regimen for nine months, and with zidovudine-containing regimen from 9 to 15 months after initiation of ART, and had to change the regimen to second-line ART (abacavir/lamivudine/lopinavir/ritonavir) because of high VL (500,783 copies/ml) at 15 months of ART, which was used to assess the outcome of ART (Table 2).
Clinical response
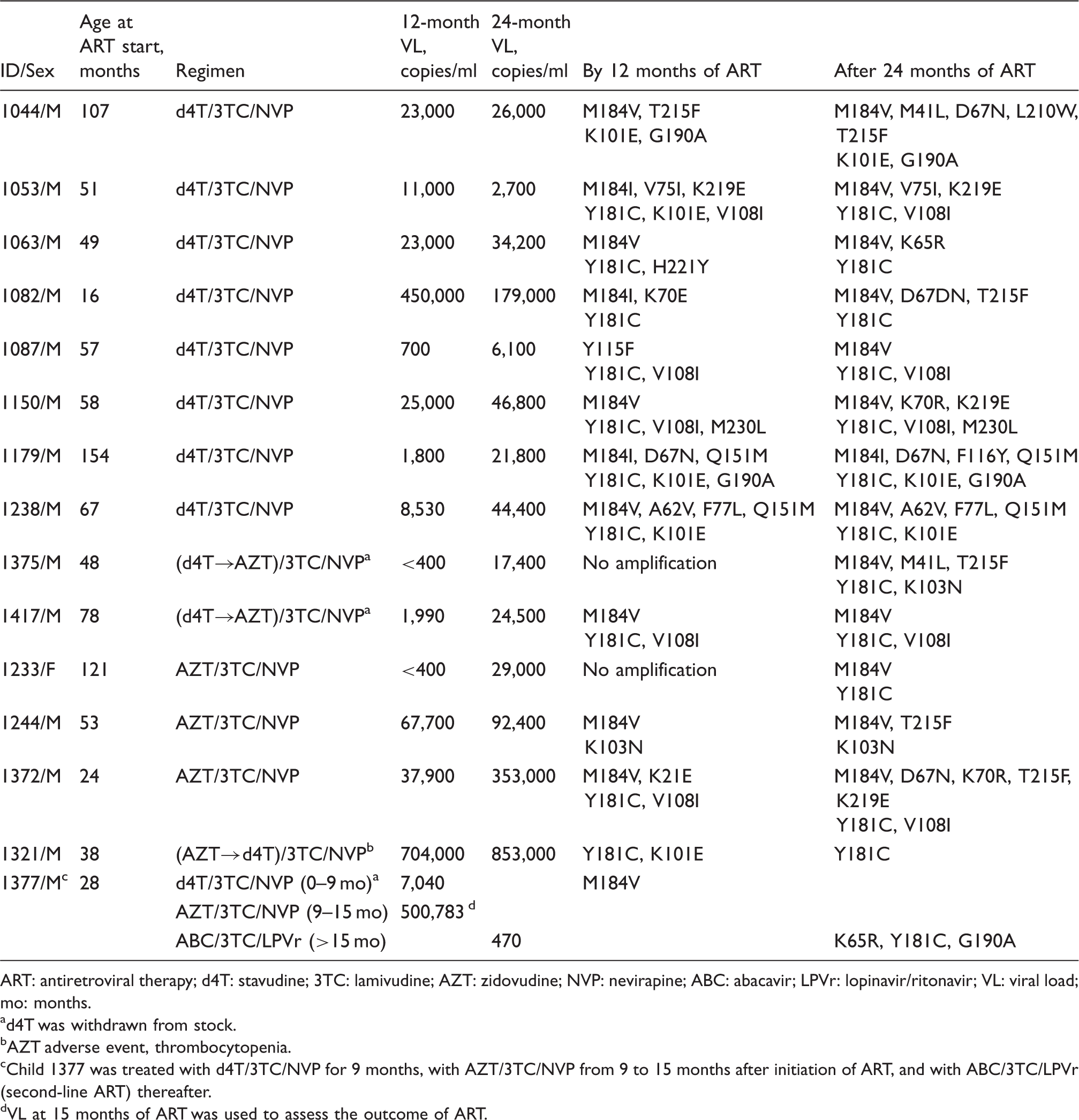
Number and percentage of children with WHO clinical stage 3–4 before and after initiating ART.
ART: antiretroviral therapy; CNS: central nervous system.
p = 0.0496.
Immunological response
Changes in CD4+ T-cell counts before and after ART initiation are shown in Figure 2. At baseline, CD4+ T-cell counts were lower in the treatment failure group (190 ± 218 cells/µL) than in the success group (329 ± 366 cells/µL), and lower in children with VL 400–1000 copies/ml (153 ± 189 cells/µL) than in children with undetectable VL (344 ± 402 cells/µL), though these differences were not statistically significant (0.1 < p < 0.2 and p > 0.2, respectively; Table 1). In successfully treated children, CD4+ T-cell counts continued to increase up to 24 months after ART initiation. In contrast, CD4+ T-cell counts of children with treatment failure increased for the first six months of ART and remained level during months 6 to 24. After 24 months of ART, CD4+ T-cell counts were significantly lower in children with treatment failure than in successfully treated children (p = 0.001). However, 24 months after initiating ART, the CD4+ T-cell counts of children with treatment failure were still twice as high as they had been at baseline (mean: 508 vs. 190 cells/µL). After 24 months of ART, one child with treatment failure (5.6%) had a CD4+ T-cell count <100 cells/µL, a WHO criterion for immunological failure in children older than five years on ART. Thus, the sensitivity of the WHO immunological marker was only 5.6%.
Changes in peripheral CD4+ T-cell counts after initiating antiretroviral therapy (ART) among HIV-1-infected children. UD ( ): plasma viral load (VL) suppressed less than 400 copies/ml after 24 months of ART; Int (
): plasma viral load (VL) suppressed less than 400 copies/ml after 24 months of ART; Int ( ): VL remained 400–1000 copies/ml after 24 months of ART; TF (
): VL remained 400–1000 copies/ml after 24 months of ART; TF ( ): VL > 1000 copies/ml by 24th month of ART. #p = 0.001.
): VL > 1000 copies/ml by 24th month of ART. #p = 0.001.
Drug resistance mutations
The profiles of reverse transcriptase inhibitor (RTI)-resistance mutations found in the current study are summarised in Table 2. Of the 18 children who failed therapy, 14 had VL > 5000 copies/ml, which is a former criteria for virological failure (2010 WHO guideline), 28 and the remaining four had VL 1000–5000 copies/ml after 24 months of ART. All the 14 children with VL > 5000 copies/ml, and one of the four children with VL 1000–5000 developed RTI-resistance mutations by 24 months of ART. Of the 68 children who were treated successfully (VL < 1000), no child developed RTI-resistance mutations. No RTI-resistance mutations were found at baseline, though only 15 plasma samples were available at baseline. Y181C, a nevirapine-induced mutation, 26 was the most dominant NNRTI-resistant mutation (13/15), followed by V108I (5/15). M184V/I, a lamivudine-resistant mutation, was the most prevalent NRTI-resistant mutation (13/15). Two children developed Q151M complex (Q151M, A62V, V77L or F116Y) and four children developed thymidine analogue-associated mutations (TAMs), such as M41L, D67N, K70R, T215F and K219E. One of the four children whose virus developed TAMs was the child (ID: 1372) who had been exposed to 27 doses of zidovudine (2 mg/kg/6 h) through the PMTCT programme. Of the NRTI-resistant mutations M184V and K219E appeared first (after six months of ART) in this child, and D67N, K70R and T215F appeared after 12 months of ART, while Y181C, the most dominant NNRTI-resistant mutation in this study, appeared after six months of ART. No baseline sample of this child was available. No protease inhibitor-resistance mutations were found in the current study.
HIV-1 genotypic analysis based on RT sequences revealed that all the children were infected with HIV-1 CRF01_AE. No significant difference was observed between treatment success and failure groups regarding VL, CD4+ T-cell count or clinical stage at baseline; age at ART start; or ART regimen; however, the male-to-female ratio was significantly higher in the failure group than in the success group (p = 0.003).
The sequences obtained in this study were deposited with Genebank under accession numbers: KC841163-KC841247.
Discussion
In the current study, we followed 86 HIV-1-positive, vertically infected Vietnamese children who were on first-line ART for at least 24 months. After 24 months of ART, 79.1% children were in treatment success (VL < 1000 copies/ml) and 73.3% had fully suppressed HIV-1 (VL < 400 copies/mL). This outcome is comparable to those of cohorts of Thai and European children13,14,29 and a meta-analysis of the studies in resource-limited settings, 30 and better than outcomes of the similar studies in African countries.12,31–33 In those African countries, anti-retroviral drugs were acquired through charity and prescription depended on drug availability by mid-2000, which might have affected ART compliance and therefore the higher failure rate. 33 All children who participated in the current study were infected with CRF01_AE; in comparison, multiple HIV-1 subtypes are circulating in Africa, which might help to explain the difference in ART outcome between Vietnam and studied African countries. Furthermore, our findings are comparable to the recently reported ART outcomes among Vietnamese adults with 70% having full viral suppression; 34 however, ART failure appears to be more frequent in children than in adults, possibly because of the differences in the prevalence and profile of drug-resistance mutations in children, particularly those who were on PMTCT, compared with adults,35–40 inadequate adherence due to unpalatable taste and/or inaccurate dosing for children of the medication. 41 This is the first longitudinal study of HIV-1-infected children on first-line ART in Vietnam.
In the current study, participating children infected with HIV-1 visited the hospital for the first time at the age of 52 months and started ART at the age of 58 months; 64.9% of participants initiated ART with CD4+ T-cell counts <350 cells/µL, and 32.5% of participants were in WHO clinical stage 3 or 4 when at the time of ART initiation (Table 1). These findings show that most vertically-infected, HIV-1-positive children in Vietnam have been identified after their diseases have progressed to a considerably advanced stage, rather than in the early stage of their lives. In addition, children with undetectable VL had higher baseline CD4+ T-cell counts than the children with VL 400–1000 copies/ml or VL > 1000 copies/ml after 24 months of ART (treatment failure group), though these differences were not statistically significant (p > 0.2 and 0.1 < p < 0.2, respectively). Therefore, the establishment of an early diagnostic system for vertical HIV-1 infection might improve ART outcomes in Vietnam. However, the current ART outcomes among Vietnamese children (79.1% ART success rate after 24 months of ART) are already comparable to global outcomes.
Clinical and immunological monitoring has been used to differentiate ART failure in resource-limited settings. In the current study, however, the WHO clinical and immunological criteria were able to differentiate only 11.1% and 5.6%, respectively, of children who were in virologic failure 24 months after initiating ART. These findings confirm that clinical and immunological parameters are less sensitive and less accurate for predicting treatment failure,11,14–16 which may delay proper timing for changing to a second-line regimen in children who experience treatment failure in resource-limited settings.
A previous study in Kenya proposed that VL testing 24 months after initiating ART could be used to efficiently differentiate ART failures among vertically-infected children with HIV-1 in resource-limited settings. 33 This proposal is also applicable to the current study. None of the 68 successfully treated children (VL < 1000 copies/ml) had HIV-1 with drug-resistance mutation(s) after 24 months of ART. All the 14 children with VL > 5000 copies/ml and one of the four children with VL 1000–5000 copies/ml developed RTI-resistance mutations by 24 months of ART. These findings suggest that adopting the threshold of 1000 copies/ml (2013 WHO guideline 10 ) could potentially catch failures before resistance mutations have time to emerge. Additionally, for the children with VL 1000–5000 copies/ml after 24 months of ART, drug resistance testing would be needed to identify those failing therapy in the near future, even in resource-limited settings.
A total of 15 children who failed therapy developed RTI-resistance mutations. The M184V/I mutation, which is directly associated with the widespread use of lamivudine, was the most common NRTI-resistance mutation. This makes sense, given that all participants in this study were treated with a lamivudine-containing regimen. Two children developed broad-spectrum Q151M complex NRTI-resistance mutations (Q151M, A62V, V77L or F116Y), even though the Q151M complex mutations are not common in ART-experienced European and African individuals.12,32,33,42 The Q151M complex mutations might be favorable for HIV-1 CRF01_AE. The Y181C mutation was the most common NNRTI-resistance mutation in this study, while K103N was rarely observed. This result is consistent with those of previous studies on ART-naïve and/or -experienced children and adults in Vietnam and Thailand.20,23,34,43,44 In this study, 97.7% of the children were treated with a nevirapine-based regimen. Our results are consistent with a large European cohort study that reported Y181C as a nevirapine-induced mutation and K103N as an efavirenz-specific mutation, 42 although K103N has also been reported as the most common NNRTI-resistant mutation among African patients on nevirapine-based regimens.12,32,33
In the current study, only two children had joined the national PMTCT programme which was introduced in Vietnam in 2006. 18 Of the 86 children studied, 66 were born before 2006 and had no chance to join the programme. Of the remaining 20 children, 12 were born in 2006, two in 2007, five in 2008, and one in 2009. An estimated coverage rate of PMTCT in Vietnam was 9.2% in 2006, 13.9% in 2007, 32.9% in 2008, and 32.3% in 2009. 18 Therefore, the number of children who were on PMTCT in this study was in the expected range. Of the two children who were on the PMTCT programme one child, who had been exposed to 3 doses of zidovudine, was treated successfully, while the other, who had been exposed to 27 doses of zidovudine, failed treatment. Because their baseline samples were not available, it was unable to confirm if their infected virus strains harboured drug-resistance mutations at baseline and affected their ART outcomes.
In the current study, male patients demonstrated a significantly higher tendency toward therapy failure than female patients (30.4% [17/56] vs. 3.3% [1/30]; p = 0.029), even though no significant difference was observed between male and female patients regarding VL, CD4+ T-cell count or clinical stage at baseline, age at ART start, or ART regimen. The reason for this finding is unclear, and further study is warranted to confirm it.
In conclusion, this is the first longitudinal study to document paediatric ART outcome in Vietnam, which is better than outcomes reported in Africa, and equivalent to outcomes of adults in Vietnam. VL testing 24 months after initiating ART can be used to efficiently differentiate ART failures among vertically-infected children with HIV-1 in resource-limited settings.
Contributorship
LV Nguyen and DTK Khu: clinical follow-up of HIV-1 infected children; HV Pham, A Ishizaki, and X Bi: genetic analysis of HIV-1 and preparation of manuscript; CTT Phan, TTB Phung, K Takemoto and PN An: plasma sample collection, laboratory testing, and plasma HIV-1 RNA testing; H Ichimura: control of the current study and preparation of manuscript.
Footnotes
Acknowledgements
The authors are grateful to the children who participated in this study for their invaluable support through the use of their blood samples.
{kind=link}