
Abstract
We present the updated British Association for Sexual Health and HIV guideline for the management of non-gonococcal urethritis in men. This document includes a review of the current literature on its aetiology, diagnosis and management. In particular it highlights the emerging evidence that azithromycin 1 g may result in the development of antimicrobial resistance in Mycoplasma genitalium and that neither azithromycin 1 g nor doxycycline 100 mg twice daily for seven days achieves a cure rate of >90% for this micro-organism. Evidence-based diagnostic and management strategies for men presenting with symptoms suggestive of urethritis, those confirmed to have non-gonococcal urethritis and those with persistent symptoms following first-line treatment are detailed.
Scope and purpose
This guideline has two main objectives:
The relief of symptoms in the affected men. To reduce the number of sexually transmitted infections (STIs) and the complications that can arise in people either presenting with signs and symptoms of an STI or undergoing investigation for possible infection.
Specifically, this guideline offers recommendations on the diagnostic tests, treatment regimens and health promotion principles needed for the effective management of non-gonococcal urethritis (NGU), covering the management of the initial presentation as well as how to prevent transmission and future infection.
It is aimed primarily at health care professionals seeing people aged 16 years or older (see specific guidelines for those under 16) in departments offering Level 3 care in STI management within the United Kingdom. However, the principles of the recommendations should be adopted across all levels. As NGU is a condition that occurs only in men the guideline is only applicable to men except where it addresses the management of women who are sexual partners of men with NGU.
The recommendation of this guideline may not be appropriate for use in all clinical situations. Decisions to follow these recommendations must be based on the professional judgement of the clinician and consideration of individual patient circumstances and available resources.
Guideline development
This guideline has been updated by reviewing the previous NGU (2008) guideline and conducting a comprehensive literature search of publications from 2008 to December 2013. MEDLINE was used to identify published articles including the search terms ‘nongonococcal urethritis’, ‘non-gonococcal urethritis’, ‘nonspecific urethritis’, ‘non-specific urethritis’ and broadened the search to include ‘urethritis’ and urethritis combined with ‘Chlamydia trachomatis’ or ‘Mycoplasma genitalium’. Reviews, case reports, editorials, comments, letters, research pertaining to the development of laboratory assays and the study of genomics were excluded. Due to the paucity of clinical trials all entries in the English language were reviewed, and if relevant the full text obtained.
Direct comparison of published studies is hindered by the majority lacking a clear microscopic definition of NGU, or using an alternative definition to ‘five or more polymorphonuclear leucocytes (PMNLs) per high-powered field averaged over five fields with the greatest concentration of polymorphs’ and varying specimen collection techniques. Due to scarcity of relevant high-quality research these studies have been included despite their limitations.
The first draft of the guideline was prepared by PH and KB and reviewed by all co-authors and the CEG. Following this the guideline was placed on the (public) British Association for Sexual Health and HIV (BASHH) website for two months and comment invited from the whole of the specialty. Consensus was used to resolve differences in expert opinion and where this was not possible the CEG had the final decision. Essentially this related to the continued recommendation of azithromycin 1 g as first-line therapy. 1 The guideline was reviewed by the BASHH Public and Patient Panel and appropriate comments incorporated into the guideline.
Introduction
Urethritis, or inflammation of the urethra, is a multifactorial condition which is sexually acquired in the majority of (but not all) cases. It is characterised by urethral discharge, dysuria and/or urethral discomfort but may be asymptomatic. The diagnosis of urethritis is confirmed by demonstrating an excess of PMNLs in the anterior urethra. This is usually assessed using a urethral smear but a first-pass urine specimen (FPU) can also be used. Urethritis is described as either gonococcal, when Neisseria gonorrhoeae is detected, or non-gonococcal (NGU) when it is not. The term non-specific urethritis (NSU) applies to non-gonococcal non-chlamydial NGU and in order to prevent confusion should be avoided. It has been suggested that mucopurulent non-gonococcal cervicitis is the female equivalent with approximately 20%–40% of cases being due to infection with Chlamydia trachomatis and 5–20% Mycoplasma genitalium.2–6 However, clinical diagnosis of this condition is problematic as there are at least three different diagnostic criteria which, although having similar sensitivities and specificities for detecting C. trachomatis and M. genitalium in high-risk women, are concordant in only <50%. 5 Cervicitis diagnosed by Gram-stained smear has the strongest association with M. genitalium. 6
Aetiology
Prevalence of the most common pathogens isolated from patients with non-gonococcal urethritis (NGU).
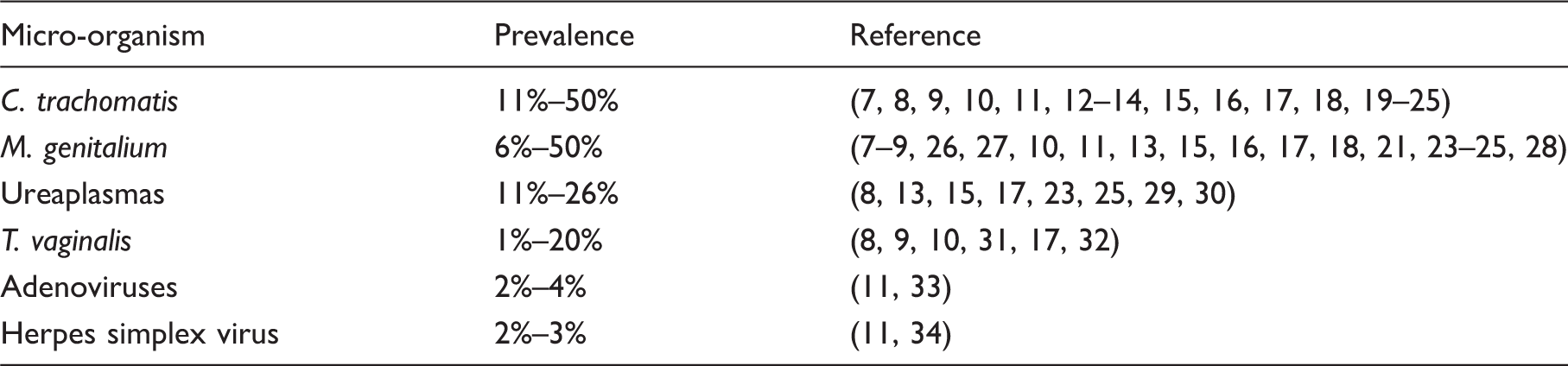
The commonest organisms implicated are C. trachomatis and M. genitalium with the latter perhaps causing more symptoms7,26
Chlamydia and M. genitalium are more likely to be detected in:
In 30%–80% of the cases with NGU, neither C. trachomatis nor M. genitalium is detected.7–9,11–14,26,35,39
Pathogen-negative NGU is more likely with increasing age and the absence of discharge or clinical symptoms.8,9,35 The detection of Trichomonas vaginalis is dependent on the prevalence of the organism in the community, being more common in non-white ethnic groups. This infection appears to be uncommon in the United Kingdom although there are only limited studies using the new commercial nucleic acid amplification tests (NAATs) for detecting T. vaginalis, which are more sensitive than previous tests.
31
In the United States prevalences of 2.5%–17% have been reported.8,9,10,31,40
Ureaplasmas have been inconsistently associated with NGU.13,41 Earlier studies did not differentiate between the two species Ureaplasma urealyticum and U. parvum. There is increasing evidence that it is only U. urealyticum that is pathogenic in some men at least, but not U. parvum.8,15,42–44
○ U. urealyticum may account for 5%–10% of cases of acute NGU. A urinary tract infection was found in 6% of men with acute NGU in a single study.
45
Adenoviruses may account for perhaps 2%–4% of symptomatic patients and is often associated with a conjunctivitis.11,33 Herpes simplex viruses types 1 and 2 are an uncommon cause of NGU (2%–3%).11,34 Epstein-Barr virus, N. meningitidis, Haemophilus sp., Candida sp., urethral stricture and foreign bodies have all been reported in a few cases and probably account for a small proportion of NGU.
34
Bacterial vaginosis-associated bacteria may also cause NGU in some men.46–48 What causes organism-negative NGU, or idiopathic urethritis as it is sometimes known, is unclear and has recently been reviewed.
48
Some of these cases are almost certainly non-infective but the tools to be able to differentiate between infective and non-infective cases are not currently available.
46
Asymptomatic urethritis, without an observable discharge, probably has a different aetiology from symptomatic urethritis, with C. trachomatis and M. genitalium being detected less frequently.7,16,26,35 There is also a possible association of asymptomatic NGU with bacterial vaginosis. 49 What causes organism-negative urethritis in these men is unclear and although the evidence is weak the proportion due to an unknown pathogenic sexually transmissible infection is likely to be low. 50 It is recommended that asymptomatic men should not be tested for non-gonococcal urethritis.
Clinical features
Symptoms
Urethral discharge Dysuria Penile irritation Urethral discomfort Nil
Signs
Urethral discharge. This may not have been noticed by the patient or may only be present on urethral massage. Balano-posthitis Normal examination
Complications
Epididymo-orchitis Sexually acquired reactive arthritis / Reiter’s syndrome. These are infrequent, occurring in fewer than 1% of cases, though incomplete forms may be more common.
Diagnosis
Only symptomatic patients and/or those with a visible discharge or presence of balano-posthitis should be assessed for the presence of urethritis (IV, C).
The diagnosis of urethritis should be confirmed by demonstrating five or more PMNLs per high power (×1000) microscopic field (averaged over five fields with the greatest concentration of PMNLs) on a smear obtained from the anterior urethra.
51
The quality of the smear is heavily dependent on how the smear is taken and there is both inter- and intra-observer variation when interpreting the result.52,53 Either a 5-mm plastic loop or cotton tipped swab can be used, which should be introduced about 1 cm into the urethra. A 5-mm plastic loop is less painful than a Dacron swab, which is less painful than a Rayon swab
54
(Ib, A). If a urethral discharge is present and can be adequately sampled without placing the loop or swab inside the meatus, then this is the recommended method for obtaining a smear as it is likely to be preferred by the patient.
54
However, this has not been compared to the standard technique in a clinical trial (IV, C).
Examining a Gram-stained preparation from 10 to 20 mL of a centrifuged sample of an FPU specimen, containing 10 or more PMNL per high-power (×1000) microscopic field (averaged over five fields with the greatest concentration of PMNLs) is not possible in the majority of clinical laboratories as centrifuges are not routinely available. Instead a FPU specimen can be examined for threads and if present these can be Gram-stained and interpreted as for a spun deposit12,55 (III, B).
Investigation of symptomatic patients with a negative urethral smear
Possible use of a leucocyte esterase dipstick on the remains of the FPU specimen.
○ While positive leucocyte esterase activity on dipstick of an FPU specimen correlates with NGU and the detection of chlamydia,
13
it does not have adequate sensitivity to be considered a reliable rapid diagnostic test for acute NGU and false positives can occur.56,57 ○ It is therefore not recommended for diagnosis of NGU in a Level 3 service where microscopy is available. In the 2010 Centers for Disease Control and Prevention guideline ≥1+ would be considered consistent with the presence of urethritis (IV, C) (http://www.cdc.gov/std/treatment/2010/STD-Treatment-2010-RR5912.pdf.). In a Level 3 service where a symptomatic patient has had a negative urethral smear, performing a leucocyte esterase dipstick on the remains of the FPU specimen could be considered, and if ≥1, a diagnosis of NGU could be made. The most likely cause for this is an inadequate urethral smear (see above) and if this is consistently observed the clinic should review its sampling technique for microscopy. If the urethral smear is negative, the patient can be reassured and advised to re-attend for an early morning smear if his symptoms do not settle. He should be advised to hold his urine overnight and to attend not having voided urine. It is good practice to advise the patient to take their last drink about 8 p.m. and to void about three hours later in order to help avoid waking with a full bladder (IV, C). Empirical treatment is not recommended as there is a risk it may perpetuate their symptoms by increasing their anxiety (IV). This should only be given in exceptional circumstances. In such situations treatment to the partner(s) would also be indicated.
The sensitivity of the smear test for diagnosing urethritis, but probably not the FPU in detecting chlamydia,58,59 is affected by the period since last passing urine. The optimum time to ensure a definite diagnosis in a symptomatic man is not known but 2–4 hours is conventional (IV, C).
Investigation of patients in settings in which microscopy is not available
Symptomatic patients should be referred to a centre which has microscopy available; however, some patients may not wish to re-attend another health care setting. The following can be used to make a diagnosis of urethritis. The sensitivity and specificity is imperfect compared to a urethral smear.
Investigations
All patients attending should be tested for N. gonorrhoeae and C. trachomatis. If positive, management should be as specified in the UK national guidelines produced by BASHH. Tests for M. genitalium and U. urealyticum are currently not widely available in the United Kingdom. Testing male patients with urethritis for M. genitalium (and for macrolide resistance if detected) would be helpful in management and should be performed if available.
6
The role (if any) of tests for U. urealyticum in routine clinical practice, if they become available, has not been determined.
6
As symptoms of a urinary tract infection may overlap with those of urethritis, if the patient complains of severe dysuria, visible haematuria (or if microscopic haematuria is discovered incidentally), nocturia, urinary frequency, urgency or is at low risk for an STI, then a urinary dipstick analysis on a mid-stream urine specimen should be considered and urine sent for microscopy, culture and antibiotic sensitivity testing.45,62 Although a urinary dipstick is only 68%–88% sensitive, it is inexpensive and a useful screening test
63
(IV, C). If a urinary tract infection is confirmed then referral for urological assessment should be considered.
Management
General advice
The following should be discussed and clear written information should be provided (see BASHH patient information on NGU):
An explanation of the causes of NGU, including non-infective causes, and possible short-term and long-term implications for the health of the patient and his partner(s). The side-effects of treatment and the importance of complying fully with it. The importance of their sex partner(s) being evaluated and treated. Advice to abstain from sexual intercourse or, if that is not acceptable, the consistent and correct use of condoms, including for oral sex, until he has completed therapy and his partner(s) have been treated (IV, C). Advice on safer sex (see UK national guideline on safer sex). The importance of complying with any follow-up arrangements made.
Treatment
Treatment should be initiated as soon as the diagnosis is made and without waiting for the results of tests for chlamydia and cultures for N. gonorrhoeae. Ideally, treatment should be effective (microbiological cure >95%), easy to take (not more than twice daily), with a low side-effect profile, and cause minimal interference with lifestyle. However, assessing treatment efficacy is not straightforward as persistence of inflammation may not indicate persistent infection.13,64,65 It is important to note that detectable inflammation may persist for an unknown length of time even when the putative organism has been eliminated. 66 Two recent, large randomised controlled trials from the United States comparing azithromycin 1 g and doxycycline 100 mg twice daily for seven days observed that both regimens are <85% effective.17,18
Chlamydia: please refer to the current UK chlamydia guideline produced by BASHH.
Mycoplasma genitalium
A number of studies indicate that doxycycline 100 mg twice daily has a microbiological failure rate of up to 68%.9,17,18 The microbiological failure rate of azithromycin 1 g is 13%–33% and is associated with isolates containing 23sRNA gene mutations associated with macrolide antimicrobial resistance.1,9,17,18,67–70 There is increasing evidence that treatment with azithromycin 1 g can induce mutations in the 23sRNA gene resulting in macrolide antimicrobial resistance.1,68–73 There is weak evidence that a prolonged course of azithromycin 500 mg stat then 250 mg daily for a further four days is more effective than a 1-g dose as this has not been assessed within a randomised controlled trial.68,74,75 In addition, the five-day regimen does not appear to induce macrolide antimicrobial resistance.68,74,75 A five-day regimen is biologically more sensible than a single dose as it is a slow-growing micro-organism.
76
Early generations of quinolones such as ofloxacin and ciprofloxacin are not highly active against M. genitalium.6,75,76 However, newer generation quinolones such as moxifloxacin appear to have high efficacy although the numbers treated in studies have been small.6,70,75–78 There is evidence that mutations in the quinolone-resistance determining regions (QRDRs) of the gyrA and parC genes can occur, with a prevalence of 10% in Japan.
79
Such mutants are likely to be resistant to moxifloxacin. There is some evidence that a 14-day regimen may be more effective than a seven-day regimen.
80
Ureaplasmas
There are limited recent antimicrobial studies on this micro-organism with few differentiating between the two species and the majority being in-vitro antimicrobial studies. Previous studies indicate that both macrolides and tetracyclines are more than 80% effective and resistant isolates do occur.81–83 Azithromycin 1 g and doxycycline 100 mg twice daily for seven days were recently demonstrated to have similar efficacy, 75% and 69%, respectively, against U. urealyticum.17,84 Ofloxacin is active in vitro against ureaplasmas but moxifloxacin is more effective.77,85 Quinolone antimicrobial resistant mutants do occur.
85
Strong clinical suspicion of UTI (see above)
Give empirical antibiotics for a presumed UTI according to local prescribing policies and local knowledge of antibiotic sensitivities.
All the regimens described below are oral.
RECOMMENDED REGIMENS (GRADE OF RECOMMENDATION A)
Doxycycline 100 mg twice daily for seven days (Ib)
Or
Azithromycin 1 g stat (Ib) (see comments below and risk of inducing macrolide antimicrobial resistance with M. genitalium)
Or
If the patient (or their sexual partner) is known to be M. genitalium-positive: azithromycin 500 mg stat then 250 mg daily for the next four days (see above) (B, IIb)
ALTERNATIVE REGIMENS (A)
Ofloxacin 200 mg twice daily, or 400 mg once daily, for seven days (Ib)
Or
Azithromycin 500 mg stat then 250 mg daily for the next four days (see above) (B, IIb)
Doxycycline 100 mg twice daily for seven days as first-line therapy
Is more than 95% effective in men who are chlamydia positive.17,18,86 Although only effective in less than 50% of men who are M. genitalium-positive there is no evidence that it induces antimicrobial resistance and thus those who fail therapy should respond to a prolonged course of azithromycin (see persistent NGU). It is as effective as azithromycin 1 g in men who are U. urealyticum-positive.
Azithromycin 1 g stat as first-line therapy
Single-dose therapy has the advantage of good compliance. Two recent well-conducted RCTs demonstrated less than 95% efficacy with azithromycin 1 g.17,18 There are a number of potential explanations for this.87,88 Is less than 90% effective in men who are M. genitalium-positive even if macrolide susceptible. M. genitalium-positive men who fail therapy are at risk of developing a 23sRNA gene mutation conferring antimicrobial resistance. If this were to occur then an extended five-day azithromycin regimen would not be effective at eradicating the infection.
Sexual contacts/partners
All sexual partners at risk should be assessed and offered epidemiological treatment, maintaining patient confidentiality. The duration of ‘look back’ is arbitrary; four weeks is suggested for symptomatic men (see BASHH Statement Partner Notification).
If C. trachomatis or N. gonorrhoeae are detected it is important to ensure that all sexual partner(s) potentially at risk have been notified and should be managed as detailed in the BASHH guidelines for the management of chlamydia and gonorrhoea (available at http://www.bashh.org/BASHH/Guidelines/Guidelines/BASHH/Guidelines/Guidelines.aspx).
Details of all contacts should be obtained at the first visit. Consent should also be obtained so that if C. trachomatis or N. gonorrhoeae are detected subsequently, and the index patient does not reattend, he can be contacted and/or provider referral can be initiated for sexual contacts (IV, C). There is no direct evidence of treatment benefit to partners of men with chlamydia-negative NGU. There are, however, a number of issues that may influence decision making:
○ M. genitalium accounts for approximately 15%–30% of cases and probably causes disease in women.6,76 ○ There are reports of patients with persistent or recurrent ureaplasma-positive urethritis being cured only after their sexual partner received appropriate treatment.
89
○ There is conflicting evidence that partners of such men may be at increased risk of testing chlamydia-positive.46,90 ○ In the absence of randomised prospective studies it would be prudent to treat partners of micro-organism-negative NGU concurrently to potentially reduce female morbidity and risk of recurrent/persistent NGU in the index men. Doxycycline 100 mg twice daily orally for seven days or azithromycin 1 g stat are recommended (see notes above). Women who are pregnant, at high risk of pregnancy or are breast feeding should be treated with azithromycin 1 g (IV, C). ○ See below for discussion of the management of sexual partners of men with persistent or recurrent NGU.
Follow-up for patients with NGU
Follow-up is only indicated if chlamydia is confirmed (see UK guideline) or if the man has persistent symptoms. Patients who remain symptomatic should be asked to return to the clinic and retreated with an appropriate regimen and the possibility of re-infection explored (IV, C).
Persistent and recurrent NGU
Persistent NGU, when symptoms do not resolve following treatment, occurs in 15%–25% of patients following initial treatment of acute NGU. Recurrent NGU is empirically defined as the recurrence of symptomatic urethritis occurring 30–90 days following treatment of acute NGU 13 and occurs in 10%–20% of patients.13,91
The aetiology of persistent NGU is probably multifactorial with an infectious agent being identified in less than 50% of cases.9,13,91,92 M. genitalium has been identified in 20%–40%9,13,92,93 and C. trachomatis in 10%–20% of men treated with azithromycin 1 g. 18 Ureaplasmas may also play a role in some men.13,44,94 T. vaginalis can be identified in up to 10% in populations where it is endemic. 8
Any treatment of persistent NGU should cover M. genitalium and T. vaginalis and/or bacterial vaginosis-associated bacteria. The only randomised controlled trial for persistent NGU was undertaken before M. genitalium had been identified as an important pathogen and used erythromycin, an older generation macrolide. 95 Although a three-week course was better than placebo it is not clear how relevant this regimen is today given that better macrolides are available which have fewer side-effects. 96
As there is a lack of evidence that female partners of men with persistent/recurrent NGU are at increased risk of pelvic inflammatory disease, the historical advice has been that they do not need to be retreated if treated appropriately initially. However, in view of the emerging evidence that persistence of M. genitalium following treatment with single-dose azithromycin (1 g) is probably equally likely in men and women, and that doxycycline is less than 50% effective, 71 it is likely that re-treatment of the sexual partner and index case will be beneficial if persistent/recurrent NGU in the index case resolves following extended therapy but subsequently recurs. This remains an area where further research is needed. It would be sensible to use the extended regimen demonstrated to be effective unless contraindicated (IV, C).
Diagnosis of persistent/recurrent NGU (IV, C)
Only perform a Gram-stained urethral smear in men who are symptomatic. For those patients with confirmed chlamydia at initial presentation please refer to the BASHH chlamydia guideline for advice on repeat NAAT testing. Consider testing for T. vaginalis using a NAAT if available. Consider testing for M. genitalium e.g. through Public Health England’s Sexually Transmitted Bacterial Reference Laboratory, Colindale, London.
Management of persistent/recurrent NGU (IV, C)
Ensure that the patient has completed the initial course of therapy and that re-infection is not a possible cause. Only treat if the patient has definite symptoms of urethritis and either physical signs on examination or microscopic evidence of urethritis. Reassure asymptomatic patients that no further test or treatment is necessary.
RECOMMENDED REGIMENS (at second attendance or first follow-up visit):
Preferred regimen
Azithromycin 500 mg stat then 250 mg daily for the next four days (III, B) plus metronidazole 400 mg twice daily for five days (IV, C)
NB: azithromycin is now off-patent and considerably cheaper than when this regimen was first introduced and a higher dose regimen of azithromycin 1 g stat then 500 mg for the next four days could be considered 88 (IV, C).
The use of azithromycin 1 g as first-line treatment for acute NGU has the risk of inducing macrolide resistance in M. genitalium, a common cause of persistent/recurrent NGU (see above), in which situation the prolonged regimen of azithromycin is unlikely to be effective.
Alternative regimen
Moxifloxacin 400 mg orally once daily for 10–14 days (IIIb, B) plus metronidazole 400 mg twice daily for five days (IV, C)
NB: In persistent / recurrent cases, moxifloxacin is not recommended as a preferred therapy due to recent safety concerns (an increased risk of life-threatening liver reactions and other serious risks) from the UK Medicines and Healthcare products Regulatory Agency. However, it may be used if the patient is considered at risk of having M. genitalium which is resistant to macrolides (IV, C).
Continuing symptoms
There is only limited evidence on how best to manage patients who either remain symptomatic following a second course of treatment or who have frequent recurrences after treatment.
Moxifloxacin 400 mg orally once daily for 7–14 days (IIIb, B)
○ Consider quinolone antimicrobial resistance as a cause of treatment failure in men who remain M. genitalium-positive after treatment with moxifloxacin. At present no registered antibiotics are available for treatment. Pristinamycin is registered in France and may be effective in most cases.
97
Urological investigation is usually normal unless the patient has urinary flow problems98–100 and is not recommended (IV, C). Chronic abacterial prostatitis, the chronic pelvic pain syndrome and psychosexual causes should be considered in the differential diagnosis.95,101,102 For men with persistent or recurrent urethritis, although there is currently no evidence that retreatment of an appropriately treated sexual partner is beneficial (see above), this would be prudent if the man with chronic NGU is cured following extended therapy but subsequently relapses following resumption of sexual intercourse (IV, C). In this scenario the index case should be retreated and the sexual partner should be treated concurrently with the same antibiotic regimen which was effective in the index. Erythromycin 500 mg four times daily for three weeks has been shown to be effective,
94
but this was undertaken before the new macrolides were generally available.
96
Clarithromycin is better absorbed, has an improved side-effect profile and can be taken twice a day.
96
Consideration should be given to using clarithromycin 500 mg twice daily for three weeks as an alternative to erythromycin (IV, C). Crofts et al. recently published a “How to…” article on how to manage men with persistent symptoms which they have demonstrated to be effective.99,100,102 This describes a structured biopsychosocial, holistic management strategy, developed by P Horner, incorporating evidence-based pharmacotherapy for men who have the chronic pelvic pain syndrome (CPPS), a complex condition which overlaps with chronic urethritis.
Auditable outcome measures
All patients with NGU should be screened for genital infection with C. trachomatis and gonorrhoea. All patients identified with NGU should have a documented offer of written information about their condition. All patients with NGU should receive first-line treatment or the reasons for not doing so should be documented. All patients with NGU should have partner notification carried out in accordance with the BASHH statement on partner notification.
Qualifying statement
The recommendations in this guideline may not be appropriate for use in all clinical situations.
Decisions to follow these recommendations must be based on the professional judgement of the clinician, consideration of individual patient circumstances and available resources. All possible care has been undertaken to ensure the publication of the correct dosage of medication and route of administration. However, it remains the responsibility of the prescribing physician to ensure the accuracy and appropriateness of the medication they prescribe.
Updating
The BASHH Clinical Effectiveness Group meets regularly and will consider the need to update this guideline depending on developments in the field. As a minimum it will be revised five years after publication.
Editorial independence
This guideline was commissioned, edited and endorsed by the BASHH CEG without external funding being sought or obtained.
All members of the guideline writing committee completed the BASHH declarations of interest form (see below) at the time the final draft of the guideline was submitted to the CEG for approval.
P Horner has received funding from Hologic, Cepheid, Atlas Genetics and Siemens for work undertaken in STI diagnostics. He has also undertaken work as a consultant for Aquarius Population Health which provides advice to companies developing diagnostic point-of-care tests.
K Blee: No declarations of interest.
KW Radcliffe: No declarations of interest.
Membership of the CEG: Keith Radcliffe (Chair), Mark FitzGerald, Deepa Grover, Steve Higgins, Margaret Kingston, Neil Lazaro, Louise Melvin, Ann Sullivan.
Footnotes
Acknowledgements
The authors thank the following people who made useful comments during the development of this guideline: John Evans-Jones, Mark FitzGerald, Deepa Grover, Steve Higgins, Margaret Kingston, Neil Lazaro, Tariq Sadiq, Paul Schrober, Ann Sullivan.