
Abstract
The objective of this study was to investigate the prevalence and influencing factors of HIV infection among men who have sex with men (MSM) in Hefei, China. A total of 578 MSM were recruited, with a mean age of 28.13 ± 6.91; 70.7% were under 30. The awareness rate was 95.4% (560/587) in the cross-sectional study. Of all the respondents, 73 (12.44%) were seropositive for HIV and 56 (9.54%) for syphilis. Multivariate analysis showed that self-reported sexually transmitted infections (STIs) (AOR = 8.02, 95% CI: 2.58–24.98, P < 0.001), received HIV testing in the past year (AOR = 0.33, 95% CI: 0.19–0.60, P < 0.001) and syphilis (AOR = 3.40, 95% CI: 1.69– 6.85, P = 0.001) were independently associated with HIV infection. It is necessary for post-test counselling to address risk among those who engage in sexual risk behaviours. More efforts are needed to enhance HIV/STI testing and treatment services in China.
Keywords
Introduction
Sex, especially male-to-male sex, has been an important route of HIV spread since HIV/AIDS was first identified 32 years ago. UNAIDS pointed out that men who have sex with men (MSM) became the prominent contributing factor to new HIV infection in the Asia-Pacific region. 1 Prevalence of HIV among MSM ranged from 7.5% to 30.8% in India, 2 Thailand, 3 Cambodia and Indonesia. 4 In China, a total number of 48,000 people were newly diagnosed with HIV infection in 2011, and 29.4% were infected via homosexual transmission. 5 From 2009 to 2011, several meta-analyses of HIV among Chinese MSM reported pooled HIV prevalence as 2.5%–15.8%.6–9
A growing number of studies suggest that not only individual factors10–12 (biologic, demographic and risk behaviours), but also social factors13–15 (cultural context, social networks, neighborhood effects and social capital) and structural factors 16 (structural violence and discrimination, legal structures, demographic change, the policy environment and war and militarisation) influence the risk of HIV acquisition, disease progression, distribution of HIV/AIDS in population subgroups and HIV transmission dynamics. Hefei, the capital city of Anhui Province, links the centre and the east of China. The last century has witnessed a number of ‘AIDS villages’ in rural areas of this province because of the illegal practice of selling blood. It is close to Nanjing and Shanghai, with a high prevalence of HIV among MSM. Hefei lags behind other municipalities both economically and in terms of social development, and has a large ‘floating’ population.17,18 As we know, a high migration rate is associated with higher risk of HIV infection in MSM. 15 Therefore, risk factors associated with HIV infection are of great importance in HIV prevention in the floating population.
Our understanding of multi-level factors has been reported elsewhere.19,20 However, studies on such factors among MSM in Hefei are lacking. In the present study, we investigated the factors associated with HIV infection among MSM in Hefei, in order to provide a reliable estimation of HIV prevalence and related influencing factors in this city.
Methods
Sampling methods and procedures
From August 2013 to May 2014, MSM were recruited for a cross-sectional HIV and behavioural survey in Hefei, Anhui, China. Before formal investigation, all interviewers were trained to understand the purpose, meaning of the investigation and the contents of the questionnaire. The survey was advertised on the internet through the official website of Disease Control and Prevention (CDC) of Hefei and QQ (Tencent QQ, a Chinese instant messaging program). Participants were recruited through snowball sampling. Inclusion criteria of the study were MSM, having male-to-male sexual risk behaviours in the past and physically able and willing to participate in the study. Participants met with the trained researcher at various venues including Luyang District CDC, Hefei CDC, MSM bars and MSM saunas. All participants were self-administered in private rooms. To protect participants’ information, actual names were not required, so nicknames were permitted. Trained interviewers gave a brief introduction to the interview. After obtaining their permission to start the interview, participants signed informed consents and filled in the questionnaires. In addition, blood samples were collected for HIV/syphilis testing and testing results were shared with participants. All participants received 50 Yuan (equivalent to about 8.05 USD) after they completed the whole interview.
The study protocol and procedures were reviewed and approved by the medical ethics committee of Anhui Medical University and complied with the principles outlined in the Helsinki Declaration.
Measures
The content of structured questionnaire included demographical characteristics (i.e. age, marital status, registered residence, ethnicity, education and time at current address), knowledge of HIV/AIDS, homosexual behaviours (having anal sex with men in the past six months, number of anal sex contacts with a man in the last week, condom use at last anal sex, frequency of condom use in the past six months, having commercial sex with men and frequency of condom use in the past six months and condom use for the last commercial sex with a man), heterosexual contacts (having sex in the past six months, frequency of condom use in the past six months, condom use in the latest sex), drug use (ever used drugs, injected drugs and ever shared needles for drug use with someone else), history of sexually transmitted infections (STIs), having received HIV test and the testing results for HIV and syphilis.
Laboratory tests
To determine HIV infection status, blood specimens were first detected by enzyme-linked immunoassay (ELISA) (Shanghai Kehua Bio-Engineering Co. Ltd., China) and positive results were confirmed by HIV1/2 Western Blot analysis (MP Biomedical Co. Ltd., Singapore). Syphilis antibodies were assessed by ELISA (Beijing Jinhao Biologic Production Co., China).
Statistical analysis
Questionnaire data were analysed with Epi Data version 3.0 (Epi Data Association, Odense, Denmark) and SPSS (PAWS statistics 18.0). Risk factors that were significant at P < 0.1 in univariate logistic regression analysis were entered into the stepwise logistic analysis model. Multivariate logistic regression analysis was used for the significant variables in the bivariate analysis and it was applied to calculate odds ratios (ORs) for risk factors related to HIV results. Significance was set at P < 0.05, and ORs were reported with 95% confidence intervals (CIs).
Results
Demographic characteristics
Demographic characteristics of MSM study participants, Hefei, 2013–2014.
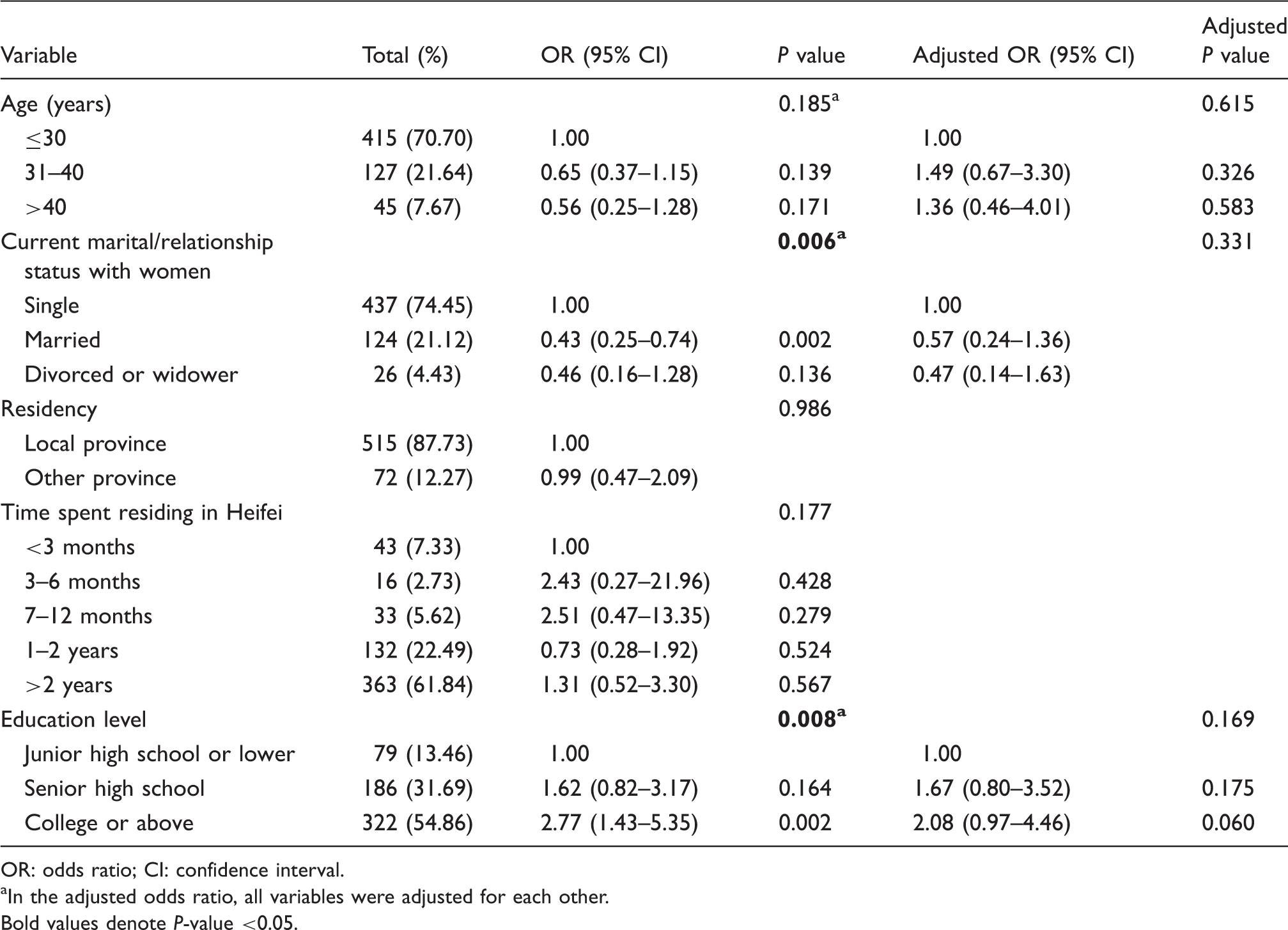
OR: odds ratio; CI: confidence interval.
In the adjusted odds ratio, all variables were adjusted for each other.
Bold values denote P-value <0.05.
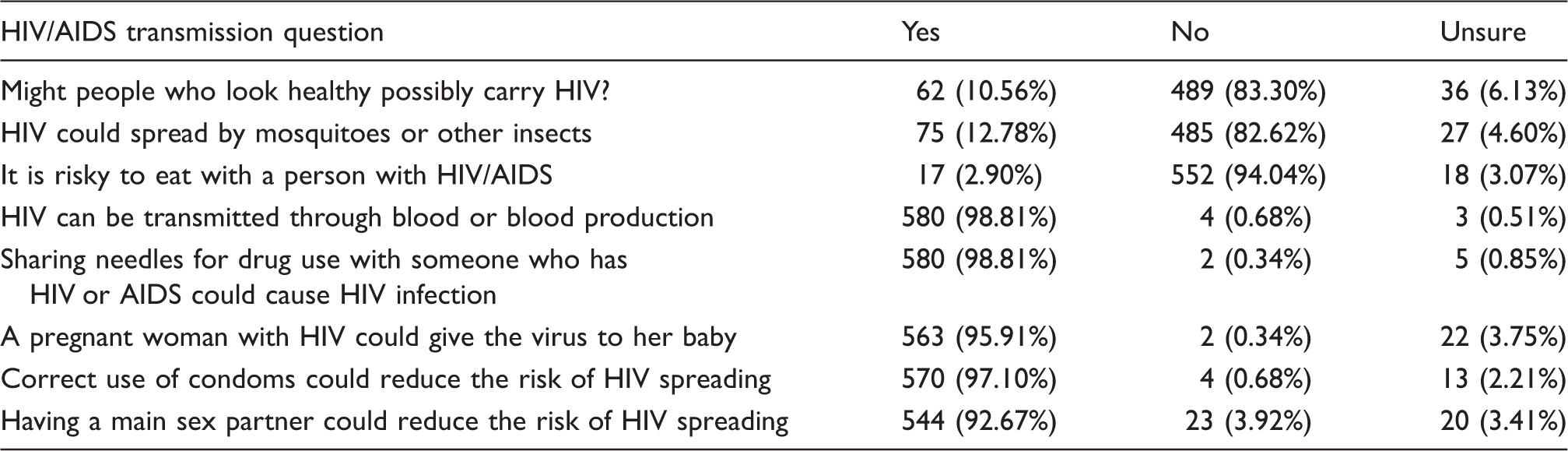
HIV/AIDS knowledge and awareness rate
The HIV/AIDS-related knowledge of MSM, Hefei, 2013–2014.
Sexual behaviours, condom use and substance use
Overall, while 91.99% participants reported that they had had the experience of having anal sex with a man, only 153 (28.33%) had always used condoms during anal sex with a man in the last six months. Among the respondents, 1.67% accepted commercial anal sex with a man in the last six months. Regarding female partners, 110 (18.74%) of MSM had had sex with a woman in the past six months. Drug use was relatively rare. The number of MSM who reported drug use throughout their lifetime was seven (1.19%). No MSM injected drugs or shared needles with others (Table 2).
Self-reported STIs, HIV testing and syphilis status
Sexual behaviours associated with HIV infection among MSM study participants, Hefei, 2013–2014.

OR: odds ratio; CI: confidence interval; STI: sexually transmitted infection.
In the adjusted odds ratio, all variable were adjusted for each other.
Bold values denote P-value <0.05.
Multivariate logistic regression analysis of factors associated with HIV infection
Results of multivariate analysis showed that MSM who had STIs were 8.02 times more likely to be HIV-positive (AOR = 8.02, 95% CI: 2.25–24.98, P < 0.001). Respondents who received HIV testing in the past year were at lower risk of HIV infection (AOR = 0.33, 95% CI: 0.19–0.60, P < 0.001). The risk of participants who had syphilis was 3.40 times higher than others to get HIV infection (AOR = 3.40, 95% CI: 1.69–6.85, P = 0.001) (Table 3).
Discussion
This study revealed an estimated prevalence of HIV among the 587 MSM as 12.44% in Hefei, which was generally consistent with the study of Li et al. 7 The Ministry of Health of the People’s Republic of China estimated that HIV prevalence among China’s MSM was approximately 6.3% in 2011 21 . Several previous studies on HIV among MSM in China reported a pooled HIV prevalence of 2.5% in 2001–2008, 6 5.3% in 2007–20098–10 and 4.9% in 2012–2013. 22 It suggests that HIV prevalence in Hefei is higher than the average level of China. Its reason is not clear and further investigation is expected.
Our data also revealed that 54.86% had a college or above level of education. HIV/AIDS knowledge and awareness rate was 95.40%, indicating good HIV/AIDS knowledge awareness. But high-risk behaviours were common among these participants; only 57.78% of the participants used a condom in the last sex with male, and the proportion of consistent condom use was only 28.33% in the past six months. 18.74% of the participants had had sex with a woman in the past six months, which is lower than the neighbouring province of Anhui (Henan). 23 The percentage of condom use at last sex with a woman was lower than male-to-male sex. During the past six months, 25.45% of the participants had never used a condom and 58.18% of the respondents sometimes used a condom in heterosexual activities. The age of respondents ranged from 17 to 58; 70.70% of the respondents were below 30 years old. The upper boundary of age is lower than other studies in different areas, such as, Shenyang, Fushun, Anshan and Henan.23,24 74.45% of MSM were single, which is higher than Shenzhen, Henan and cities in northeast China23–25 and the proportion of MSM who are single is as high as 82% in Chongqing and Guangdong26–28. We speculate that the younger age and single status might have an impact on increasing sexual risk behaviours. We recommend the use of behavioural prevention interventions to reduce the risk behaviours among MSM. Suggested strategies include HIV testing and linkage to care, access to condoms and sterile syringes, prevention programmes for people living with HIV and their partners, prevention programmes on HIV/AIDS-related knowledge for MSM, substance abuse treatment, and screening and treatment for other STIs.
Deuba et al. 29 reported that the risk of HIV infection among MSM who had a history of STI symptoms was three times higher than those who had no history of STI symptoms. Our data showed that the risk of HIV infection was 8.02 times higher. In addition, another study documented that MSM with a history of STIs were more likely to be infected with HIV in Jamaica. 30 As risk behaviours for STIs are similar to those of HIV, it is likely that MSM are still engaging in high-risk sexual behaviours. 31 Mirzazadeh et al. showed that more than one-third of MSM had STIs during the past 12 months and only a few sought out appropriate treatment 32 ; 8.2% participants reported at least one STI in the last 12 months in New Zealand. 33 Early diagnosis and effective STI treatment is an essential component of HIV prevention because STIs facilitate HIV transmission and this is consistent with Boozer and Philipson 34 and Galvin and Cohen’s 35 studies. As the risk of acquiring and transmitting HIV is amplified in the presence of STIs, it is necessary for post-test counselling to address risk among those who are chronically engaging in sexual risk behaviours.36,37
In this study, HIV test was associated with a lower risk of HIV infection (P < 0.001, AOR = 0.33, 95% CI: 0.19–0.60). Balaji et al. 38 found that, compared to young MSM who had had their recent HIV testing in the last 12 months, those who had had their recent HIV testing more than 12 months ago were more likely to be infected with HIV. In other words, HIV testing in the past year significantly decreased the risk of HIV infection. However, according to this study, 50.6% of the respondents did not receive HIV testing in the last 12 months. Moreover, HIV testing is a necessary first step in linking MSM to HIV prevention in the interests of their own health. 39 This suggests that HIV testing for MSM needs to be expanded. 40 The existing ways to make HIV testing more accessible include methods such as, support from HIV/AIDS outreach volunteers, voluntary counselling and testing (VCT) services from district hospitals, local health care facilities and VCT communities, carrying out all kinds of sexual health and AIDS education, and so on.
Our study indicated that MSM who had syphilis were 3.40 times more likely than those without syphilis to test positive for HIV. Several studies also demonstrated the connection between syphilis and HIV infection23,41–46 and suggested that syphilis could increase the sexual transmission efficiency of HIV. Several plausible biologic mechanisms may explain how syphilis (STIs) increases the risk of HIV transmission. Genital ulcer disease and inflammatory STIs may facilitate HIV infection through both mechanical and immune-mediated mechanisms and both genital ulcer disease and inflammatory STIs increase shedding of HIV from genital ulcers, semen and genital secretions. 47 So we speculate that syphilis had an impact in facilitating HIV infection in Hefei. It is effective to decrease the risk of HIV transmission by increasing public health efforts and treatment in this area.
However, several limitations in this study should be acknowledged. First, all of our results are based on self-reported data, which may be underestimated because of selective suppression or revealing of information. Second, this is a cross-sectional study, so it has its own shortcoming of missing causality between risk factors and HIV infection.
Conclusion
A high-impact prevention that uses a combination of scientifically proven, cost-effective and scalable interventions targeted to the right populations in the right geographic areas, this approach promises to greatly increase the impact of HIV prevention efforts. 48 Given the complexity of factors associated with HIV infection among MSM in Hefei, the use of high-impact prevention holds promise as a way to implement a multifaceted approach that expands HIV testing, and prevention and treatment services for STIs. We recommend an increase in efforts to make HIV/syphilis testing opportunities more accessible so that MSM can learn their HIV infection status and access appropriate care and prevention services.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was partly supported by National Major Scientific and Technological Special Project during the Twelfth Five-year Plan Period (2012ZX10001-007-006).