
Abstract
Summary
Human papillomavirus is a common sexually transmitted infection and the causative agent for cervical cancer, a frequently occurring malignant disease among women in developing countries. We assessed human papillomavirus awareness prior to the delivery of a brief information and education intervention, and human papillomavirus vaccine provision to female entertainment and sex workers (N = 220). At baseline, only 23.6% of women had heard of human papillomavirus. Following the educational intervention, 90% answered all the human papillomavirus knowledge questions correctly. Of 192 participants attending the first quarterly cohort visit where vaccine was offered, 149 (78%) were eligible for vaccination; HIV-positive (n = 32) and pregnant (n = 11) women were excluded. Acceptance of vaccine among eligible women was universal, and 79.2% completed the three-dose vaccination series. Women who reported use of amphetamine-type stimulants had significantly and independently lower odds of vaccine completion (adjusted odds ratio [AOR] 0.24; 95% confidence interval [CI] 0.08, 0.69). New pregnancies also had an impact on vaccine completion: 5.4% (8/149 5.4%) who started the series had to stop due to new pregnancy. Results demonstrate the effectiveness of a simple education intervention designed to increase human papillomavirus knowledge and the feasibility of successful human papillomavirus vaccine in a population that is often difficult to engage in preventive health care.
Keywords
Introduction
Human papillomavirus (HPV) is one of the most common sexually transmitted infections (STIs) globally, with worldwide age-adjusted point prevalence in women estimated to be 11–12%, and most women under 25 have been infected.1–3 Certain genotypes (especially 16 and 18, which make up 60–70% of infections) of HPV are recognized as the primary cause of cervical cancer,2,4–6 the third most commonly occurring cancer in women globally, and the fourth ranked cause of cancer mortality (respectively, second and third ranked after age adjustment) 7 responsible for 7.8 million years of life lost worldwide. 1 The greatest burden of mortality is in developing countries, which account for up to 88% of the estimated 530,000 deaths annually, 8 and where the cytological screening programmes that have been effective in reducing cervical cancer deaths have not been readily adopted. 5
In addition to sexual behavioural factors such as early age of sex, numbers of partners, and inconsistent condom use, the risk of HPV infection is associated with smoking, oral contraceptive use, and other STIs.6,9 Younger, sexually-active populations are most at risk of HPV and older women are at higher risk of cancer. Women engaging in transactional sex have a disproportionately high risk for multiple and recurrent 10 HPV infection and the subsequent development of cervical and other types of cancer.6,9,10
HPV vaccines have the potential to significantly reduce the morbidity and mortality from cervical cancer.11–13 The two commercially available vaccines, Gardasil® and Cervarix®, target the HPV genotypes recognized as causing most cervical cancer (HPV types 16 and 18), and Gardasil® also targets types that cause genital warts (HPV types 6 and 11). The vaccines have close to 100% protective efficacy against these types of HPV infection when administered to women without previous infection14–16 and are also effective in reducing progression to neoplasia in women who have been previously exposed.17,18 Both vaccines require a three-dose series administered over six months.
Given the high worldwide incidence of cervical cancer, the implementation of high-quality HPV vaccination programmes is emerging as a priority for many developing countries. 19 Despite the advances in HPV detection and the development of highly efficacious prophylactic vaccines, feasibility studies have shown low levels of knowledge and awareness of HPV and cervical cancer.20,21 HPV vaccination programmes in developing countries face formative and programmatic implementation challenges, as well as resource limitations; however, among young girls (age 9–13 years) school- and health-centre-based delivery can result in high coverage rates. 19 Less is known regarding how vaccination programmes can be effectively targeted to high-risk women, but achieving high rates of coverage and completion will require some understanding of the knowledge and attitudes towards HPV and the HPV vaccine. There is at present very little information on HPV-related knowledge and attitudes among adult women in the Asia Pacific region, and especially very high risk women such as female entertainment and sex workers (FESW). 22
Cambodia has one of the highest rates of cervical cancer in the Asia Pacific region. In the context of a cohort study of young women at high risk for STIs, we investigated knowledge of HPV prior to and following the provision of two brief HPV information and education sessions. We then measured subsequent acceptance and uptake of the three-dose quadrivalent vaccine (Gardasil®) series for eligible women.
Methods
Study population
The study population consisted of a convenience sample of 220 FESW in Phnom Penh, Cambodia, who participated in the Young Women’s Health Study 2 (YWHS-2), 23 described in detail elsewhere.10,24,25 Briefly, the YWHS-2 was a prospective study conducted from August 2009 to August 2010 on the prevalence and incidence of STIs and HIV, sexual behaviours, reproductive health practices, drug use, and sociocultural determinants of HIV infection amongst FESW. Eligible participants were biologically female, 15–29 years old, of self-identified Cambodian ethnicity, understood spoken Khmer, able to provide informed consent, and reported two or more sex partners or engagement in transactional sex within three months of study enrolment. Outreach for recruitment and retention was conducted by the Cambodia Women’s Development Association (CWDA) who visited women at community locations proximal to where they worked and lived throughout the study period. They were asked to attend quarterly visits for data (including behavioural surveys) and specimen (including for HIV, HPV, and biomarker tests for semen [prostate specific antigen] and amphetamine-type stimulants [ATS]). Women were compensated US$5 for each study visit they attended, whether or not they received HPV vaccine. The study protocols were reviewed and approved by Institutional Review Board of the Committee on Human Research at UCSF, the Cambodian National Ethics Committee, and the University of New South Wales Human Research Ethics Committee.
Demographic and behavioural survey in YWHS-2
Structured questionnaires were administered in Khmer by native speakers to enrolled participants at a baseline visit and on a quarterly basis for one year. The survey, which took approximately 45 min to administer included up to 45 questions (depending on skip patterns) on demographics, employment, income, sexual behaviours, alcohol and drug use, perception of HIV risk, reproductive health, and STI/HIV prevention behaviours. Women were also queried at baseline regarding whether they had heard of or knew anything about HPV infection or vaccine, and answers were coded dichotomously (yes/no).
HPV information and education brief intervention
Following the baseline study visit, participants received a brief information and education intervention that was delivered in two sessions, both of which included: general information on HPV, instruction on modes of transmission, the relationship between HPV and cervical cancer and genital warts, and benefits and risks of the quadrivalent multi-dose HPV preventive vaccine, including its contraindications for women who were pregnant or had HIV. The first session was held one month prior to the first quarterly study visit (month two of the study): outreach workers invited participating women to attend a session at the community-based partner (CWDA) site. The second session was held at the clinic at the three-month visit, prior to data collection and vaccine administration. At both sessions, a pamphlet with the same information was also given to each participant. All sessions and information were provided by a trained outreach worker from CWDA in Khmer language.
Pre-vaccination knowledge and attitude survey
At the three-month study visit, participants completed a brief knowledge and attitude survey to assess knowledge of HPV infection resulting from the information and education, and to assess their willingness to receive the HPV vaccination. Portions of the survey were adapted from other studies which assessed HPV knowledge and attitudes towards vaccination.26,27 The survey assessed: (1) HPV and vaccine knowledge, (2) general attitudes on vaccination, (3) willingness to accept HPV vaccination, (4) reasons for accepting vaccination, and (5) reasons for declining vaccination. The reasons for accepting and declining vaccine were from a list and were not open-ended questions. Surveys were translated from and back-translated between English and Khmer for accuracy.
HPV vaccination
All women negative for HIV and not pregnant were offered the quadrivalent HPV vaccine via a schedule that followed the package insert instructions with three doses over six months (at month 0, 2, and 6). Those who accepted the offer received the first vaccination at that visit. HIV-positive individuals were excluded from vaccination (but not the education sessions), as the safety of the vaccine in HIV-positive individuals this population had not been determined at the time of this study. Pregnant women were also excluded from receiving vaccine, in accordance with the CDC Guidelines for Vaccinating Pregnant Women 24 and women receiving the vaccine were counselled to avoid pregnancy and provided with free condoms. Study outreach workers reminded participants to attend vaccination visits with verbal and written reminders and transportation was provided. HPV acceptance and immunization completion rates were tracked and recorded on paper and clinical report forms and then entered into the study database.
Measures
Outcome variables for the present analysis include: (1) HPV awareness, which was measured at baseline by the question: ‘Have you ever heard of HPV?’ Participants were classified as ‘aware’ if they indicated that they had heard of HPV, and ‘not aware’ if they had not heard of HPV; (2) results from the HPV knowledge and attitude survey including general HPV knowledge, vaccine, and willingness to receive HPV vaccine were tabulated; with the raw number of correct answers summed for each question, and knowledge was represented by the total number and percentage of women answering all questions correctly; (3) HPV immunization eligibility; and (4) HPV immunization series completion among those who were eligible.
Analyses
Descriptive statistics, including frequencies and measures of central tendency (medians and interquartile ranges [IQRs]), were used to describe the study population, and results of HPV knowledge and attitudes survey. We examined both HPV vaccine uptake and series completion by demographic characteristics. Factors associated with vaccine series completion were assessed using the Chi square test and multivariate logistic regression. Multivariate models were built using a backward stepwise elimination method, including variables hypothesized to be associated with the vaccine incompletion outcome, such as ATS use, variables significant at 0.20 in bivariate analyses, and known confounders, including those associated with ATS use, such as sex work venue. Variables were eliminated one by one in reverse order of significance until the model contained only sex work venue and those factors remaining significant at p ≤ 0.05. All analyses were performed using STATA (Version 12.1, College Station, TX).
Results
Study population
Characteristics of women participating in the YWHS-2 Study, eligible for and completing the three-dose vaccine series, and associations with vaccine series completion.

*p-value ≤ 0.05; **p-value ≤ 0.01.
¶Data are missing for two women.
ATS: amphetamine-type stimulant.
HPV awareness at baseline and three-month visits
HPV and vaccine knowledge among 191 FESW (following brief information and education intervention).

HPV vaccine eligibility, acceptance, and reasons for receiving vaccination
Reasons for HPV vaccine acceptance among 152 eligible FESW (following a brief information and education intervention).

HPV vaccine series completion
Out of the 149 women who received the first dose of the vaccine, 138 (92.6%) returned in two months and 11 (7.4%) women were lost to follow up (Figure 1). Of the 138, three women had become pregnant and were ineligible to continue the vaccine series. For the third and last vaccine administered at month six, 123 (91.1%) women of the 135 who had received the second vaccine returned, and 118 received the third and final dose. Five additional women had become pregnant during the interim period and were not eligible for the final vaccine visit. The overall vaccine series completion rate among vaccine initiates was 79.2%.
HPV vaccine completion.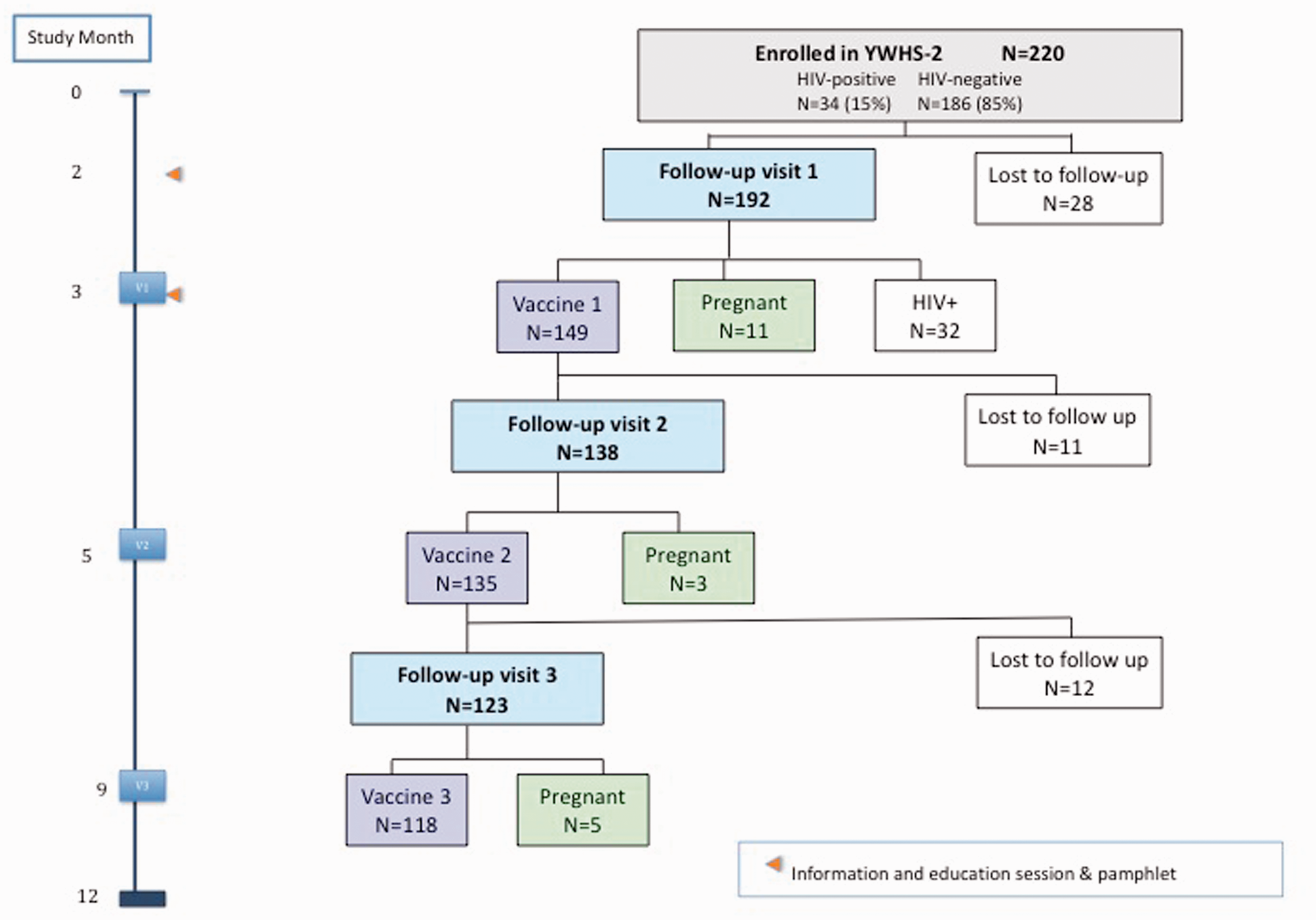
Women were still offered the subsequent vaccine dose if they returned after their scheduled visit date. The median number of days between the first and second dose of the vaccine was 57 days and 180 days between the first and the third dose. Overall, 15.4% of women were lost to follow up and did not complete vaccination. With the exception of age (median 26 versus 31.5 years) and time engaged in sex work (median 25 versus 7 months), there were no significant differences between the 192 retained and the 28 not retained, respectively. Overall, one in 20 women (5.4%) who started the series had to stop due to new pregnancy. Both recent and any use of ATS, reported by 27.3 and 37.3% of women, respectively, were significantly associated with incomplete vaccination in bivariate analyses, as was number of sexual partners in the past month (Table 1). In multivariate logistic regression a recent history ATS use, remained independently and significantly associated with incomplete vaccine series (AOR, 0.2; 95% CI, 0.08, 0.69; P < 0.01), after controlling for sexual risk exposures and confounders: number of sexual partners and employment venue (Table 1). Age did not affect the model and was removed so that the most parsimonious model is presented.
Discussion
In this study we found that HPV awareness was low in young FSWs, less than a quarter of whom had heard of HPV at study baseline. Following a brief information and education intervention, however, they demonstrated comprehensive understanding of HPV including mode of transmission, potential disease outcomes, risk and prevention approach, including vaccination. Among those who were eligible for vaccination, all elected to receive the HPV vaccine, and nearly 80% received all three doses during the six-month period, with no adverse events. However, a substantial proportion of women (over 20%) were ineligible for HPV vaccine as a result of pregnancy or HIV infection, and new pregnancies accounted for some further discontinued vaccines. Drug use, specifically ATS use, was a strong predictor of incomplete HPV immunization. We have previously published on the context and described consequences of ATS use among young women involved in the sex and entertainment industry in Cambodia. 28 ATS use is increasingly associated with adverse health outcomes including incident STI and HIV infection in young FSWs.24,25 Many women initiate ATS use to stimulate income generation, but consequently experience negative health effects, and in turn diminished capacity for income generation through dependence and/or physical degeneration. 28 Our results show that ATS use can also have negative effects on health-seeking behaviour potentially due to stigma, fear of law enforcement, or other psycho-social distress.
Few studies have assessed vaccine acceptance in FSWs, and this study adds important data to literature regarding high acceptance and measures of vaccine completion in this group of women. In Lima, Peru, researchers assessed HPV awareness and interest in receiving HPV vaccine in a similarly aged (18–29 years) group of FSWs. 26 Although less than half (44.2%) had heard of HPV, after receiving information regarding the infection and its association with cancer, almost all (97.5%) wanted to receive the vaccine. This group also demonstrated a 92% completion rate of the three-dose HPV vaccine in this population in a trial comparing two dosing schedules. 29 As in this study, FSWs in Thailand also demonstrated low knowledge levels regarding HPV despite the high rates of cervical cancer in the region. 30 Our finding that women can dramatically increase HPV and HPV vaccination knowledge levels through a simple information and education intervention is especially useful for health providers and programmes who want to provide vaccination programmes to high-risk women. Although we did not measure knowledge retention, HPV vaccination programmes may also result in increased knowledge and reduced sexual risk exposures among FSWs, as shown by Brown et al., in Peru. 30
Our study has several limitations. The modest sample size could have impacted power to detect effects from behaviours or exposures potentially associated with incomplete vaccination. The vaccine provided in the YWHS-2 was provided at no cost as part of the study and similar results may not be achieved in settings where women have to pay for the vaccine, as suggested by the fact that all eligible women cited free vaccine provision as a reason to accept. The research programme provided transportation, and the vaccine was given at the research clinic (which was co-located in the same building as an STI and family practice clinic) and did not involve local health care providers, factors that were not examined as part of vaccine completion. Study participants were recruited to the YWHS-2 via convenience sampling methods and results may not be generalizable to all FSWs in Cambodia. Since labour laws in Cambodia restrict employment to those 18 and older, this sample may be older than seen in other groups of sex workers. Almost one in seven (15.4%) women who initiated HPV vaccine were lost to follow up, which could have biased the associations detected (either over- or under-estimating) with vaccine completion.
Despite these limitations, this study demonstrated the feasibility and effectiveness of delivering both a brief educational intervention, and a multi-dose vaccine to FSWs in a developing country setting. Our finding that many participants accepted the vaccination because of advice from a doctor or nurse contributes to the existing literature highlighting the important role health care providers play in vaccine uptake. 5 In general, enhancing education of both the public and of providers is critical to increasing vaccination rates. Since all eligible women accepted vaccination, it was not possible to assess whether the educational intervention enhanced vaccine uptake. However, factors that were not evaluated and which may have impacted vaccine acceptance and uptake may in fact have been related to the research study itself, including the relationship women had with the study health care providers, and the logistical support provided to women to attend study visits. Future studies, especially implementation science studies, should consider evaluating logistical constraints that FESW experience in accessing health care, including transportation and clinic access.
For women in the sex and entertainment industry, likelihood of exposure to HPV is high. Although it is ideal to vaccinate individuals prior to sexual debut, there is growing evidence that the HPV vaccine is effective in women regardless of previous exposure to HPV.17,18 A modelling study suggests that including women who have exposure to HPV can significantly and positively impact the cost effectiveness of vaccination efforts and that adult vaccination strategies should be reassessed. 31 At the time of this study, the immunogenicity and safety of the HPV vaccine in people with HIV infection were unknown. More recent studies have shown that the vaccine is immunogenic, safe, and well tolerated in women with HIV, who can therefore be included in programmes for vaccination. 32
In conclusion, Cambodian FSWs, a population at high risk for HPV infection, responded positively to a brief information and education intervention, demonstrating good knowledge and high vaccine uptake. ATS use and high-risk sex both had especially negative associations with vaccine completion. As well, women in brothel-based or freelance sex work were more likely to complete the vaccine series. This may be a result of more intensive health messaging directed towards women in these venues in association with HIV prevention. While this study informs future vaccine implementation programmes, more tools are needed to identify methods to not only curb and prevent ATS use, but also minimize pregnancy, loss to follow-up, and associated vaccine non-completion for this group of women. Programmes that target women at high sexual risk should consider ways to target women in multiple venues, as well as the potential positive of strong community involvement with respect to outreach and health workers. Incorporating reproductive health messaging in HPV vaccine education sessions as well as providing alternative prevention methods (to condoms) should be explored in future implementation science research. Implementation science research should be conducted to assess other operational factors as well such as transportation and clinic location. The efficacy of modest incentives could be studied, as these have been shown to increase vaccine completion in other high-risk groups, such as people who use drugs.33,34 Given the strong associations found between ATS use and incomplete vaccination, interventions to reduce drug use should also be explored in this population. Prioritizing HPV vaccination in high-risk women in Cambodia may also offer new opportunities to advance prevention for other STIs and HIV, in addition to reducing HPV-associated morbidity and mortality.
Footnotes
Acknowledgements
The authors would like to acknowledge the coordinated efforts and dedication of the research teams at the National Center for HIV/AIDS, Dermatology, and STDs and the Cambodian Women’s Development Agency. We thank Merck Medical Projects Team for making the HPV vaccine available. We are indebted to all the Cambodian women who agreed to participate in this study and grateful for the privilege of working with them. We acknowledge the donation of HPV vaccine to the study by Merck Medical Projects Team Australia (
Declaration of Conflicting Interests
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, nor the Australian Government. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Young Women’s Health Study was supported by an award R01NR010995 from the U.S. National Institutes of Health, National Institute of Nursing Research. M-C Couture was also supported by the Canadian Institutes of Health Research (postdoctoral fellowship award). Professors Lisa Maher and John Kaldor are supported by the Australian National Health and Medical Research Council (NHMRC) Research Fellowships. The Kirby Institute is affiliated with the Faculty of Medicine, University of New South Wales and is funded by the Australian Government Department of Health and Ageing. Professor Gandhi is supported by the UCSF Global Health Sciences Masters' program.