
Abstract
Sexual difficulties are common in people attending genitourinary (GU) medicine/HIV services and many would like professional help. Here, we report the results of the BASHH Special Interest Group in Sexual Dysfunction (SD) survey on the level and type of SD service provision within UK GU medicine services in 2007. Many clinicians expressed an interest in SD, however, only 25% of GU medicine clinics provide a designated SD service. Marked regional variation in the level of service provision was highlighted. Lack of resources and other pressures on GU medicine services, notably 48-h access, are barriers to SD service development. In spite of these constraints, we argue that GU medicine clinics are a highly appropriate place to treat SD.
Introduction
Sexual difficulties are common in people attending genitourinary (GU) medicine 1 /HIV 2 8 services and many would like professional help. Here we report the results of the BASHH Special Interest Group in Sexual Dysfunction (SD) survey on the level and type of SD service provision within UK GU medicine services in 2007. We have sought to identify existing SD services and determine whether provision is in the form of specialist SD clinics, or whether patients who present to GU medicine with SD are managed as part of the GU medicine clinic workload. Clinicians’ views on the provision of SD services in GU medicine are reported.
Further, the recent increased media coverage of women SD and European licensing of the trans-dermal testosterone patch, Intrinsa® (Proctor & Gamble Inc),9,10 for the management of low sexual desire in surgically menopausal women on concomitant oestrogen therapy, prompted specific enquiry into the management of female SD in GU medicine clinics.
Method
A postal survey of the 273 UK and Eire GU medicine clinics listed in the British Association for Sexual Health and HIV (BASHH) clinic directory was conducted in February 2007. A brief questionnaire was circulated to the lead clinician at each clinic.
Results
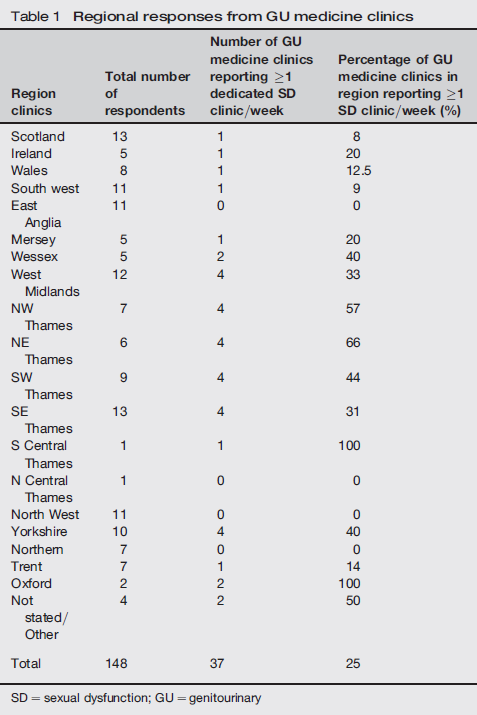
Regional responses from GU medicine clinics
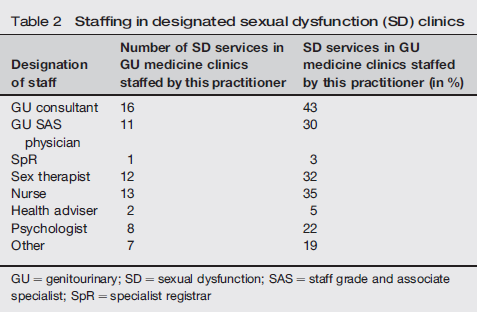
Staffing in designated sexual dysfunction (SD) clinics
Provision of care for patients who present to GU medicine with sexual dysfunction

A range of psychological interventions including brief counselling, cognitive behavioural therapy, psychosexual therapy, integrated therapy and hypnosis are provided by some GU medicine and SD services. A total of 26% clinics prescribe pharmacological treatments in SD management.
Clinician's comments revealed interest in the management of SD within GU medicine clinics; however, a number of common factors arose as inhibitors to service development: GU medicine service priority given to achieve 48-h access (raised by 13 respondents); lack of funding inhibiting service development (raised by 22 respondents); lack of staff trained in management of SD. Existing links with other services were identified in some areas. Ad hoc provision by GU medicine physicians with a special interest and training in management of SD was apparent. Two respondents questioned the role of GU medicine in SD management and one stated that management of SD was not his/her job.
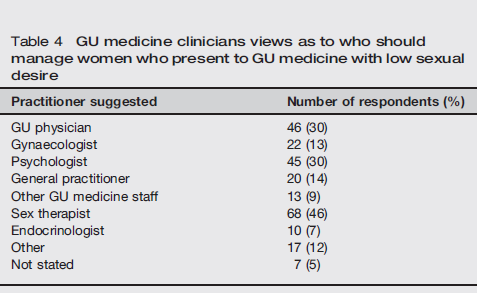
GU medicine clinicians views as to who should manage women who present to GU medicine with low sexual desire
A total of 53% of responding clinicians held the opinion that medication should be considered in the management of women complaining of low sexual desire; some commenting that this would depend on the context, results of investigations or fulfilment of criteria and would not be their first line management. A range of pharmacological agents including hormonal and antidepressant preparations was suggested. Twenty-one percent would prescribe Intrinsa® at least occasionally for women who complain of low sexual desire. The need for product information and fully informed patient consent was emphasized. Forty percent were unsure about prescribing Intrinsa®, expressing their need for more information about efficacy, evidence base, definitions and treatment criteria. Reasons for not prescribing included lack of funding, inexperience or the opinion that low sexual desire should not be managed in GU medicine.
Discussion
Wide disparity in the level of service provision in UK and Eire GU medicine services is apparent, possibly reflecting the local funding arrangements and the interest, training and skills of individual practitioners. Twenty five percent of GU medicine services hold at least one designated SD clinic per week. A variety of interventions are provided by multidisciplinary staff at these clinics. Some SD clinics are separately funded from GU medicine, some accept referrals from primary care others do not. Some services offer an integrated model of sexual health service provision encompassing GU medicine, family planning and SD services; these services report inadequate funding for the large number of patients presenting with sexual difficulties.
Widespread interest in SD by GU medicine physicians, with a desire by some to extend their service provision, has been highlighted; however, other pressures on GU medicine services, in particular 48-h access, often take precedence. Lack of funding inhibits service development and has resulted in the closure of clinics in some areas. Some interested and experienced clinicians continue to provide ad hoc care on a voluntary basis to GU medicine/HIV patients. Lack of qualified personnel and opportunities for training are additional barriers to service provision, as previously reported.1,11–14
While effective links with existing SD services that facilitate patient access have been identified, some with integrated care pathways and shared care protocols, in many areas inadequate provision is reported. The lack of equitable access to specialist services demonstrated by this survey, falls short of UK recommended standards. 15
There is a high rate of SD in the UK. In a population study, 35% of men and 54% of women admitted they had a SD problem for one month or more over the previous year. 16 That study showed that a majority of those who sought help for these did so via their GPs. Whereas in central London a third of GPs felt competent to deal with SD issues, 17 in the provinces GPs and practice nurses may not address sexual health issues proactively with patients. 18 Particular barriers to discussing sexual issues were: if the patient was of the opposite gender; middle aged or elderly; from black or ethnic minorities or non-heterosexual. Constraints of time and lack of expertise were also deemed important. Other researchers have found that physicians in general consider personal embarrassment an obstacle to initiating discussions on female SD. 19 Whereas only 9% of men and 5% of women in the UK population study sought help for their SD at GU medicine clinics, 20 GU physicians are ideally placed to handle SD for a number of reasons e.g. they are good at taking sexual histories and examining genitalia. 21 SD in men is primarily (but not exclusively) associated with organic problems such as hypertension, diabetes and recent STI diagnoses.16,22 In women, having small children, relationship issues, anxiety and depression appear to be the major issues associated with SD.16,22 Similar issues appear to obtain for HIV positive women with SD. 23 Handling the psychological issues are already being undertaken by some sex therapists and psychologists in the GU setting; as evidenced by the results of our current study. The major barrier to this would appear to be funding; a recurrent theme highlighted by many respondents. Further indirect evidence of this is that currently only 25% of clinics have a SD service compared with over 40% in 1997 and 2001.12,14 These studies supported the notion that GU physicians were very supportive of the idea of having SD clinics; over 80% endorsing this idea.
Intrinsa®, a testosterone patch used for surgically menopausal women with low sexual desire has recently been in the news. 9 Hitherto, in spite of low sexual desire being the commonest SD among both men and women, it appears women have been reluctant to come forward for treatment. More specifically 41% of women in a UK population study admitted to low sexual desire for one or more months over the past year, with 10% saying they had the problem for six or more months over the past year. 22 However, only a proportion of these women are distressed about their condition (between 9 and 26% of those who complain of low desire in the USA 24 ). Such women are now, in the light of the heightened media interest, more likely to present to health care professionals. Our current study suggests that women are already presenting to GU clinics with this problem, and that their physicians feel they would like more information regarding specific therapy (Intrinsa®), which may be helpful under certain circumstances. An important issue is that unlike medications such as Viagra, medications to help low desire in women will have to be given in conjunction with psychological therapies to ensure reasonable therapeutic outcome. 25 This is a particular issue as the efficacy of Intrinsa® in post-menopausal women with low desire, in terms of satisfactory sexual events (compared to sexual desire outcome for example) appears to be marginal. 26
CONCLUSION
There is inequity in SD service provision by GU medicine clinics across UK and Eire. While 25% clinics surveyed hold at least one designated SD clinic per week, ad hoc provision for selective sexual problems is available in many others for patients who present directly to these services. A variety of models of service provision have been identified where professionals from multidisciplinary backgrounds are involved in the identification, assessment and treatment of SD. This holds implications for education and training. Pressures on GU medicine services, especially 48-h access, compound lack of resources both financial and personnel, as barriers to service development. In spite of this, we argue, departments of GU medicine may be an ideal setting to manage patients with SD.