
Abstract
This study reports the first EU-wide survey of community-based voluntary counselling and testing services (CBVCTs), with the following aims: to assess the current availability of CBVCTs and how the concept of CBVCT is understood; to describe CBVCT modalities and strategies; and to measure the use of rapid tests within CBVCTs. A cross-sectional survey was conducted in two different key informant groups: HIV/AIDS National Focal Points (NFPs) and CBVCTs from the EU and European Free Trade Association (EFTA) countries. A definition of CBVCTs was reached. Descriptive and correspondence analyses were performed. The COBATEST survey was answered by NFPs from 25 of the 32 EU/EFTA countries (response rate of 78.1%), and by 55 CBVCTs in 22 different countries. CBVCTs were functioning in nearly all the responding countries, but only 56% explicitly included them in their national strategic plans. In those that had CBVCTs, the NFPs often lacked reliable information on CBVCTs. In general, CBVCTs in Europe are focused mainly on men who have sex with men, are primarily peer-driven and highly communitarised, whereas CBVCTs targeting other at-risk populations are more medicalised. In addition, the oral test is under-used and in general test performance is highly medicalised. Results show that there is a wide heterogeneity of CBVCTs in Europe, which is varied and highly medicalised. The data provided in this study in conjunction with other deliverables produced by the COBATEST project should contribute to the development of standardised indicators to enable comparisons over time and eventually improve the effectiveness of CBVCTs across Europe.
Keywords
Introduction
HIV infection remains of major public health importance in Europe. In 2013, 136,235 new HIV infections were diagnosed in 51 of the 53 countries of the WHO European Region, giving a rate of 15.7 per 100,000 population. 1 These data suggests continuing HIV transmission in many countries and that HIV remains concentrated in key populations at higher risk, such as men who have sex with men (MSM); people originating from high-endemic countries and people who inject drugs (PWID). 1 Moreover, late presentation is also a significant issue in all HIV exposure groups across Europe, 2 although with regional variations. 3 The persistent high prevalence of late presentation has been explained in most European regions as due, among other factors, to significant barriers to effective HIV testing. 4
Early diagnosis and treatment have been shown to be beneficial for both the individual and the community and are therefore a critical public health priority. 4 With early diagnosis and treatment, an HIV-infected individual experiences lower morbidity, mortality and increased treatment effectiveness.5–7 Consequently, antiretroviral treatment (ART) reduces the HIV viral load, reducing an individual’s risk of HIV transmission. Hence, community benefits are principally due to lower transmission rates in people diagnosed early, because of both lower infectivity on ART, coupled with changes in sexual and drug injecting behaviours after diagnosis.8,9 To encourage early diagnosis of HIV infection and decrease the proportion of infected people who are undiagnosed, there has been a policy shift towards expanded HIV testing. These policies encourage the promotion of community-based voluntary counselling and testing services (CBVCTs) and the use of rapid testing technologies.4,10
CBVCTs have been described in the literature as effective providers of HIV testing and counselling (HTC), 11 with high acceptability and uptake of HIV testing. Also, CBVCTs help build public trust, protect human rights and reduce stigma and discrimination, 12 target one or more specific populations, including MSM, migrants, PWID and young people, 4 and contribute to the removal of structural, logistic and social barriers to HTC. 12
Despite laws and recommendations applying to HIV testing being enacted in all European countries, national policies and guidelines about HIV screening often differ by country 13 and little is known about specific policies on targeted HIV screening of different sub-populations and the role of CBVCTs.13,14 In 2009, the European Commission highlighted the need to promote early diagnosis through ‘Community Action in the Field of Public Health Work Plan 2009’ 10 and in 2010, WHO Europe aimed to increase access to HTC both within and outside health facilities, in order to respond to the particular needs and challenges faced by the region. 15
In line with those recommendations, the HIV-COBATEST project was implemented from 2010 to 2012, co-funded by the Consumers, Health and Food Executive Agency (CHAFEA), under the EU Public Health Programme 2009–2013, in order to promote early diagnosis of HIV infection in Europe by improving the implementation and evaluation of community-based testing practices. The objectives of this study are to assess the current availability of the CBVCTs, to understand how the concept of CBVCT is translated into practice, to describe CBVCT typologies, modalities and strategies and to assess the use of rapid technologies within CBVCTs.
Methods
A cross-sectional survey was conducted in two different key informant groups: HIV/AIDS national focal points (NFPs) and CBVCTs from the EU and European Free Trade Association (EFTA) countries (32). The NFPs are the main points of contact at national level, including; Ministries of Health, HIV surveillance centres and HIV programmes, whereas CBVCTs were mainly comprised of non-governmental organizations (NGOs), HIV/sexually transmitted infections (STI) programmes and health institutions that managed or participated actively in the CBVCTs. The NFPs were identified and contacted directly by the study group through e-mail. NFPs were asked to identify the relevant regional focal points (if any) and the persons directly responsible for the management of individual CBVCTs and to send the resulting list of contacts to the coordinating centre of this study. The CBVCTs were identified in three ways: first, by the list sent by the NFPs; second, through the mailing list of the NGOs partnership on HIV and AIDS in Europe and Central Asia (AIDS Action Europe) and third, by the information provided by the associated and collaborating partners of the HIV COBATEST Project. The Civil Society Forum, CHAFEA and the European Aids Treatment Group (EATG) were also consulted to help identify possible CBVCTs respondents in the European countries. Data collection was conducted from December 2011 to February 2012. The minimum accepted response rate for the NFPs was set at 65% of participating countries. Since it was not possible to calculate an estimated sample size of CBVCTs, the aim of the survey was to collect information from the highest possible number of services, in order to create as inclusive an opportunistic list as possible, not construct a statistically significant sample.
As a standard definition of CBVCT was not available in the literature, a definition of CBVCT was reached by consensus through an expert meeting held in October 2010 in Luxembourg with representatives of the European Centre for Disease Prevention and Control (ECDC); CHAFEA; National HIV surveillance and Public Health Institutes from different European countries; university research groups on HIV; European CBVCT managers; EATG; Civil Society Forum and representatives of civil society. The definition used was aimed as being as much inclusive as possible, and it has incorporated both an operational (outside the health settings) and a principle (community involvement) component. The final definition for CBVCTs was agreed by all participating countries to be as follows: ‘CBVCT is any programme or service that offers HIV counselling and testing on a voluntary basis outside formal health facilities and that has been designed to target specific groups of the population most at risk and is clearly adapted for and accessible to those communities. Moreover, these services should ensure the active participation of the community with the involvement of community representatives either in planning or implementing HIV testing interventions and strategies’.
Data were collected using two piloted, semi-structured and self-administered tools, one for NFPs and the other for CBVCTs. The questionnaires were adapted,16–18 and adjusted to the consensus definition. The questionnaire directed at NFPs contained 35 questions. Topics covered were related to HTC policies, CBVCT implementation and resources, testing methods and guidelines, referral procedures, data reporting and evaluation processes. The CBVCTs questionnaire was addressed to persons directly responsible for the management of the CBVCTs and included 45 questions related to the type of facility, settings, kind of involvement of the community, testing methods, target groups reached, test fees, accessibility, privacy and confidentiality of HTC and linkage to care. Both questionnaires were sent electronically and were returned via e-mail to the data manager.
Settings were defined as: (a) outreach setting: refers to the provision of HTC in the community without having a structural fixed facility, including caravans and mobile units; (b) venue setting refers to saunas, discos, bathhouses, etc. that serve as venues where HIV testing can be performed; (c) NGO refers to the headquarters of non-governmental organisations that perform initiated (routine) and client-initiated (voluntary) HIV/AIDS testing programmes and (d) health care settings include, but are not limited to, acute-care hospitals; physicians’ offices; urgent-care centres and outpatient clinics.
Both descriptive and correspondence analyses were performed. The latter statistical method was performed with the data collected from the 55 CBVCTs, and used in order to define recurrent typologies in order to discriminate between general and specific concepts of CBVCTs. A model was constructed with different sets of variables. The first set included variables that describe the ‘community’ as setting, as resource and as agent (modalities: staff performing rapid test in a scale from ‘complete medicalisation’, where only physicians or nurse are involved, to ‘complete communitarization’, where only peer-educators are involved). The second set comprised two specific variables: opening time at night and confirmation test provided directly at the CBVCTs. In the third set were variables that defined the community as target, starting with MSM, adding stepwise modalities such as PWIDs, sex workers (SW), migrants and young people. Two dimensions were identified; one formed by modalities defining the community as target or resource and called ‘community issues’, the other formed by modalities which contribute to the definition of the setting called ‘organisational issues’.
In order to summarise the degree of community involvement allowed in the procedures and activities of the CBVCTs (rapid test performance, blood taking, pre- and post-test counselling) in Europe, a 5-score scale was constructed directly with the data collected from the NFPs surveys. The scale was constructed as follows: Score.1, ‘complete medicalisation’ when only physicians and/or nurses are involved in the activity; Score.2, as for score.1 but when other psychosocial professionals such as psychologist or social workers are allowed to perform the activity; Score.3, as for Score.2 but with the involvement of peer counsellors, regardless of professional status; Score.4, activities performed only by psychosocial professionals or peer counsellors without the involvement of medical professionals (physicians and/or nurses); Score.5, ‘complete communitarization’ only peer counsellors are involved. Statistical analyses were performed using Stata Statistical Software: Release 11 (Stata Corp Ltd., College Station, TX, USA).
Results
Settings where CBVCT is performed, according to NFPs and CBVCTs, by country (2010–2012).
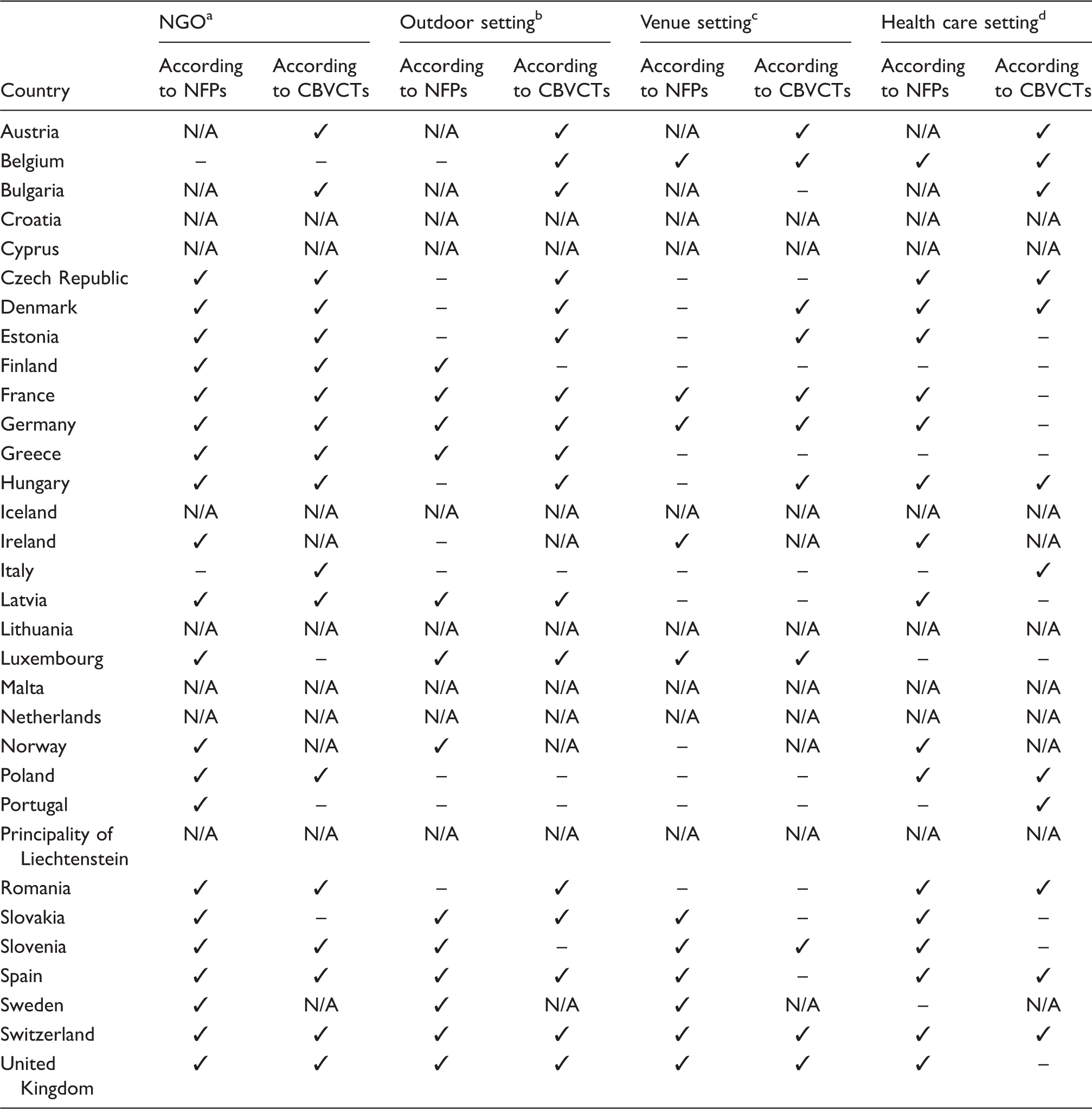
Note: The main characteristics of the 55 participating CBVCTs were: 91% were NGOs; 50% were co-founded by public and private sectors; 84% were focused on men who have sex with men (MSM); and 49% on people who inject drugs (PWID).
NFP: national focal points; CBVCTs: community-based voluntary counselling and testing services; NGO: non-governmental organisation; N/A: not applicable, which means that the survey was sent to the NFP and the CBVCTs, but no answer was received.
Outreach setting: refers to the provision of HIV counselling and testing in the community without having a structural fixed facility, this includes caravans and mobile units.
Venue setting refers to saunas, discos, bathhouses, etc. that serve as venues where HIV testing can be performed.
NGO refers to the headquarters of non-governmental organisations that perform initiated (routine) and client initiated (voluntary) HIV/AIDS testing programmes.
Health care settings include, but are not limited to, acute-care hospitals; physicians’ offices; urgent-care centres and outpatient clinics.
Nearly all NFPs from the participating countries reported that CBVCT implementation was included in their national strategic plans; although only 56% (13/25) of these had drawn up specific strategic plans covering CBVCTs. Eighty percent of NFPs in the 25 participating countries reported the actual operation of CBVCTs, despite these strategic plans.
Figure 1(a) shows information reported by the NFPs related to fees that were charged to get tested in the public health system and describes that testing was offered in nearly all health care settings and in 48% (12/25), the test was free of charge. Although, Belgium and Estonia required valid health insurance for testing and in Switzerland fees are charged unless the person cannot afford it. Furthermore, where rapid HIV testing was recommended by official guidelines, 64% (16/25) recommended using blood and 24% (6/25) oral fluid. Figure 1(b) and (c), shows that the HIV test most used by CBVCTs was rapid testing using finger prick (73% [18/25]), followed by conventional tests requiring venepuncture (45% (11/25)). The use of rapid blood HIV test through finger prick was reported by the large majority of the CBVCTs (73% [40/55]) and only 4% (2/55) of CBVCTs reported using oral fluid in rapid tests. Of the CBVCTs offering rapid HIV testing, 45% (19/42) directly requested confirmatory tests to the reference laboratory. When confirmatory test was performed in the CBVCT service (25 CBVCTs), test strategies changed: almost half of the CBVCTs (51%) used Western Blots, 22% used Elisa, 4% used a second rapid test and the other 8% did not know. Requirement of informed consent was reported by almost all responding CBVCTs (91%). In most of the participating services, the required informed consent was only oral (65%), and the minimum age for being tested for HIV in the CBVCTs without parental consent varies between countries, ranging from 14 to 18 years old.
Data provided by the NFPs on: 1(a) Whether HIV testing is free of charge in the public health system; (b) Whether rapid HIV tests on oral fluid are officially accepted and/or recommended and 1(c) Whether rapid HIV tests on blood are officially accepted and/or recommended, by country. NFPs: national focal points.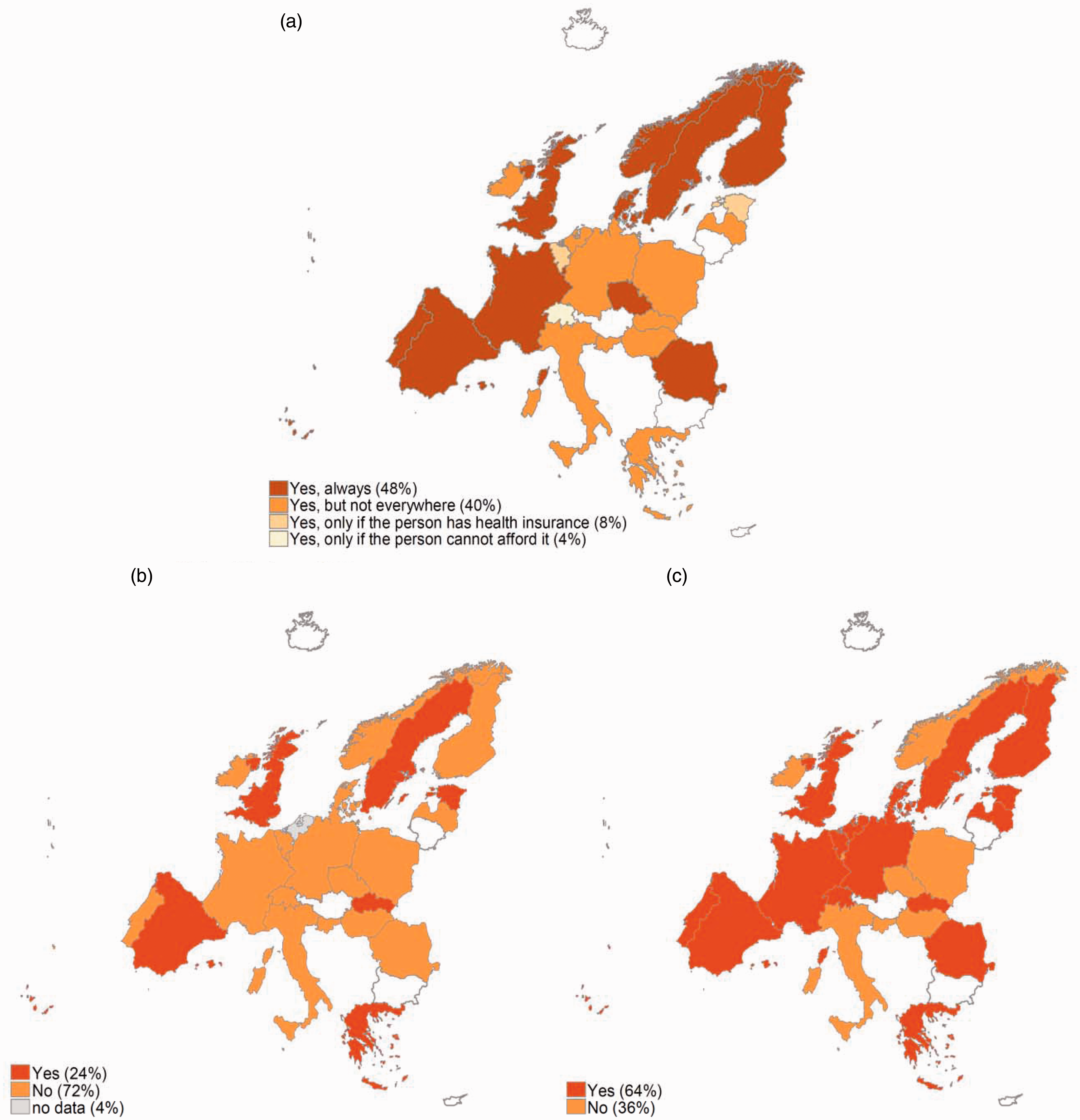
Professionals allowed to provide counselling or to perform rapid testing, according to national focal points and community-based voluntary counselling and testing services, (2010–2012).
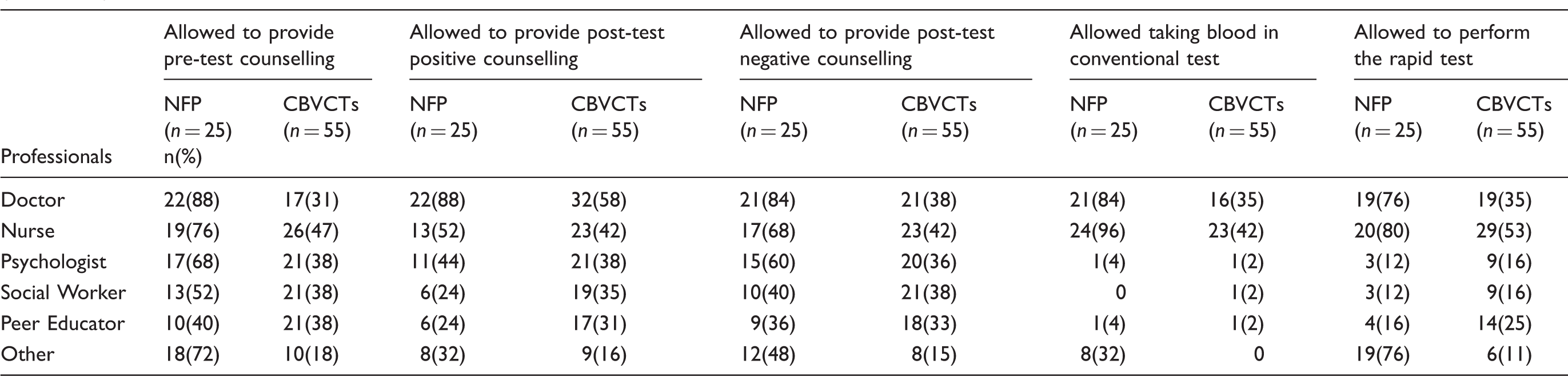
NFP: national focal point; CBVCTs: community-based voluntary counselling and testing services.
Figure 2 shows the scale of medicalisation or communitarisation of rapid HIV testing according to the NFPs. Rapid testing is completely medicalised in 53% (13/25) of the countries, and only in 13% (3/25) is it completely communitarised. According to the scale, pre-test and post-test negative counselling are done mainly by peer educators, psychologists and social workers whereas the post-test positive counselling is done mainly by physicians and nurses; in 48% (12/25) of the reported positive cases, post-test counselling was done by physicians.
Data provided by the NFPs on the degree of community involvement in the provision of community-based voluntary CBVCTs in different European countries, stratified by a five score scale ‘staff involvement approach’. Scale applied to 2(a) Rapid test; 2(b) Pre-test counselling; 2(c) Post-test negative counselling and 2(d) Post-test positive counselling. NFPs: national focal points; CBVCTs: community-based voluntary counselling and testing services.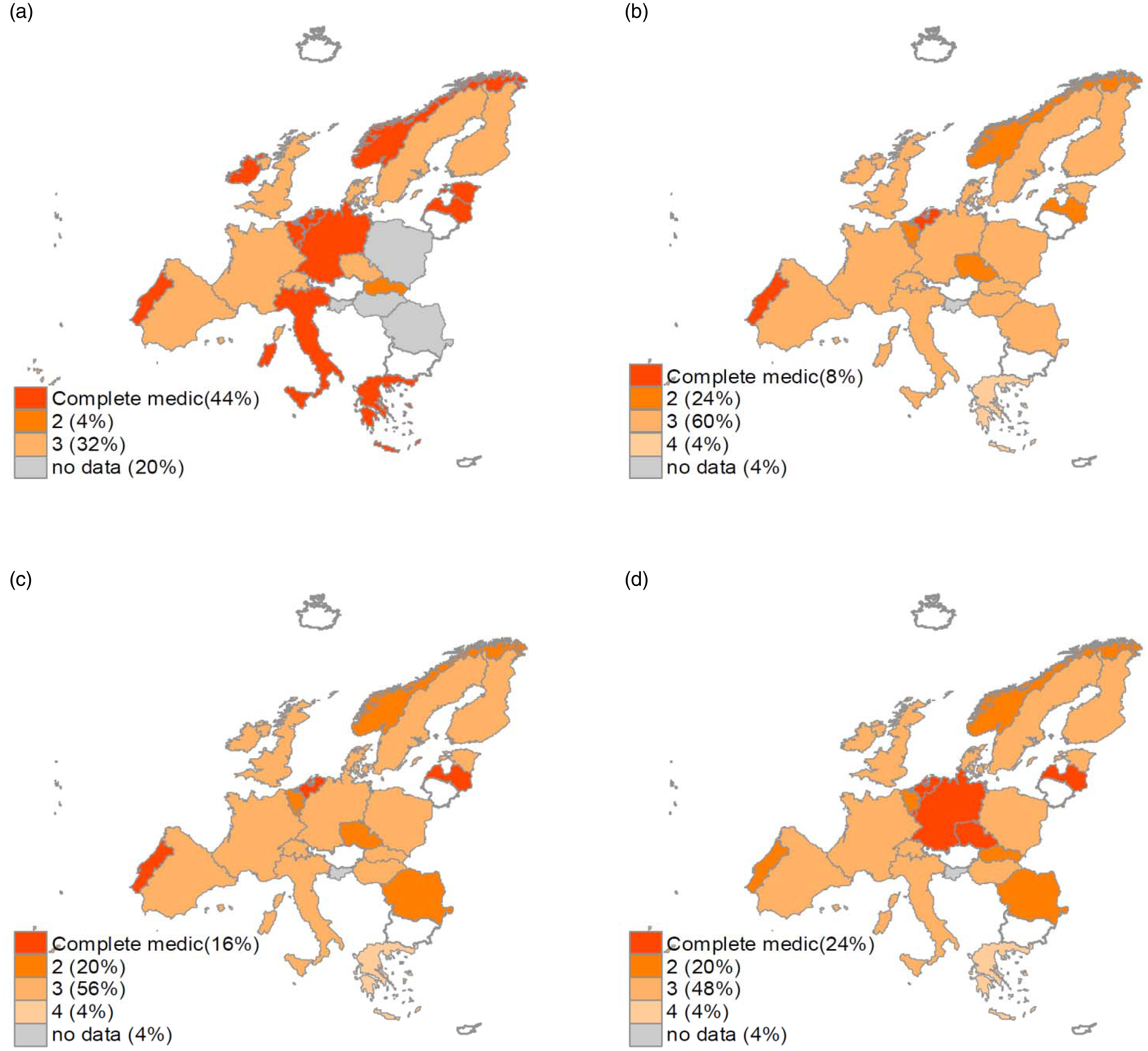
Almost all CBVCTs (91% [50/55]) reported being exclusively managed by NGOs. In only five cases in different countries (Belgium, Poland, Czech Republic, Italy and Switzerland) the CBVCT was managed by a public body. However, when the focus is shifted towards community involvement, direct community management is reported only by 27% (15/55) of the participating CBVCTs. All 15 CBVCTs with both NGO and community management are targeting MSM.
Less than half of NFPs (44% [11/25]) reported that the CBVCTs in their countries systematically report their activities to the local Public Health authorities. The majority of the CBVCTs, however, (88% [48/55]) reported that all new cases of HIV diagnosed were referred to the National Health System, and 94% (52/55) had access to direct referral processes to a specialised HIV clinical setting for treatment and care. Most of the CBVCTs (84% [46/55]) reported having formal agreements with the health system and 71% (39/55) with a specific protocol to accompany people who tested positive.
From the correspondence analysis (Figure 3), the two dimensions (organisational and community issues) identified explained slightly more than 59% of the variance of the CVBTCs' typology. Four main forms of CBVCTs were identified: one with a strong community involvement, peer-driven, implemented in venue or NGO settings, managed by the community and usually targeting MSM; one characterised by a bigger role played by professionals such as psychologists and social workers, but where an NGO is present as a key ‘community representative’ and where work and settings (NGO settings or outdoor settings) are organised in order to meet the needs of the target population, mainly PWIDs, SWs and migrants; one characterised by the role of the health care setting, where the term ‘community-based’ is characterised by some kind of needs assessment of the target population (mainly young people) together with some level of outreach activity. The fourth form was less clearly identifiable as ‘community-based’, characterised by full medicalisation of rapid testing, direct access to confirmatory tests and no community involvement in the procedures, this one was not focused on any particular target population.
Scatterplot of category points in the multiple correspondence analyses the data provided by the CBVCTs. Model with five target most at risk populations, MSM, PWID, SWs, migrants and young people). CBVCTs: community-based voluntary counselling and testing services; MSM: men who have sex with men; PWID: people who inject drugs; SWs: sexual workers.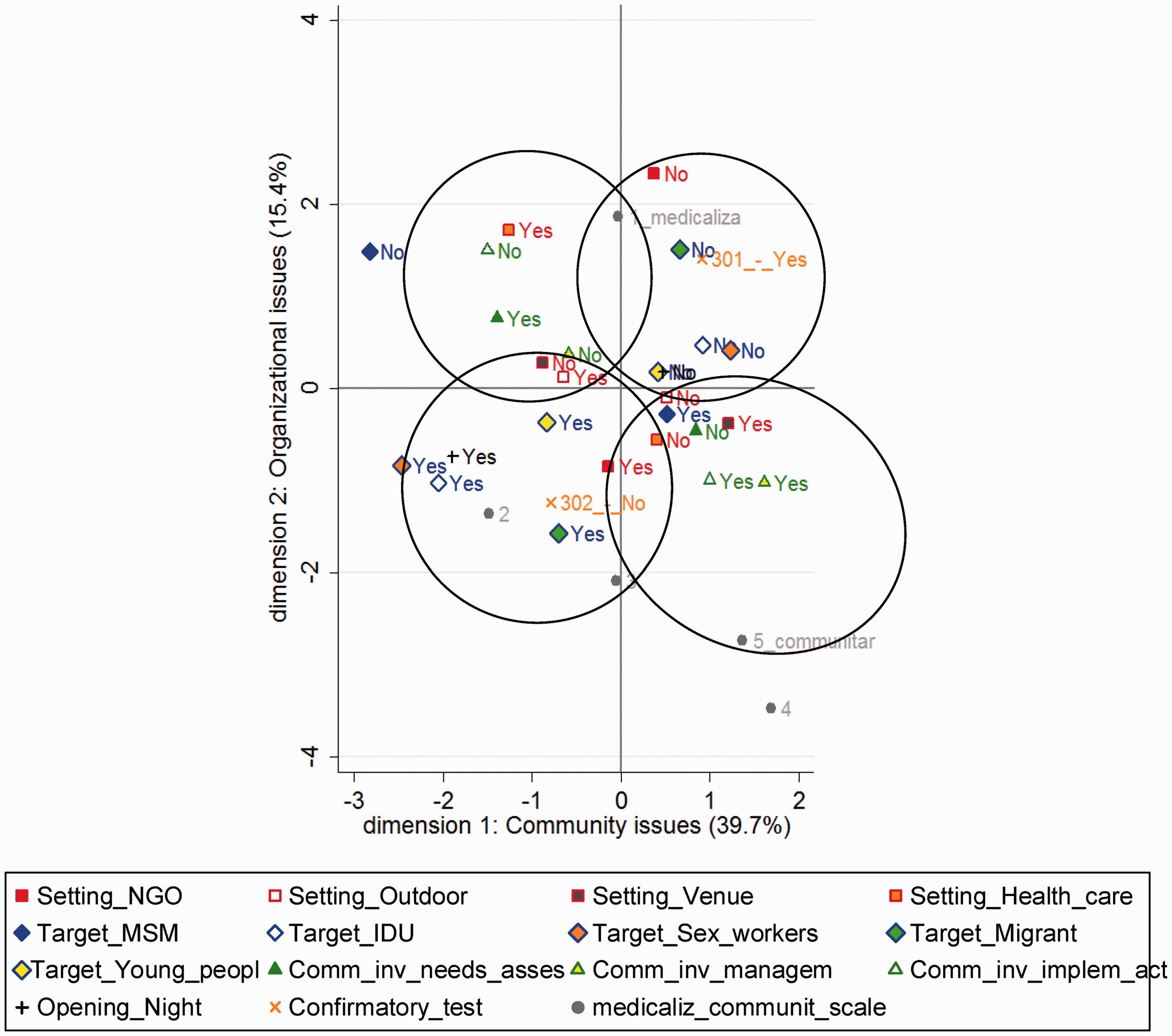
Discussion
This study shows that CBVCTs seem to be established in nearly all the responding European countries. However, only 56% of countries had specific strategic plans covering HIV testing in CBVCTs, and in those that had CBVCTs, the NFPs on HIV, especially in large countries, did not have reliable information on CBVCTs and programmes, which in many cases contradicted the information provided by existing CBVCTs. Overall, CBVCTs across Europe are mainly focused on MSM, with a typology of peer-driven, highly communitarised services. CBVCT targeting other at-risk populations tended to be more medicalised. In addition, the rapid oral test is under-used; and in general, the performance of the test at the CBVCTs is highly medicalised.
The CBVCT model is commonly recognised to improve access to early HIV diagnosis for most-at-risk populations. These centres are in an excellent position to improve all aspects of HTC including access, offer, uptake and effectiveness. 11 However, there was no agreed definition of CBVCT, leading to the definition that was proposed in this study; one of the first that tries to include the heterogeneity of CBVCTs across Europe.
A large number of definitions have been used in the literature to describe CBVCTs. One widely used describes CBVCTs as places that are based outside pre-existing traditional healthcare settings, and includes both standalone services, as well as venues primary used for other purposes where HIV testing is offered as additional service.11,19 This description is practical, grouping structured, formal testing sites from a geographical perspective, but leaves out more diffuse services that might be defined by the type of community involvement or the target population.20,21 The definition of CBVCTs that has been proposed in this study and has been well accepted by participating countries, was seeking to be inclusive of both formal organisational structures, as well as informal community initiatives which might not have any organisational (or physical) structure and are significantly more fluid in nature and do not fit easily into current classification systems. Nevertheless, this wide definition might result in a varied body of information that makes cross‐analysis and comparison difficult, reducing the room for research and evaluation processes. Therefore, effort should go into facilitating the development of common regulations, strategies and procedures (including standardised indicators), that would allow sharing of methodologies, data collection instruments and monitoring and evaluation tools, in order to ensure comparability across countries and between CBVCTs.
Community involvement seems to be very strong when members of the community are simultaneously the target of the service and also form part of the implementation and management staff. In line with other studies,11,19 this occurs mostly with the MSM population, characterising the service as strongly peer-driven, and where the main places to offer testing are NGOs. This approach has been demonstrated to be effective in attracting more MSM, especially those most exposed to at-risk situations and less likely to have been tested during the two previous years. 22 Also, when CBVCTs have a high community involvement targeting the general population, programmes are successful in reaching people early in the course of HIV infection and have higher uptake rates of HIV testing.19,23 Although in the literature there is no evidence of harm from being tested in CBVCTs by non-health care professionals, a recent report describes the possibility of false positive diagnosis in these settings, with lack of HIV test confirmation, poor training and supervision of community health workers and with insufficient quality control procedures. 24 This study also shows that there is often poor support from national structures, with just 28% having regulations in place to allow non-health professionals in CBVCTs to perform an HIV test. Consequently, countries should review their regulations and remove inappropriate obstacles to testing in community settings, create legal frameworks for non-health professionals performing activities in CBVCTs in concordance with validated testing algorithms and following the 5Cs of good testing practices (informed consent, confidentiality, counselling, correct test result, connection to prevention and ensure quality control and good linkage to health care system). 12
As regards to the use of testing technologies, our results showed that rapid tests are fairly recommended by countries guidelines, used by CBVCTs moderately on oral fluid and in general when it is performed is highly medicalised. The benefits of the use of rapid testing have been demonstrated in the literature, as they increase the likelihood of a person receiving their results,25,26 are highly acceptable to clients 27 and are advantageous in settings where venipuncture is not possible or where quick turnaround of test results is desirable.4,28 In line with the extant evidence, in Europe, the use of rapid test either on blood or oral fluid should be encouraged in CBVCTs. In order to improve their use, common legal frameworks for non-health professionals performing rapid tests should be developed and minimum pre-test information packages agreed.
This study gathers information never before collected that might help to describe the pattern of CBVCTs across Europe. Among the limitations of this study, we can mention that information collected by the HIV-COBATEST survey does not allow for an exhaustive picture of all CBVCTs operating in Europe, and the description of the CBVCTs might be biased by the characteristics of the participating CBVCTs, however, the collected information gives a first description of CBVCTs across Europe, and will complement qualitative studies and policy analysis. Second, it is important to keep in mind that NFPs completed the questionnaire to the best of their knowledge, but these were subjective assessments that may have underestimated the true extent of the complexity of CBVCTs in Europe. Finally, this is one of the first EU-wide surveys on CBVCTs and shows variability between countries with regard to regulations, typologies and use of new technologies. Our survey revealed that there is substantial gap between information managed by the NFPs and existing CBVCTs. However, data from the COBATEST survey should be analysed complementarily with data from the qualitative studies of the project as well as with data from other existing surveys to gain a more precise picture of the magnitude of CBVCTs in Europe.
In conclusion, this study represents the first attempt to define and describe community testing services at the European level and the definition used has allowed to include a wide typology of CBVCTs. Although it does not pretend to be representative of all of them, it has clearly shown the complexity and heterogeneity of the on going community testing programmes and services, ranging from pure outreach programmes to very medicalised services. The data provided in this study, in conjunction with other deliverables produced by the COBATEST Project, have allowed developing standardised indicators that will allow comparisons between strategies and geographical areas over time. The project has also helped to consolidate the concept of community testing and to speed up the actual implementation of this approach in some countries in which testing was performed exclusively within health settings. Although, since community testing has dramatically increased during the last two years, the data presented may not reflect the current situation of community testing in some countries, it is worthwhile to note that despite CBVCTs are being established in nearly all European countries, only a few had specific strategic plans and even in several countries with CBVCTs the NFPs on HIV had little information on them. Community testing may play an important role in HIV early diagnosis and treatment in Europe and it should be reflected as that in the National HIV Plans. Finally, in the near future, new technologies and Point of Care approaches will facilitate the improvement of the CBVCTs effectiveness in early detection of HIV and other STIs and its typology will further evolve; monitoring and evaluation tools like the Dublin Declaration needs to incorporate specific indicators aimed and measuring and improving the effectiveness of community testing in Europe.
Footnotes
Acknowledgements
The authors would like to acknowledge the European Commission, the Agencia de Salut Publica de Catalunya (ASPC) and Gilead Sciences Ltd, for their support. They are grateful to all the NFPs and CBVCTs who participated in the survey. They are also grateful to Colin Campbell for English revision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Consumers, Health and Food Executive Agency (CHAFEA) (former Executive Agency for Health and Consumers (EAHC)), under the EU Public Health Programme [Grant Agreement N° 2009 12 11].