
Abstract
Reactive arthritis may be caused by both sexually transmissible and enteric organisms, though Microsporidia is not currently recognised as a causative agent. This case report describes the development of reactive arthritis following Microsporidia infection in an immunocompetent man.
Case report
On the 6th of June a 24-year old UK-born heterosexual man presented to the Sydney Sexual Health Centre with three red macules on his penis, which had been first evident three months earlier but had transiently cleared for a period of three weeks after the patient applied an unknown cream.
The patient had been travelling for six months through India, Cambodia, Thailand, Singapore, Vietnam, Laos and Indonesia. Two weeks into his travels, whilst in India, he developed mild diarrhoea with some anal mucus and occasional cramping abdominal pain. He received no treatment for his gastrointestinal symptoms and the diarrhoea was persistent with some mild weight loss (Figure 1).
Sequence of clinical events.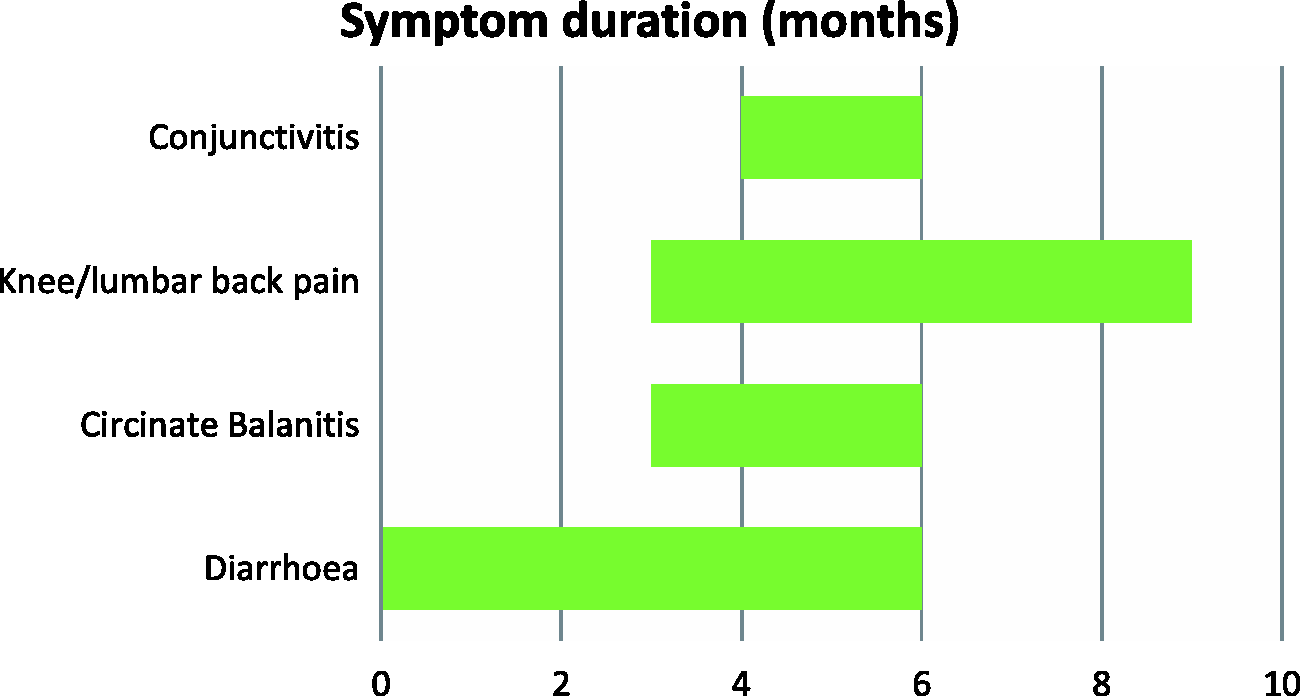
The patient reported a two-month history of conjunctivitis, worst in the mornings, but without pain or blurred vision. He received some unknown eye drops from a doctor in Vietnam. He also reported a three-month history of left knee and lumbar back pain, for which he was taking ibuprofen and paracetamol. He also reported muscular tenderness around the trapezius and intrascapular regions.
On examination on 6 June, he had an effusion of the left knee, a shallow dorsal tongue erosion and three lesions of circinate appearance on the glans penis. There was no urethritis or conjunctivitis evident on this date. When the patient presented for follow up on 21 June, there was conjunctivitis present on examination.
The patient reported no history of sexually transmitted infections and no unprotected sex for more than six months.
The patient was diagnosed with reactive arthritis and was referred for review by a rheumatologist and ophthalmologist. This confirmed the diagnosis, as they agreed that the eye signs and asymmetrical oligoarthritis were consistent with reactive arthritis.
On 15 June, the patient was prescribed 0.1% mometasone cream daily for treatment of balanitis, resulting in rapid symptomatic improvement.
Faecal microscopy with fluorescent staining showed spores of Microsporidia on three separate occasions, with no evidence of other bacterial growth and no cysts, ova or parasites visualised. A four-week course of albendazole 400 mg twice daily was prescribed on 18 June. This did not appear to relieve his symptoms.
Serology for HIV, syphilis and hepatitis C were negative, and the CD4 cell count was 780 cells/mm3. His full blood count and renal function were normal, with a slightly elevated C-reactive protein of 19 and a normal erythrocyte sedimentation rate. The patient was HLA-B27 positive, and rheumatoid factor and antinuclear antibodies were negative. Repeated urine polymerase chain reaction tests for chlamydia were negative.
Aspirate from the left knee showed inflammatory changes, without crystals. The patient received a joint injection of methylprednisolone on the 27th of June. The patient was treated with 400 mg of celecoxib twice daily initially. However, after a month of treatment to little effect, he began sulfasalazine at 500 mg daily increasing to 1 g twice daily.
Plain X-ray films of the lumbar spine, sacro-iliac joints and left knee were reported as normal.
The patient had an endoscopy and colonoscopy on the 11th of July. Warthin-Starry-stained sections showed no evidence of Microsporidia at this time. The patient was also diagnosed with post-infective irritable bowel syndrome, and possible minor distal inflammatory bowel disease.
The patient returned to the UK and was lost to follow-up the following February.
Discussion
This is the first report of reactive arthritis following Microsporidium infection. Microsporidia are single-celled obligate, intracellular protists closely related to fungi. Over the past 25 years, microsporidial infection has been recognised as an opportunistic infection primarily affecting patients with advanced HIV and other immunosuppressed individuals such as organ transplant recipients, cancer patients and diabetics. Among the immunocompetent, it has been known to affect children, travellers and the elderly. 1 Transmission in humans is thought to be primarily via the faecal-oral route; however, infection may also be caused by direct contact to the skin or eyes, trauma, vertical transmission or sexual transmission. 2
Clinically, diarrhoea and malabsorption are the most common symptoms of Microsporidia infection. However, microsporidial species may also cause keratoconjunctivitis, sinusitis, tracheobronchitis, encephalitis, nephritis, hepatitis, cholecystitis, osteomyelitis or myositis. 3
Reactive arthritis may be caused by sexually transmissible or enteric organisms. Salmonella, Shigella, Campylobacter and Yersinia species have been identified as causative agents in post-enteric reactive arthritis. 4
While microsporidial infection in an immune-competent patient is unusual, increased testing and improved testing methods are revealing a higher number of infections than previously. 1 This immune-competent patient may have had a genetic predisposition to developing symptoms of reactive arthritis due to his positive HLA-B27 status. 5 Due to its propensity to cause disseminated infection and a wide variety of clinical signs along with the difficulty with detection, it is possible that microsporidial infections are often under-diagnosed. 1 As reactive arthritis is thought to also be underdiagnosed, 5 this may offer some explanation as to why Microsporidia has never before been implicated in the development of reactive arthritis. That said, the temporal association between Microsporidia infection and reactive arthritis in this case could be coincidental rather than causal.
The patient had six months of symptoms and had not received any antimicrobial therapy prior to his presentation at the clinic, suggesting chronic infection. It has been suggested that chronic infection, such as chlamydia, may influence the development of reactive arthritis. 6 Based on the theory of chronic carriage, it is possible that chronic, rather than acute, infection with enteric pathogens such as Microsporidia may also play a role in the development of reactive arthritis.
Footnotes
Acknowledgements
The authors thank Dr Marcus Chen for his role in the patient’s care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.