
Abstract
Summary
Given that syphilis is associated with HIV infection among people who inject drugs (PWID), we examined syphilis incidence among PWID in Tijuana, Mexico. From 2006 to 2007, 940 PWID (142 women and 798 men) were recruited via respondent-driven sampling and followed for 18 months. At semi-annual visits, participants were tested for syphilis and completed surveys, which collected information on socio-demographics, sexual behaviours, substance use and injection behaviours. Poisson regression was used to estimate syphilis incidence rates (IRs), incidence rate ratios (IRRs) and 95% confidence intervals (CIs). Twenty-one participants acquired syphilis during follow-up (IR = 1.57 per 100 person-years, 95% CI: 1.02–2.41). In a multivariate analysis, syphilis incidence was higher among women (IRR = 3.90, 95% CI: 1.37–11.09), HIV-positive participants (IRR = 4.60, 95% CI: 1.58–13.39) and those who reported ever exchanging sex for drugs, money, or other goods (IRR = 2.74, 95% CI: 0.97–7.76), while syphilis incidence was lower among those living in Tijuana for a longer duration (IRR = 0.95 per year, 95% CI: 0.91–1.00) and those reporting at least daily injection drug use (past 6 months) (IRR = 0.22, 95% CI: 0.09–0.54). Our findings suggest interventions that address the destabilising conditions associated with migration and integrate sexual and drug-related risk reduction strategies may help reduce syphilis incidence among PWID along the Mexico–US border.
Keywords
Introduction
Although HIV acquisition among people who inject drugs (PWID) has historically been attributed to parenteral exposures resulting from risky injection practices, 1 sexual transmission accounts for a substantial proportion of HIV infections within this population. 2 Previous research conducted among PWID has also documented elevated rates of syphilis, 3 which facilitates HIV transmission and enhances susceptibility to HIV during sexual intercourse. 4 Interventions that promote testing for sexually transmitted infections (STIs), including syphilis, and address both sexual and drug-related risk behaviours are needed to reduce HIV transmission among PWID.
Tijuana, Mexico borders San Diego, California, and is positioned on a major drug trafficking route linking the United States (US) with South and Central America, which has contributed to an epidemic of injection drug use in the city. 5 Although HIV prevalence remains under 5% among male PWID in Tijuana, the estimated prevalence among female PWID is higher at 10%. 6 Similarly, a higher prevalence of active syphilis (RPR titres ≥1:8) has been reported for female PWID (16%) than for male PWID (6%) in Tijuana, and active syphilis has also been independently associated with HIV infection within this population. 6 Among female sex workers (FSWs) who inject drugs surveyed in the Mexico–US border region between 2004 and 2005, the estimated prevalence of active syphilis was 23%. 7 In another study conducted among FSWs in the region, active syphilis was associated with injecting drugs, using illicit drugs before/during sex and having clients from the US. 8 Yet little is known about predictors of syphilis incidence among PWID in this region. To inform the development of syphilis control programmes for PWID, we estimated the incidence and identified predictors of syphilis among PWID in Tijuana, Mexico.
Methods
Study design
From 2006 to 2007, 1056 PWID in Tijuana were recruited via respondent-driven sampling (RDS) 9 to participate in a prospective (18 months) study of HIV, syphilis and tuberculosis. As previously described,10,11 diverse seeds (n = 32) (heterogeneous with respect to age, gender, and geographic location) were selected and given uniquely-coded coupons to refer their peers to the study. Eligible recruits were then given coupons to recruit their peers in subsequent recruitment waves. Men were given three coupons while women were given six to twelve coupons in an effort to recruit more women. Of the 32 seeds, 24 successfully recruited other PWID eligible for study participation. On average, there were 6.8 recruitment waves (min = 1; max = 17) across the 460 recruitment chains. Eligible individuals were ≥18 years old; reported injection drug use within the past month (verified by inspection of track marks); spoke Spanish or English; and had no imminent plans to move to another city. All participants provided informed consent and institutional review boards at the University of California, San Diego and Tijuana General Hospital approved all study protocols.
Study procedures
At semi-annual visits (four visits total), participants completed interviewer-administered questionnaires that collected information on socio-demographics, mobility, sexual behaviours, substance use and injection behaviours. Participants provided blood samples for HIV and syphilis testing at each visit. Positive ‘Determine’ rapid HIV antibody tests (Abbott Pharmaceuticals, Boston, MA) were confirmed via Western blot. Syphilis infection was identified via rapid plasma reagin (RPR) testing (Macro-Vue; Becton, Dickinson and Company, Cockeysville, MD) of participants’ sera and confirmed using the Treponema pallidum particle agglutination assay (TPPA; Fujirebio, Wilmington, DE). All specimen testing was conducted at the San Diego County Health Department. HIV or syphilis positive participants were referred to municipal clinics for free care and treatment.
Incident syphilis
Baseline RPR and TPPA results and RPR titres were considered in defining incident syphilis. Among participants without syphilis at baseline (i.e. RPR and TPPA negative or RPR and TPPA positive with RPR titres <1:8), incident syphilis cases were RPR and TPPA positive with RPR titres ≥1:8 at a follow-up visit. Among participants with syphilis at baseline (i.e. RPR and TPPA positive with RPR titres ≥1:8), incident syphilis cases self-reported treatment and had evidence of a four-fold decrease in titres at a follow-up visit followed by a four-fold increase in titres at a subsequent follow-up visit. Of the 1056 participants, 940 had data available at baseline and ≥1 follow-up visit to determine their incident syphilis status and were eligible for inclusion in our analysis.
Statistical analysis
For our analysis, participants were followed from enrolment to incident syphilis, loss to follow-up, or the end of the study period, whichever came first. Syphilis incidence was calculated by dividing the number of incident cases by the observed number of person-years. The date of syphilis infection was defined as the date of the visit at which the individual tested syphilis positive. Poisson regression was used to estimate syphilis incidence per 100 person-years. In an exploratory analysis, Poisson regression was used to identify predictors of incident syphilis. Predictors of interest included: socio-demographics, mobility, sexual behaviours, substance use and injection behaviours. To minimise temporal ambiguity, we examined predictors measured at the second visit. Significant (α = 0.05) predictors in unadjusted analyses were examined for collinearity and considered for inclusion in our final adjusted model. If <5 incident syphilis cases were observed for a single level of a significant predictor (i.e. usual injection location), that predictor was excluded from our final model to minimise the potential for biased estimates due to small cell sizes. Because RDS-weighted and unweighted estimates were similar only unweighted results are presented. 12
Results
Characteristics of PWID in Tijuana, Mexico.a
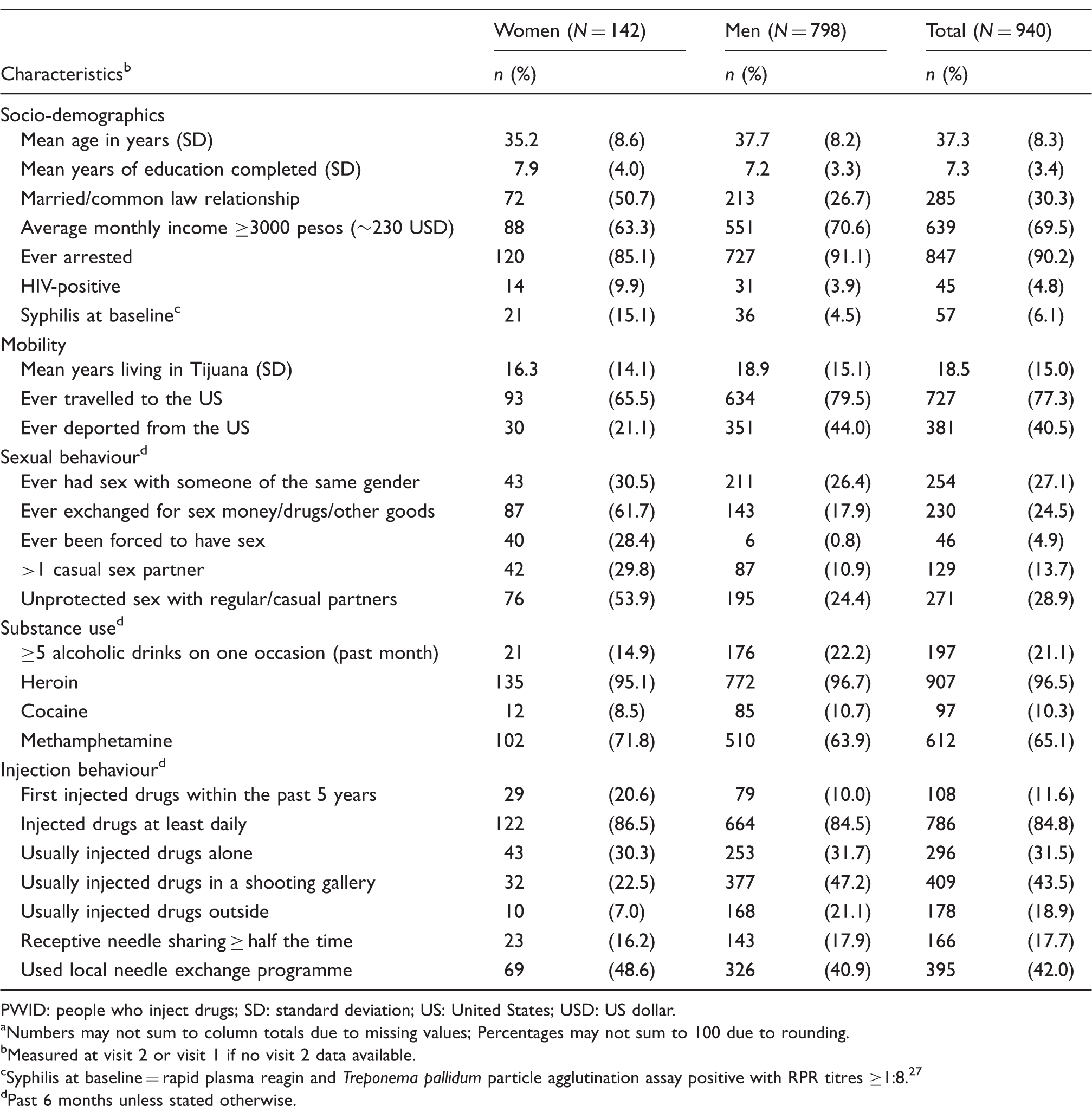
PWID: people who inject drugs; SD: standard deviation; US: United States; USD: US dollar.
Numbers may not sum to column totals due to missing values; Percentages may not sum to 100 due to rounding.
Measured at visit 2 or visit 1 if no visit 2 data available.
Syphilis at baseline = rapid plasma reagin and Treponema pallidum particle agglutination assay positive with RPR titres ≥1:8.27
Past 6 months unless stated otherwise.
Incidence rate ratios for syphilis among PWID in Tijuana, Mexico.
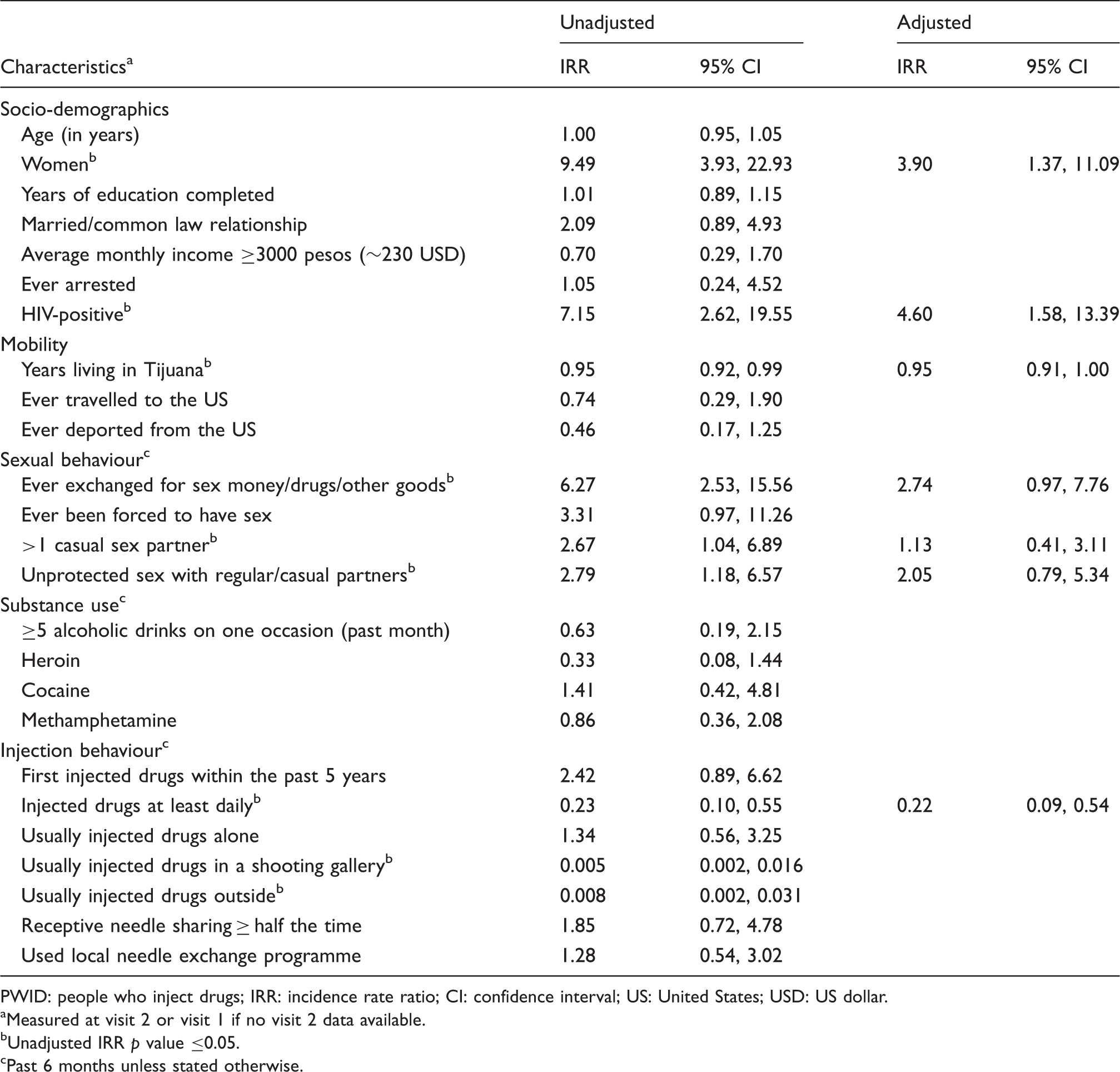
PWID: people who inject drugs; IRR: incidence rate ratio; CI: confidence interval; US: United States; USD: US dollar.
Measured at visit 2 or visit 1 if no visit 2 data available.
Unadjusted IRR p value ≤0.05.
Past 6 months unless stated otherwise.
Discussion
In this cohort of PWID followed for 18 months in Tijuana, Mexico, the overall incidence of syphilis was 1.6 per 100 person-years – slightly lower than that observed in a cohort of PWID in Los Angeles County (2.6 per 100 person-years, 95% CI: 1.9–3.2). 13 However, the rate of syphilis infection was nearly four times higher among women, which is consistent with reports from previous studies conducted among PWID reporting both a higher prevalence 3 and incidence13,14 of syphilis among women. Previous research has also documented an association between syphilis and trading sex or being paid for sex among PWID,13,14 particularly female PWID, 15 which may explain much of the observed association between gender and incident syphilis. In Mexico–US border cities, socially-marginalised women who inject drugs have limited employment opportunities and often engage in sex work to support themselves and their addictions. 16 Although we were unable to stratify by gender, we observed an association between incident syphilis and ever exchanging sex for drugs, money, or other goods, which was reported by a greater proportion of women than men (62% vs. 18%). Thus, our findings underscore a need for gender-specific risk reduction strategies and suggest interventions designed to increase condom use with commercial sex partners may help reduce the risk of syphilis among female PWID.
Participants living in Tijuana for a longer duration were less likely to be diagnosed with syphilis during follow-up. This finding is consistent with the previously reported association between recent migration to Tijuana and HIV infection within our sample.6,10 Migrant populations are highly prevalent in the Mexico–US border region as a result of both cross-border mobility between Mexico and the US and migration from within Mexico in search of economic opportunities in the region. 17 Numerous studies have documented a relationship between migration and increased sexual risk behaviours and risky injection practices,18–20 which may be the result of changing social networks or an enhanced sense of anonymity in the new environment. 21 However, migrants may also be driven to engage in high-risk behaviours (e.g. substance use, sex work or sex with commercial sex workers) as a means of coping with the social and economic stressors (e.g. homelessness, difficulty securing employment, and family separation) associated with migration. 22 Interventions targeting migrant PWID in the Mexico–US border region that minimise the destabilising conditions associated with migration, and integrate strategies to reduce both sexual and drug-related risk behaviours may help control the spread of syphilis within this population.
Syphilis incidence was also lower among participants reporting daily injection drug use. In a study of male PWID in Vietnam, non-daily injection drug use was associated with chlamydial infection. 23 During in-depth interviews, these male PWID expressed decreased sexual interest or desire with increasing injection frequency. 23 Thus, decreased sexual activity may have similarly reduced syphilis exposure among PWID who reported daily injection drug use in our sample.
Although not statistically significant, syphilis incidence was higher among participants reporting elevated risk behaviours, such as having multiple casual sex partners, engaging in unprotected sexual intercourse and practicing receptive needle sharing at least half the time in the past 6 months. Moreover, HIV-positive participants were also more likely to be diagnosed with syphilis during follow-up. While many HIV-positive individuals adopt lower risk behaviours following diagnosis, 24 others continue to practice high-risk behaviours,25,26 which may have been the case within our sample and explain the observed relationship between HIV and incident syphilis. Given that nearly half of our sample reported obtaining syringes from the local needle exchange program (past 6 months), expanding such programs and incorporating risk reduction counselling, point-of-care STI/HIV testing, and on-site STI treatment may help reduce STI/HIV incidence among PWID in the Mexico–US border region.
Our study has several limitations. First, given the study’s recruitment strategy, our findings may not be generalisable to all PWID in Tijuana. Second, although retention was high (81%), participants with complete follow-up differed from those with incomplete follow-up with respect to their baseline HIV status and duration of residence in Tijuana, which may have biased our estimate of incident syphilis downwards. Third, our definition of incident syphilis is limited to diagnosis as part of the study. Although unlikely, participants could have been diagnosed and treated for syphilis between study visits, which would have resulted in an underestimate of incidence. Fourth, data were collected via face-to-face interviews, thus participants may have under-reported sensitive information on substance use and sexual behaviours. However, study staff made every effort to build rapport with participants and earn their trust to minimise social desirability bias. Fifth, the low overall incidence of syphilis within our sample resulted in large CIs and may have limited our power to detect predictors of incident syphilis. Finally, although enhanced efforts were employed to recruit female PWID, the small sample of women included in our study did not enable stratification by gender.
Despite these limitations, our findings underscore the need for syphilis control programs among PWID along the Mexico–US border. While additional research powered to investigate syphilis incidence among both male and female PWID is needed to inform the development of effective interventions for this population, our findings suggest interventions that address the destabilising conditions associated with migration and integrate sexual and drug-related risk reduction strategies may help reduce syphilis incidence among PWID in the Mexico–US border region.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (grant numbers R37-DA019829 and T32-DA023356).