
Abstract
Summary
Raltegravir is one of the standard antiretroviral therapy (ART) options in treatment-experienced and -naïve patients. However, efficacy data from clinical practice are scarce. Therefore, the efficacy of raltegravir-containing ART in clinical practice was investigated retrospectively. In all, 295 treatment-naïve and -experienced patients were analysed using two different cut-offs for virological failure (200 or 50 copies/ml). The response at week 24 and onwards was evaluated as a ‘time to loss of virological response’ analysis and estimated as a survival function. Additionally, dual therapy regimens (raltegravir plus boosted protease inhibitor) were compared to standard combinations in experienced patients performing a snapshot analysis at weeks 24 and 48, as well as a time to loss of virological response analysis. A total of 86.2% of the 64 treatment-naïve patients maintained virological suppression using a cut-off of 200 copies/ml (c/ml), while 67.7% maintained virological suppression with a 50 copies/ml cut-off from week 24 until the end of observation. Among the 231 treatment-experienced patients, 84.8% maintained virological suppression from week 24 onwards using a cut-off of 200 copies/ml; and 71.0% using 50 copies/ml, respectively. In the subgroup snapshot analysis at week 24, 98.3% (86.7% using a cut-off of 50 copies/ml) and at week 48, 93.3% (80.0%) of patients responded to dual therapy. Patients who were receiving a standard background therapy responded in 88.3% (81.3%) at week 24 and in 86.0% (80.7%) at week 48. Differences were not significant. This study shows again the overall long-term efficacy of raltegravir-based ART and furthermore gives reference for a comparable efficacy of dual and standard nucleos(t)ide reverse transcriptase inhibitor–backbone regimens in experienced patients on raltegravir over a period of 48 weeks in a real-life cohort where patients with severe comorbidities were included.
Keywords
Background
The continuous development of new antiretroviral agents is indispensable due to the constant selection of resistant variants of the human immunodeficiency virus (HIV). Several classes of antiretroviral agents are available; one of the youngest among them being inhibitors of the viral integrase. Raltegravir (RAL) has been the first integrase strand-transfer inhibitor (INSTI) to be licensed for the therapy of treatment-experienced HIV-infected patients by the Food and Drug Administration (FDA) in 2007. The BENCHMRK-registration trials showed superiority in virological suppression for raltegravir plus optimised background therapy (OBT) in patients with triple-class drug resistance compared to OBT alone.1,2 This was even the case in patients with baseline characteristics of high HIV-1 RNA levels and low CD4 cell counts. 3 Similar findings were shown by Grinsztejn et al. 4 In treatment-naïve patients non-inferiority of a RAL-based combination treatment to an efavirenz-based combination treatment was shown in the STARTMRK study5–9 and by Markowitz et al. 10 These studies showed promising data on the efficacy of a RAL-based antiretroviral combination therapy, although for patients with stable virological suppression switching from lopinavir/ritonavir to RAL non-inferiority was not achieved (SWITCHMRK study). 11
In clinical practice, however, comorbidities and other interfering diseases, as well as issues of non-compliance and maladherence to antiretroviral therapy (ART), are also important factors leading to failure of ART, but are usually not displayed in prospective studies because of strict exclusion criteria. Gras et al. 12 gave evidence for the correlation of adherence to RAL therapy and virological control. Therefore, it would be interesting to see how clinical study data translates into practical therapy. Unfortunately, very few data gained retrospectively and directly from clinical practice are available. 13 Thus, one aim of this study was to investigate, from a retrospective view, long-term efficacy of different RAL-based antiretroviral therapies of both treatment-experienced and antiretroviral-naïve patients in clinical practice. Additionally, we intended to look at the virological efficacy of different RAL-containing regimens in the group of ART-experienced patients. There are a number of patients in our cohort who are, due to several clinical reasons such as toxicity of other agents or virological resistance/failure, treated with a dual therapy of RAL plus a boosted protease inhibitor (PI). Hence, another aim was to compare the virological efficacy of such a dual therapy with triple therapy regimens, mainly consisting of RAL plus two nucleos(t)ide reverse transcriptase inhibitors (NRTIs).
Patients and methods
We conducted a monocentric retrospective cohort analysis. The data were taken from the patient database of the HIV Outpatient Department of the Frankfurt University Hospital. The database contains all HIV-positive patients being treated in the department. Informed consent was obtained for every patient. The data were completed with information from the individual patient’s file. Patients were eligible to be enrolled in the study if they have received RAL as part of an ART regimen between October 2007 (approval of raltegravir) and October 2012. Patients were excluded from the study if there were less than two clinical visits. Additionally patients who had mistaken database entries were excluded.
All laboratory investigations were part of the clinical routine. All patients were treated in accordance with the Declaration of Helsinki and national and institutional standards.
The background therapy (BT) was categorised in: RAL plus boosted PI (‘dual therapy’), RAL plus two NRTIs, RAL plus boosted PI plus non-nucleoside reverse transcriptase inhibitors (NNRTI, ‘TRIO’), NRTI plus boosted PI and boosted PI plus T20.
Measurement of HIV-RNA levels and resistance analyses were performed using the COBAS AMPLICOR HIV-1 MONITOR Test, version 1.5, Roche Diagnostics (Pleasanton, California). The lower limit of amplification and detection was at 20 copies/ml.
In order to evaluate virological response to RAL-containing ART we performed a ‘time to loss of virological response’ (TLOVR) analysis. Virological response was evaluated at week 24 and onwards. It was defined in two different ways: a decrease in the HIV-RNA level to less than either 200 or 50 copies/ml at week 24 and onwards (naïve patients) or maintenance of virological suppression after a switch of ART to a RAL-containing regimen (experienced patients). Virological failure was defined as an increase in the HIV-RNA level of more than either 200 or 50 copies/ml. Patients whose HIV-RNA level was between 50 and 200 copies/ml in two consecutive measurements were considered to have a low-level replication, which was counted as virologic failure. In both approaches, ‘blips’, defined as one raised viral load with undetectable values before and after, were not considered as treatment failure.
Patients were analysed in two different groups (naïve and switch patients as described above). HIV-RNA level was measured every 12 weeks on routine clinical visits. Since we conducted a retrospective study, deviations from 12-weekly clinical visits of ±6 weeks were accepted. Patients were not excluded from the study, if they missed a clinical visit, but subsequent data were used instead if available, as described below. Patients who, by definition, did not respond to the RAL-containing ART but continued RAL therapy were followed up to see if HIV-RNA level would decrease subsequently.
We then also conducted a subgroup analysis of virological response regarding different regimens of BT among the group of treatment-experienced patients. A dual therapy of a boosted PI plus RAL was compared with a standard BT consisting of (N)NRTI, PI plus (N)NRTI or PI plus entry-inhibitors. Comparison was again carried out as a TLOVR analysis using survival functions to estimate the rate of patients with virological response as a function of the time of observation. Additionally a subgroup snapshot-analysis was performed at week 24 and at week 48 in accordance with the FDA guidelines regarding virological response. The definitions of virological response/failure, as mentioned above, were applied. Missing data were treated as per-protocol, so previous (week 24/week 36) or following (week 60/week 72) data were used in these cases, if available.
All data evaluation and statistical analyses were carried out using Microsoft Excel 2010 (Redmond/Washington), SPSS Statistics 19 (IBM, Armonk, New York 2010) and BiAS 10.0 (Epsilon Publishing 2012, Frankfurt, Germany). Group comparisons for significant differences were carried out using Chi square test, Fisher’ exact test and Mann-Whitney U test. Response rates to RAL therapy were statistically evaluated using a survival function to estimate the rate of patients with virological response as a function of time. These results were diagrammed in Kaplan-Meier plots.
Results
In all, 350 patients were identified from the database who had received RAL-containing ART between the approval of RAL in October 2007 and October 2012. Of these a total of 295 patients met the inclusion criteria mentioned above and were eligible to be enrolled. A total of 55 patients had to be excluded; eight due to incomplete data in the database, 20 due to mistaken entries in the database and 27 patients because they had visited the clinic fewer than two times during observation.
The remaining 295 patients were divided into two groups: patients being treatment-naïve prior to RAL therapy (n = 64) and patients who were treatment-experienced (n = 231).
Baseline characteristics.

ART, antiretroviral therapy; CDC, Centres of Disease Control and Prevention; DRV/r, darunavir/raltegravir; MVC, maraviroc; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
As BT, for both groups, an NRTI backbone was chosen in 66.8% (197 out of 295) of all patients, whereas 22.7% (66 out of 295) of all patients received dual therapy: RAL plus a boosted PI.
Baseline characteristics of experienced patients regarding the two groups of different BT as mentioned above show that 23.3% (14 out of 60) of patients in the ‘dual therapy’ group and 29.8% (51 out of 171) in the ‘standard BT’ group were women. Median CD4 cell count was 452.5 for the ‘dual therapy’ group and 459 in the ‘standard BT’ group. Median HIV-RNA level was 1.78 log10 copies/ml in the ‘dual therapy’ group and 1.6 log10 copies/ml for the group of ‘standard BT’ patients. Among the ‘dual therapy’ group, 6.7% (4 out of 60) had a hepatitis C coinfection while 16.6% (32 out of 171) were coinfected within the ‘standard BT’ group. The rate of patients having (had) AIDS, defined by CDC category C, was 35.0% (21 out of 60) within the ‘dual therapy’ group and 31.6% (54 out of 71) within the ‘standard BT’ group. Differences between the two groups were not significant (p > 0.05), except for ‘region of origin’, where p value was 0.01.
Among the group of treatment-naïve patients, 86.2% had constant HIV-RNA levels below 200 copies/ml at week 24 and onwards until the end of the observation period. Virological failure according to the definitions mentioned above therefore occurred in 13.8%. Low-level replication was found in 9.4%; not leading to failure in any case. 67.7% of treatment-naïve patients had constant HIV-RNA levels below 50 copies/ml at week 24 and onwards. Therefore, using 50 copies/ml as a cut-off, virological failure occurred in 32.3% at any time after week 24. Results are shown in Figure 1.
Response to RAL-therapy from week 24 on: ‘Time to loss of virologic response’ (TLOVR) analysis from week 24 on until the end of the observation period. Percentage of patients showing virologic response to RAL therapy for the whole time of observation.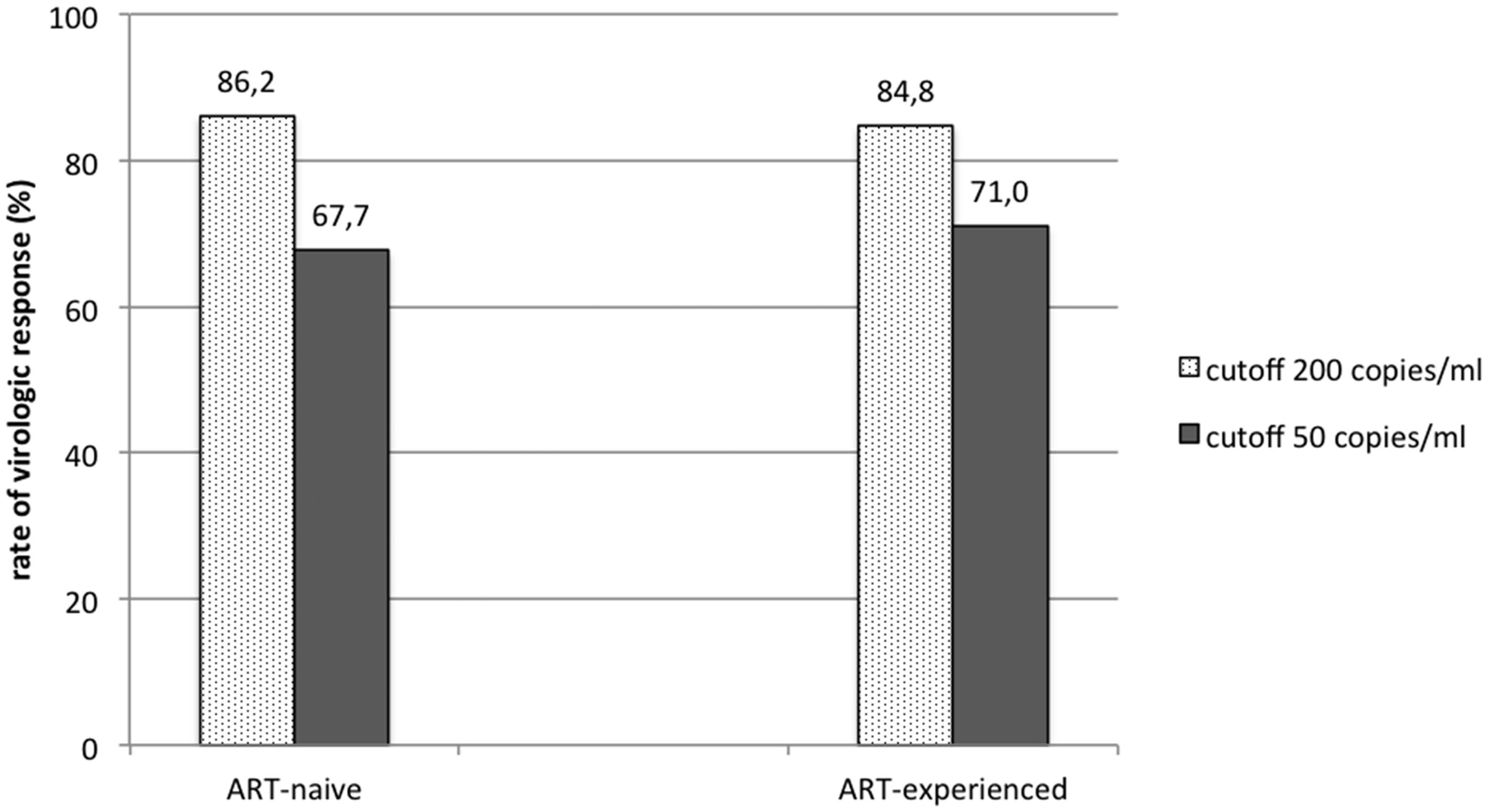
Among the group of treatment-experienced patients 84.8% had constant HIV-RNA levels below 200 copies/ml at week 24 and onwards until the end of the observation period. Virological failure according to the definitions mentioned above therefore occurred in 15.2%. Low-level-replication was found in 15 of 231 patients; leading to virological failure in eight patients. Of treatment-experienced patients, 71.0% had constant HIV-RNA levels below 50 copies/ml at week 24 and onwards. Therefore, using 50 copies/ml as cut-off, virological failure occurred in 29.0% at any time after week 24. Results are shown in Figure 1.
For the comparison of a dual therapy of boosted PI plus RAL with a standard BT consisting of (N)NRTI, PI plus (N)NRTI, or PI plus entry-inhibitors, 60 out of 231 treatment-experienced patients were identified to have been given a dual therapy while 171 patients had received a standard BT in addition to RAL.
Figure 2 shows Kaplan-Meier survival plots of the TLOVR analysis displaying virological response to RAL therapy as a function of the time of observation. Response rates are indicated for treatment-naïve and experienced patients separately using the two methods to define virological failure as described above. Differences were significant with p < 0.05 within both groups.
Virologic response to RAL-therapy displayed as a survival function over the time of observation (Kaplan-Meier survival plot). Numbers at risk: n = 64 for naïve patients; n = 231 for experienced patients. Two different cut-off viral load values to define virologic response/failure. p < 0.05 for both groups.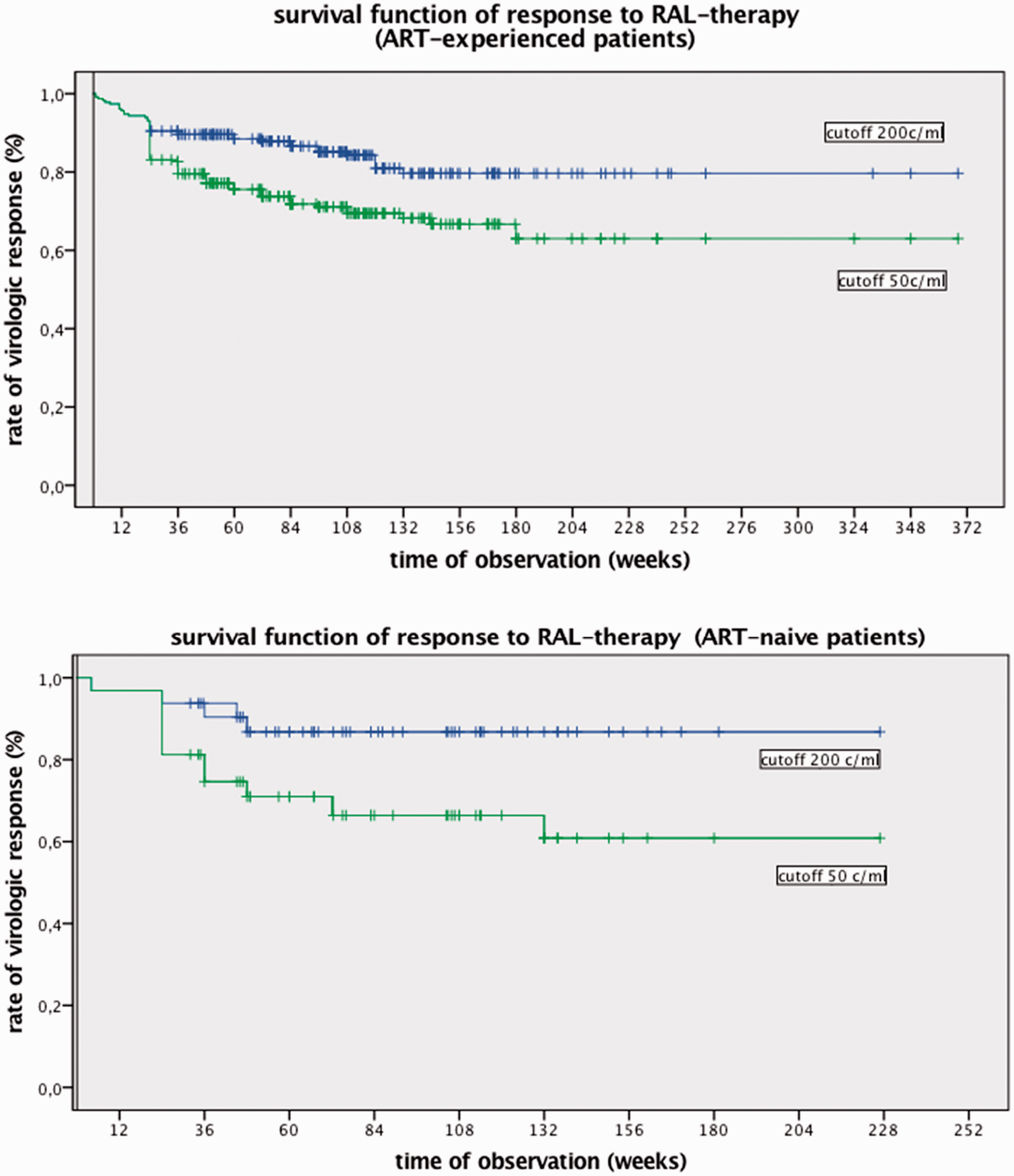
Figure 3 shows Kaplan-Meier survival plots (TLOVR analysis) comparing virological response to RAL therapy between the two different groups of BT as a function of the time of observation, again using ‘50 copies/ml’ as well as ‘200 copies/ml’ as cut-off viral load, respectively. In both approaches differences between the two groups were not significant.
Virologic response rates of different RAL-containing regimens in treatment-experienced patients: dual therapy vs. standard background therapy. Percentage of patients with virologic response as a function of time (Kaplan-Meier survival plot). P = 0.76 for cut-off 200 copies/ml; p = 0.58 for cut-off 50 copies/ml. Numbers at risk: n = 60 for ‘dual therapy’, n = 171 for ‘standard BT’ at baseline.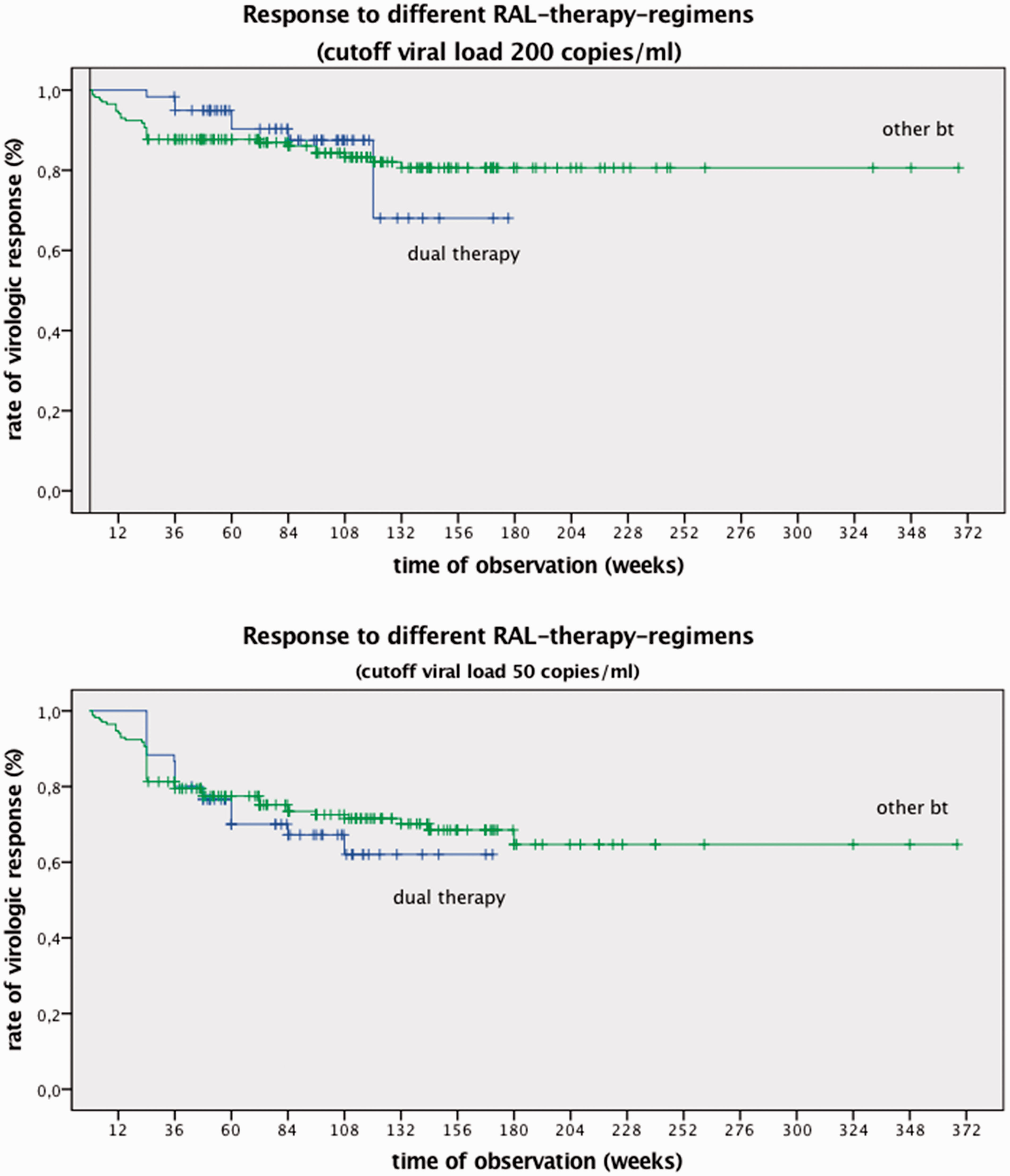
Snapshot-analysis regarding the two different BT-regimens showed: at week 24, 98.3% of the patients who received a dual therapy (86.7% using a cut-off of 50 copies/ml) showed virological response. Patients who received a standard BT showed virological response in 88.3% (81.3%). Please note that in this group data were missing for eight of 171 patients.
Comparison of dual therapy as background therapy vs. standard background therapy regimens in addition to RAL therapy: snapshot analysis of virologic response at weeks 24 and 48. Differences were not significant: p > 0.05 for all groups.

Resistance testing was performed in 23 of 295 patients; all 23 of them having had virological failure at or after week 24 with a viral load above 200 copies/ml. In 12 patients, emergence of resistance to RAL therapy could be detected. Three of these patients were treatment-naïve while the remaining nine patients had received a different ART regimen previously. Median time of detection was at week 48 (range 10–132) among all patients, at week 60 (range 36–96) for treatment-naïve patients and at week 36 among treatment-experienced patients (range 10–132). Integrase gene mutations identified in patients with virological failure mainly emerged from the two major pathways: Q148 & N155.14,15 N155 was affected in four patients and Q148 in five patients. Mutations of G140 occurred in three patients. In most cases where genotypic evidence of virological failure was obtained, combinations of several mutations were seen.
Discussion
The aim of this study was to investigate, in a retrospective view, long-term efficacy of different RAL-based antiretroviral therapies. To reproduce an image of real-life clinical practice of ART in a mixed population of patients no exclusions of comorbidities were made. Additionally we aimed to evaluate and compare efficacy of a dual therapy of RAL plus boosted PI with standard (NRTI-based) BTs given alongside RAL.
Results indicate that for both of the cut-off levels used for the evaluation of virological response, RAL, given twice daily (with BT), is an effective treatment for both treatment-naïve and experienced patients. 16 Considering the heterogeneity of the examined cohort, containing patients with or without (severe) comorbidities alike, results are even more notable. Of treatment-naïve patients in this study, 20.3% had a history of AIDS, being in CDC category C, and 10.9% of treatment-naïve patients had hepatitis B or C coinfection. Whereas, for example, in the STARTMRK study only 14% had a history of AIDS and 6% were coinfected with either hepatitis B or C. 5 However, more detailed research is needed here to evaluate response to RAL-containing ART in the clinical context of specific comorbidities or anti-infective cotherapies such as anti-mycobacterial therapy, chemotherapy or treatment of chronic hepatitis C infection.
Within the group of experienced patients no significant differences in virological response between dual therapy and standard (NRTI-based) BT regimens are seen in the TLOVR survival analysis. Virological response rates (cut-off level 200 copies/ml) to dual therapy are higher within the first 108 weeks, whereas the response to RAL plus standard (NRTI-based) BT seems to be more stable considering long-term efficacy. Snapshot analysis at both weeks 24 and 48 shows equal or higher response rates for a dual therapy regimen, using either one of the cut-off levels to define virological response. These differences are, however, not significant.
While further (prospective) studies are still needed to confirm these results, our data give a promising reference for dual therapy with RAL as an addition to the arsenal of ART regimens consisting of only two substances. Since this was not a randomised study, the selection of specific regimens was ultimately made by the treating clinician. Thus, there certainly is an inherent bias as usual in this kind of studies. This has to be kept in mind when interpreting our data, especially the comparisons of dual therapy vs. RAL plus standard (NRTI-based) BT.
In general, NRTI-sparing regimens containing RAL plus PI/r for treatment-experienced patients are still far from being established in clinical practice and very few data on long-term efficacy are available. This includes Allavena et al. 17 who described efficacy for a dual therapy in a small (n = 29) observational study and Tsukada et al. 18 who presented efficacy of a RAL plus DRV/r regimen after a median of 48 weeks (n = 19). Our findings also coincide with corresponding results presented by the SECOND-LINE study group for a dual therapy with lopinavir/r. 19
For treatment-naïve patients non-inferiority in efficacy and safety of a first line-dual therapy regimen was shown for darunavir/r by Raffi et al in the NEAT study as well as for boosted lopinavir in the PROGRESS study.20,21 These complementary results demonstrate the promising role of a dual therapy with RAL plus boosted PI as an alternative to conventional combination therapies in both treatment-experienced and -naïve patients.
In summary, this retrospective analysis shows the overall notable efficacy of RAL in clinical practice in a mixed population of patients with a variety of possible comorbidities. Especially in treatment-naive but also in experienced patients RAL plus NRTI-based BT or even as a dual therapy showed high efficacy also in long term treatment of 48 weeks and above. Thus a dual therapy of RAL plus a boosted PI appears to be a safe and effective alternative in the arsenal of antiretroviral treatment options, especially in first-line therapy of treatment-naïve patients but also for experienced patients with various comorbidities and previous ART-regimens.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MJ declares that there is no conflict of interest. GS received travel grants and fees for lectures from Abbvie, Bristol Myer Squibb, Gilead, Janssen, Merck Sharp Dome and ViiV. PdL received travel grants and fees for lectures from Bristol Myers Squibb, Gilead. TW received travel grants and fees for lectures from Abbvie, Bristol Myer Squibb, Gilead, Merck Sharp Dome and ViiV. CS received travel grants from Bristol Myer Squibb, Gilead and ViiV. The rest of the authors declare that there are no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.