
Abstract
Opinions are divided on whether to screen asymptomatic men for non-chlamydial non-gonococcal urethritis (NCNGU). We systematically reviewed the literature to determine whether male asymptomatic NCNGU is associated with significant clinical outcomes for men and/or their sexual partners. We searched electronic databases and reference lists from retrieved articles and reviews. No studies reporting clinical outcomes in men with asymptomatic NCNGU were identified. Two eligible studies report rates of sexually transmitted infections (STIs) in female partners of men with asymptomatic NCNGU; Chlamydia trachomatis was detected in 2.4% and 8.3% of these women. The evidence available is insufficient in quality and breadth to enable us to conclude whether asymptomatic NCNGU is associated with significant health consequences for men or their sexual partners; however, clinical consequences of asymptomatic NCNGU are poorly investigated. Clinicians should be aware of the limitations of the evidence on which current screening guidelines for asymptomatic men are based.
Keywords
Introduction
Non-chlamydial non-gonococcal urethritis (NCNGU) is a common condition that is believed to be sexually transmitted. Approximately 70,000 men in the UK receive this diagnosis each year. 1 It is characterized by microscopic findings of polymorphonuclear leukocytes (PMNLs) on urethral Gram stain in the presence (symptomatic NCNGU) or absence (asymptomatic NCNGU) of urethral discharge, dysuria, urethral itching and penile irritation in men in whom Chlamydia trachomatis and Neisseria gonorrhoeae have been excluded.
Several pathogens such as Trichomonas vaginalis, Herpes simplex virus and adenovirus have been linked with NCNGU but recent interest has focused on Mycoplasma genitalium, which accounts for between 10% and 46% of cases of NCNGU.2,3 M. genitalium appears to be associated predominantly with symptomatic presentations4–7 and although associations have been reported with a number of adverse health consequences in women, including pelvic inflammatory disease (PID) and tubal factor infertility,8–10 testing for and treatment of M. genitalium is not current standard of care in UK. 11
The significance of NCNGU in men is the subject of debate,12–16 largely due to the paucity of high-quality clinical studies. In particular, opinions are divided on whether or not to screen asymptomatic men for NCNGU. This is important in the current context of wider roll out of non-invasive sexually transmitted infection (STI) screening in settings without access to microscopy. UK and Australian guidelines for testing of STIs no longer recommend urethral smear microscopy in asymptomatic men.11,17 Instead, there is a reliance on the presence of symptoms to indicate likely infection and the high sensitivities and specificities of non-invasive tests to detect asymptomatic infection with C. trachomatis and N. gonorrhoeae. This has led to a reduction in the number of men diagnosed with and treated for asymptomatic NCNGU and is likely to limit research on this condition in the future. However, the public health consequences of untreated asymptomatic NCNGU for men and their sexual partners are unknown.
Our study takes a systematic approach to a poorly understood but common clinical presentation. Here we systematically review the published literature to determine whether asymptomatic NCNGU, as diagnosed in routine UK clinical practice by urethral smear microscopy and negative tests for C. trachomatis and N. gonorrhoeae, is associated with significant clinical consequences in men and/or their sexual partners in order to better inform STI screening and testing policy.
Methods
Databases, search strategy and search terms
We searched four electronic databases (MEDLINE, EMBASE, CINAHL and PsycINFO) using terms including urethritis, nonspecific, non-chlamydial, non-gonococcal, non-specific urethritis (NSU), non-gonococcal urethritis (NGU), NCNGU and non-gonococcal non-chlamydial urethritis (NGNCU) (see Appendix 1, available online only at: http://www.ijsa.rsmjournals.com/cgi/content/full/22/5/338/DCl) and included literature published after January 1965 (the year C. trachomatis was first recognized as a cause of urethritis 18 ) to February 2010. Results were also restricted to English language for practical reasons.
JMS screened titles and abstracts for potential relevance (based on accepted clinical knowledge of the subject 19 ) and allocated them into one of two groups; ‘for exclusion’ or ‘for further assessment to determine eligibility’. If relevance could not be assessed from the title and abstract, we obtained a full text version. The second researcher (CSE), blinded to the first researcher's initial group allocation, reviewed a random sample of 10% of the study titles in each group to assess reliability of the screening process. Any differences were resolved by discussion between the researchers and a final group of relevant articles for assessment of eligibility was agreed. In order to capture articles potentially missed by the literature search but with outcomes of relevance embedded in their text, full text articles were also retrieved for relevant references quoted in review articles and editorials on NCNGU.
Types of study included
We included studies that reported clinical outcomes for men with asymptomatic NCNGU and/or their sexual partners. Trials, observational studies, including cohort and non-comparative case series, were eligible for inclusion but we excluded case reports.
Participants
Men with asymptomatic NCNGU and sexual partners (any gender) of men with asymptomatic NCNGU.
Inclusion and exclusion criteria
Studies had to meet the following accepted definition of asymptomatic NCNGU in order to be included:
Asymptomatic men with a Gram or methylene blue-stained urethral smear containing ±5 PMNLs per high-powered field (HPF) (x 1000) averaged over five fields with the greatest concentration of PMNLs, or a Gram stain of a pellet produced by centrifuge of first void urine containing ≥10 PMNL/HPF averaged over five fields with the greatest concentration of PMNLs.
19
Studies not reporting a diagnostic criteria based on microscopy were excluded. However, we did include studies using a higher threshold for detection than the ≥5 PMNL/HPF if explicitly stated. The asymptomatic status of the male index cases could be self-reported or clinician elicited; A negative urine or urethral swab nucleic acid amplification test (NAAT) or culture test for C. trachomatis and N. gonorrhoeae. Thus, studies that used enzyme immunoassay, serology or other non-NAAT, non-culture methods for detection of C. trachomatis, or studies that used a leukocyte esterase test to diagnose urethritis were excluded because of variable and low reported specificities and sensitivities.20,21
Validity
Because of the limited number of studies relating to asymptomatic NCNGU, we included all studies regardless of our assessment of validity.
Data extraction
Data were extracted by the authors independently and disagreements settled through discussion.
Outcome measures
We included any recognized clinical outcome 22 in the index male patients and/or their sexual partners including, but not restricted to, epididymitis, conjunctivitis, arthritis, infertility, PID including salpingitis and endometritis, cervicitis, diagnosis with another STI, miscarriage, premature delivery and psychological diagnoses. We also included studies that investigated the relationship between asymptomatic NGNCU and HIV seminal plasma viral load as this has been linked with enhanced HIV transmission, which we considered a relevant potential clinical outcome. 23
Results
We identified 1413 references from the search. There was an 85% agreement between reviewers of the initial screening process and we reached consensus by discussion for the remaining 15%. We retrieved full papers for 103 titles, 101 of which failed to meet the inclusion criteria leaving two eligible studies (see Figure 1 and Appendix 2 of excluded studies [available online only at http://www.ijsa.rsmjournals.com/cgi/content/full/22/5/338/DC1]). No previous systematic review was found in the Cochrane database library and no ongoing UK-funded studies were identified from the National Institute for Health Research (NIHR) clinical research network portfolio database. Three studies included asymptomatic and symptomatic men with NCNGU but did not report separate clinical outcomes for the asymptomatic group and were therefore excluded from further analysis.4,24,25
1. Association of asymptomatic NCNGU with adverse health outcomes in men.
We did not find any eligible studies reporting adverse physical or psychological health outcomes for men with asymptomatic NCNGU.
2. Association of asymptomatic NCNGU with adverse health outcomes in sexual partners of men with the condition.
Two studies described relevant outcomes as summarized in Table 1.26,27 These studies investigate associations of asymptomatic NCNGU with concomitant STIs in sexual partners. C. trachomatis was detected in 2.4% 27 and 8.3% 26 of female partners of men with asymptomatic NCNGU. A single study also detected pathogen-negative PID in 2.4% and cervicitis in 9.4% of female partners. 27
Association of NCNGU in men and concomitant STIs in their female sexual partners
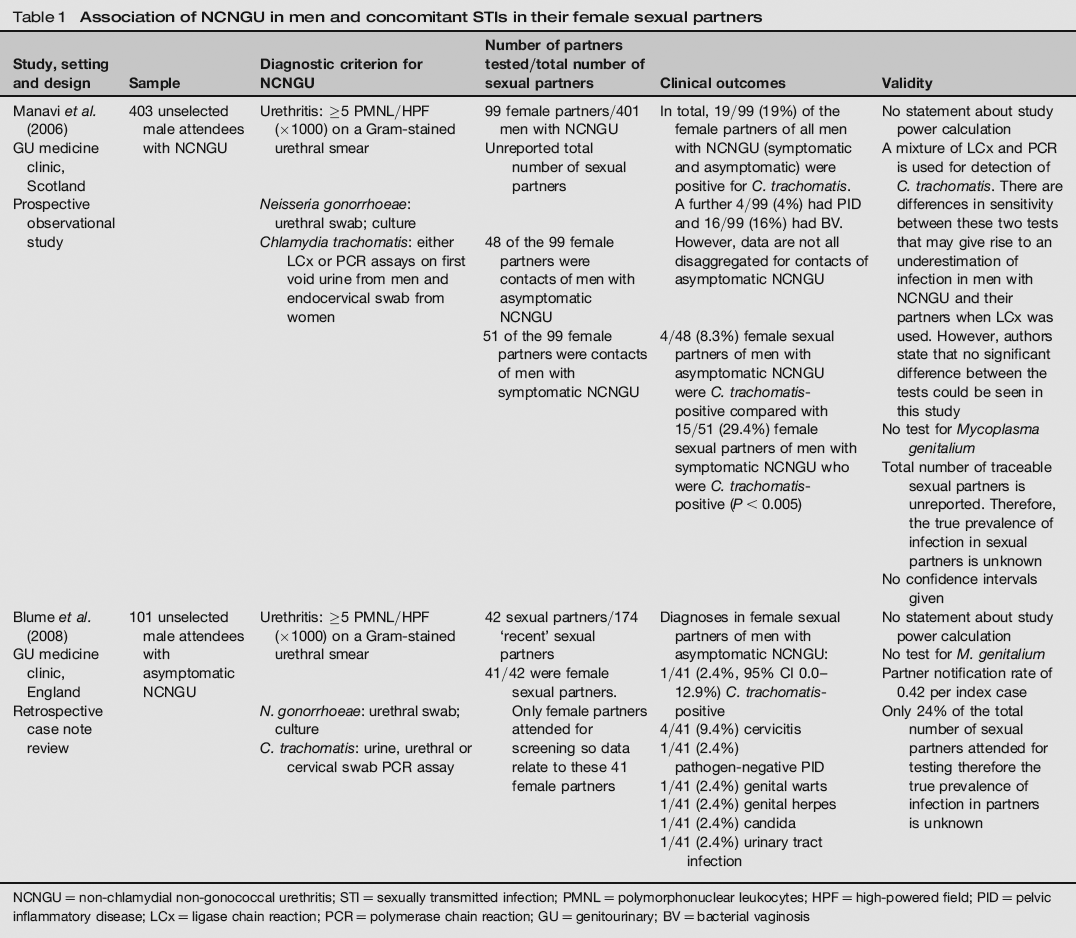
NCNGU = non-chlamydial non-gonococcal urethritis; STI = sexually transmitted infection; PMNL= polymorphonuclear leukocytes; HPF= high-powered field; PID = pelvic inflammatory disease; LCx = ligase chain reaction; PCR = polymerase chain reaction; GU = genitourinary; BV = bacterial vaginosis
Discussion
We identified only two studies that met the inclusion criteria for our review. The available research in this area, on which clinical guidelines are based, is insufficient in quality and breadth to enable us to draw robust conclusions on whether asymptomatic NCNGU is associated with significant health consequences for men or their sexual partners.
Where literature exists, consequences for sexual partners focus on the diagnosis of concomitant STIs in female partners.26,27 The prevalence of C. trachomatis in these women ranges from 2.4% 27 to 8.3%. 26 A single study also found PID in 2.4% and cervicitis in 9.4% of sexual partners who were negative for C. trachomatis and N. gonorrhoeae? 7 It is possible that these women had false-negative results or M. genitalium-positive disease. While the identification of men with asymptomatic NCNGU may allow for contact tracing and discovery of STIs in sexual partners, the prevalence of C. trachomatis seen in female partners is no higher than would be reasonably expected in the general sexually active population. 28 It is difficult to know whether the prevalence of pathogen-negative PID and cervicitis detected is significantly different from the background prevalence.
Whether or not it is beneficial in public health and economic terms to redirect resources from screening asymptomatic men for NCNGU to specific STI screening programmes is unknown; no studies investigating these important issues were identified. We did not find any studies that investigated the effects of asymptomatic NCNGU on men with the condition. In particular, none addressing the psychosocial impact of asymptomatic NCNGU were found and no articles investigating the effect of asymptomatic NCNGU on HIV seminal plasma viral load were eligible for inclusion.
The studies included in this review have a number of important limitations. The total number of contactable sexual partners is only reported in the study by Blume et al 27 and the prevalence of infection is presented as the number of infections found in the partners attending for testing. This gives an incomplete picture of partner pathology and it is not possible to calculate the true prevalence of infection in partners without testing all sexual contacts. Neither of the included studies report whether a power calculation was performed to guide their sample size. Studies tend to include small numbers of index men and even smaller numbers of sexual partners which, again, may give rise to a false estimate of the true burden of disease in both male index cases and their sexual partners. The included studies did not apply standardized time periods between the index man last passing urine and the urethral swabs being taken. This is known to influence the yield of PMNLs per high-powered field. 29 There is also significant intra- and inter-observer variability in reading urethral smear Gram stains.30,31 The epidemiology of infections will vary between the geographical locations of studies (Scotland and south England) and when they were conducted (between 2002 and 2007), meaning that findings are not directly transferable to current populations.
There are several limitations of the review itself. While we only included studies that give an explicit definition of microscopic urethritis (≥5 PMNL/hpf averaged over 5 fields), some studies used a higher PMNL threshold. This means that men with a lower ‘grade’ of urethritis may not be included, leading in turn to an over-representation of symptomatic men. The definition of asymptomatic is difficult to standardize across the studies. Men who self-report as asymptomatic may have signs of infection when examined or may have been symptomatic in the recent past. Studies not published in English were not included for practical reasons and ongoing trials may be occurring which are not on the NIHR database. It is possible that among the large number of studies on NCNGU we have missed relevant results. However, we feel that it is unlikely that we have missed significant, well-conducted, appropriately powered studies investigating clinical consequences of asymptomatic NCNGU.
Finally, it is important to highlight that this review is focused on whether asymptomatic NCNGU is associated with adverse health outcomes. Organisms such as M. genitalium are responsible for some cases of asymptomatic NCNGU and there is an increasing body of literature to support its role in genital tract pathology in women.8,32 Therefore, a review looking at clinical consequences of asymptomatic M. genitalium-positive NCNGU may have different findings. As current provision within UK sexual health services does not provide for M. genitalium testing, we feel that the clinical question of relevance is whether or not asymptomatic NCNGU has significant clinical consequences, not whether M. genitalium-positive NCNGU has significant clinical consequences. The development of more sensitive microarrays may also find associations between other organisms not currently thought relevant and NCNGU. Again, the clinical consequences of this are currently unknown.
This review highlights the paucity of high-quality literature and lack of knowledge about asymptomatic NCNGU. The two studies identified for inclusion report rates of infection in female partners of men with this condition that are no higher than expected in the general population. However, it is important to consider the limitations of these studies when drawing conclusions about the significance of asymptomatic NCNGU and whether screening men is a useful clinical strategy. What is clearer is that current clinical guidelines are based on a limited evidence base. We feel it is unlikely that there will be any significant research into the implications of asymptomatic NCNGU in the future although we would argue that well-designed prospective studies with good follow-up of men and their partners are needed in order to better inform clinical practice. We are currently undertaking modelling work into the public health and economic implications of abandoning urethral microscopy in asymptomatic men based on assumptions around the prevalence of M. genitalium and its potential pathogenicity. We are also investigating the clinical and behavioural factors associated with a diagnosis of asymptomatic NCNGU in men attending sexual health services in order to identify whether these men are at risk of other STIs.