
Abstract
Tuberculosis is recognised as one of the leading causes of severe sepsis among HIV-infected patients. Most patients with Mycobacterium tuberculosis bacteraemia have advanced HIV disease with CD4 counts less than 100 cells/μl and its presentation is non-specific in most instances. This was a cross-sectional study which was done by analyzing data from 201 adult HIV-infected patients who met the inclusion criteria for severe sepsis. The prevalence of Mycobacterium tuberculosis bactraemia in the study population was 34.8%. Severe sepsis caused by other etiologies was observed in 33 (16.4%) of the participants. Concomitant infection of Mycobacterium tuberculosis bactraemia with other organisms is not uncommon in patients with severe sepsis. This cohort of HIV-infected patients had severe immunosuppression with a median CD4 count of 51 (20–136) cells/μl with moderate anaemia, mean haemoglobin 8.0 (3.0) g/dl, and were generally underweight with a mean mid upper arm circumference (MUAC) of 21.0 (3.4) cm. Mycobacterium tuberculosis bacteraemia is very common in HIV-infected patients with advanced HIV disease who present with severe sepsis. Mycobacterium tuberculosis bacteraemia co-infection with aerobic organisms is not uncommon. Factors that were independently associated with Mycobacterium tuberculosis bacteraemia in our study population were MUAC and sodium level.
Introduction
Severe sepsis is one of the leading causes of death among hospitalized HIV-infected patients in sub-Saharan Africa. 1 Disseminated tuberculosis is recognised as one of the leading causes of severe sepsis among HIV-infected patients and significantly affects short-term and long-term survival among this population of patients.2–6
Mycobacterium tuberculosis bacteraemia may go unrecognised among febrile hospital patients in less-developed countries where both Mycobacterium tuberculosis and HIV are prevalent. 7 Many patients with disseminated tuberculosis and Mycobacterium tuberculosis bacteraemia have advanced HIV disease with CD4 counts less than 100 cells/μl and the typical signs and symptoms of pulmonary tuberculosis may not be present.7,18 Serious blood stream infections arising from other bacteria cannot be distinguished from Mycobacterium tuberculosis bacteraemia. Standard mycobacterium cultures may take four weeks to detect mycobacterium in blood and automated cultures may take 2–3 weeks, this contributes to delays in making the diagnosis Mycobacterium tuberculosis bacteraemia. 8 Subtle or unusual presentation of tuberculosis in HIV-infected patients with advanced disease coupled with lack of rapid diagnostic tests and laboratory capacity makes it difficult to diagnose tuberculosis in these patients who present with severe sepsis. Delays in making a diagnosis of Mycobacterium tuberculosis bacteraemia can lead to disease progression and outcome is poor.8,19,23
This study analyzed data from 201 HIV-infected patients admitted with severe sepsis at the University Teaching Hospital in Lusaka, Zambia, to determine clinical factors associated with Mycobacterium tuberculosis bactraemia in order to identify patients who may benefit from empirical anti-TB drugs.
Methodology
Study design
This study was a subgroup analysis of HIV-infected patient from two trials (Simplified Severe Sepsis Protocol [SSSP] and the Simplified Severe Sepsis Protocol-2 [SSSP-2]) plus other prospectively examined patients. The SSSP and SSSP-2 studies assessed the performance and cost of a simple treatment protocol, developed by the investigators, for severe sepsis. The protocol involved an algorithm of IV fluid administration with dopamine and blood transfusion for patients with persistent hypotension and severe anaemia, respectively. Two blood culture bottles were collected from each patient within one hour of admission, one for aerobic organisms and the other for Mycobacterium tuberculosis.
The SSSP and SSSP-2 studies were randomized controlled trials which were done at the Adult Emergency Medical unit of the University Teaching Hospital, the largest health institution in the country. The two studies had approval from the University of Zambia Biomedics Research Ethics Committee (UNZABREC) REF. Nos.: 009-08-11 for SSSP and 008-06-12 for SSSP-2.
This study had an independent approval from UNZABREC, REF. No: 001-02-13.
Study population
Patients above 18 years of age were screened and enrolled in the study from the Adult Medical Emergency Unit (AMEU) every day, during week days.
Inclusion criteria
Consenting HIV-infected adults (>18 years old) with a study-defined sepsis were included in the study. Severe sepsis was defined as suspected or confirmed infection with two or more of the SIRs criteria:9,10 axillary temperature >38 degrees or <36 degrees; heart rate >90 b/min, respiratory rate >20/min, leukocytosis >12,000 leukocytes/mm and one or more signs of end-organ dysfunction including hypotension defined as systolic blood pressure of ≤90 mmHg or a mean arterial pressure (MAP) of <65 mmHg, altered mental state, oliguria (urine <0.5 ml/kg/l), severe respiratory distress (respiratory rate >40/min), creatinine more than 120 μmol/l, hyperbilirubinaemia (total bilirubin >17 μmol/l) or thrombocytopenia (platelets <100,000 μ/l). All patients in the SSSP-2 study were required to have hypotension for inclusion.
Exclusion criteria
Patients were excluded from the SSSP and SSSP-2 studies if they had gastrointestinal bleeding, suspected renal or heart failure or if they required immediate surgery. Additionally, we excluded patients on treatment for tuberculosis and those with other causes of acute blood loss and those with history of blood transfusion in last three months.
Sample size
For the purpose of power calculation, we hypothesized that severe anaemia (Haemoglobin ≤7.0 g/dl) would be associated with Mycobacterium tuberculosis bacteraemia. A study of severe sepsis in Uganda found that approximately 20% of patients with Mycobacterium tuberculosis bacteraemia had severe anaemia. 11 In Malawi 43% of HIV-infected patients with severe anaemia had Mycobacterium tuberculosis. 12 Assuming severe anaemia was the exposure and Mycobacterium tuberculosis bacteraemia as the outcome, we calculated study power using OpenEpi software.
A minimum sample size of 205 patients would have a power of 80% with an alpha of 5% to detect 22% difference in Mycobacterium tuberculosis bacteraemia between those with and without severe anaemia. The final figure also allowed for a 10% attrition rate and for limited data or missing laboratory data.
Variables measured
The dependent variable for this study was the demonstration of Mycobacterium tuberculosis bacteraemia by a positive blood culture in HIV-infected patients with severe sepsis with a confirmatory MPT4 antigen test for Mycobacterium tuberculosis.
Independent variables measured include age and sex of the study participants, haemoglobin, CD4 count, CXR report, sputum microscopy result, mid upper arm circumference (MUAC), fever and cough of any duration. Biochemical variables included alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin, urea, creatinine and sodium.
The following are the definitions of some of the independent variables:
In this study severe anaemia was considered to be haemoglobin <7 g/dl, moderate anaemia as haemoglobin between 7 and 10 g/dl and anaemia as haemoglobin between 10 g/dl to normal limit for age and sex. 13 Wasting was defined as MUAC ≤20.0 cm and 19.0 cm for men and women, respectively, and corresponding to a body mass index (BMI) of <13.0. 14 This comes from the analysis and extrapolation of data from nine different surveys in Asia, Africa and the pacific where a series of MUAC cut-off points have been identified to allow the screening of adults under extreme conditions.
Microbiology
Approximately 3–5 ml of blood was aseptically collected and inoculated in BACTEC Myco/F lytic culture vials for mycobacteria culture within one hour of admission. The cultures were placed in a Bactec FX (BD Diagnostic, Spark MD, USA), an automated machine, and cultured up to six weeks or until positive culture was identified. Confirmatory MPT-64 antigen test was done on positive cultures to differentiate Mycobacterium tuberculosis from non-tuberculous mycobacterium. For pathogens other than tuberculosis 8–10 ml of blood was aseptically inoculated into a Bactec aerobic blood culture bottle and incubated in the Bactec FX.
Data analysis
Data for 201 participants enrolled in the study were transcribed to a Microsoft excel (2010) spread sheet and imported into SPSS version 16.0 for analysis. The multivariate model and multiple imputation were analyzed with Stata version 12.
Continuous variables were summarized as means and standard deviations for normally distributed and medians and interquartile ranges for non-parametric data. Categorical variables were expressed as proportions and summary of odds ratios (OR). The Chi square test was used to examine the association between the independent variables and the dependent variable. The Student t-test was used to examine the association between normally distributed independent variables and the dependent variable, while the Mann-Whitney U test was used for non-parametric data. An association was considered to be significant if the p value was less than 0.05 (one tailed).
Bivariate logistic regression was used to determine factors associated with Mycobacterium tuberculosis bacteraemia using each of the independent variables and Mycobacterium tuberculosis bacteraemia outcome result as the dependent variable. All variables with p value <0.2 were then incorporated into multivariate logistic regression model. Multiple variables were then removed from the model in a step-wise fashion, starting the variable with the highest p value above 0.5. Multiple imputation (m = 5) was used to account for missing lab values in the bivariate model.
Results
Patient enrolment
Three hundred eighteen patients were enrolled in the SSSP and SSSP 2 studies between the period of February 2012 and September 2013. Two patients were enrolled independent of these studies. Out of the 320 participants who were assessed for eligibility in this analysis, 201 met the inclusion criteria and were included in the study. The other patients were excluded because they were HIV-negative. The patient enrolment flow diagram is shown in Figure 1.
Flow chart for the enrolment of study participants. In all, 320 patients were eligible for the study; 119 patients were excluded from the study for the following reason: 42 were HIV-negative or the HIV status was unknown, 15 had no Myco F result, 62 had a diagnosis of TB already and were undergoing treatment.
Demographic and clinical characteristics of the study patients
The mean age of the 201 study participants was 32.3 (SD: 9.5) years and there was an almost equal proportion of male and female participants in the study with 103 (51.2%) being males. Weight loss was the most common symptom 186 (92.5%) of the participants while fever of any duration was present in 150 (74.6%) and cough in 139 (69.2%). Slightly over half, 109 (54.2%), of the study participants were either not on antiretroviral therapy (ART) or the ART history was unknown. For those on ART the median time on ART was 3.5 (0.77–24) months. The mean MUAC for the study participants was 21.0 (SD: 3.4) cm. Sputum was available only in 27 (13.4%) patients and tuberculosis was confirmed microscopically in 11 (5.5%). From the available 105 chest X-rays, 72 (35.8%) participants had chest X-ray findings which were suggestive of tuberculosis.
Demographic and clinical characteristics of the study participants.

Prevalence of mycobacterium tuberculosis bacteraemia and other organisms
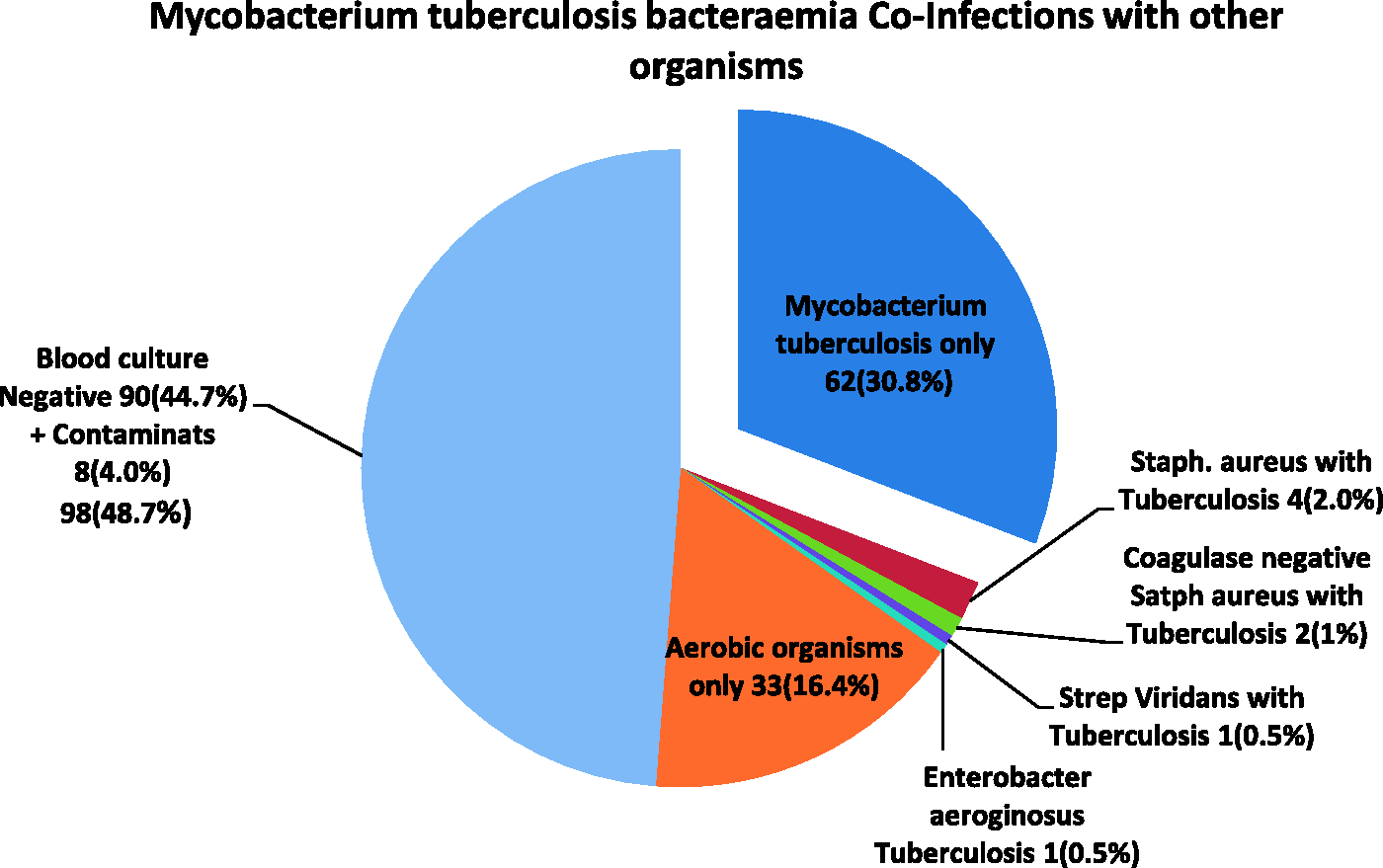
Mycobacterium tuberculosis bacteraemia was detected in 70 (34.8%) of the 201 patients. The prevalence of all other aerobic organisms, excluding those deemed as contaminants, was 33 (16.4%) and the commonly isolated organisms were Staphylococcus aureus 10 (5.0%), Streptococcus five (2.5%), Klebsiella four (2.0%) and E. coli two (1.0%). Other organisms isolated included Salmonella typhi, non-Salmonella typhi, Pseudomonas aeruginosa, Enterobacter and Cryptococcus making up the remainder of the isolates. Coagulase negative Staphylococcus was isolated in five (2.5%). These results are shown in Figure 2. Concomitant Mycobacterium tuberculosis bacteraemia and aerobic bacteraemia were observed in eight (4.0%) of the 201 participants. Of the eight patients with Mycobacterium tuberculosis bacteraemia and bacterial co-infection, Staphylococcus aureus was present in four patients, two had Coagulase negative staphylococcus and Streptococcus viridans while Enterobacteraeruginosus was isolated in the remaining two patients. The Mycobacterium tuberculosis bacteraemia co-infection with other organisms is illustrated in Figure 3. Details of the routine blood culture results are summarized in Table 2.
Pie-chart of organisms isolated from blood culture. Mycobacterium bacteraemia due to tuberculosis was seen in 34.8% patients. Blood cultures were negative in 44.7% patients. Staphylococcus aureus was isolated in 5% while Enterobacterecea were isolated in 4.0% of patients. Pie-chart showing co-infection of Mycobacterium tuberculosis bacteraemia with other organisms. Mycobacterium tuberculosis was the only isolate in 62 (30.8%) participants. Mycobacterium tuberculosis co-infection with other organisms was observed in 8 (4.0%) participants. Routine blood culture findings in 201 HIV-infected patients with severe sepsis.
a
Excludes Myco/F results.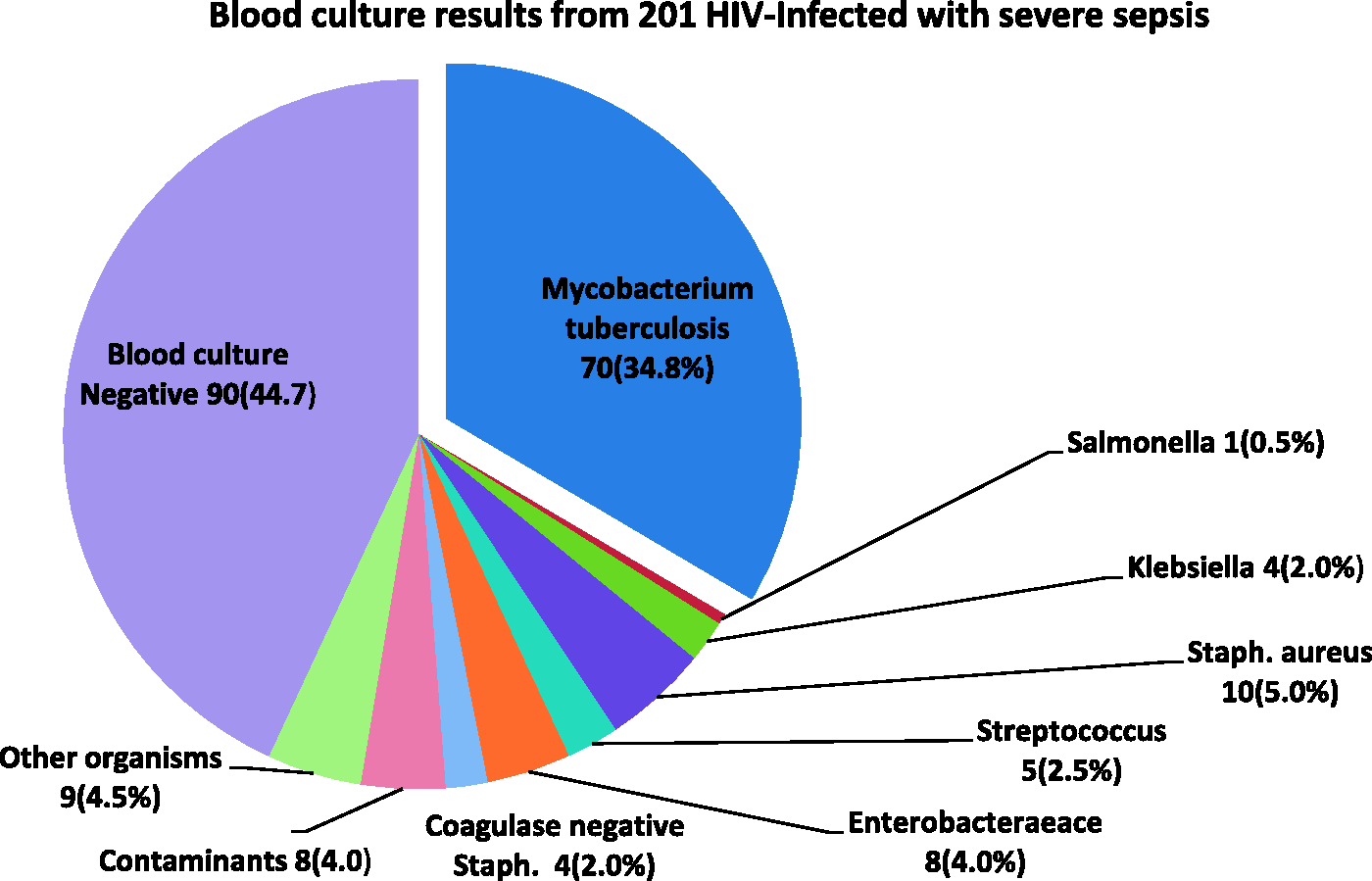
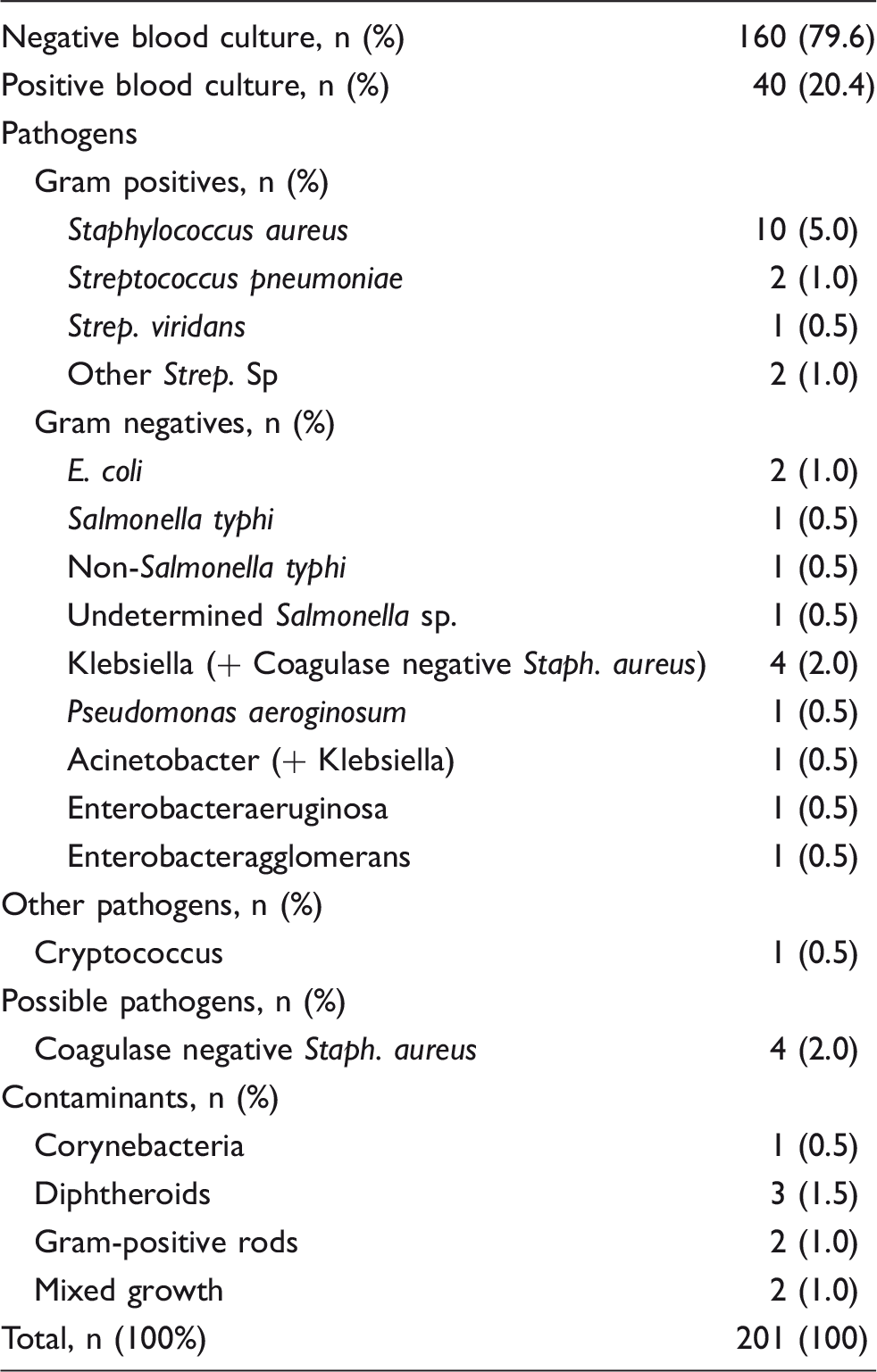
The prevalence of bacterial infections other than Mycobacterium tuberculosis was 41 (20.4%) of the participants.
Aerobic organisms excluding those deemed as contaminants were isolated in 33 (16.4%) of the participants.
Staphylococcus was the commonest Gram-positive organism isolated, 5% (10), followed by Streptococcus pneumonia and Streptococcus viridans at 1% (2) each.
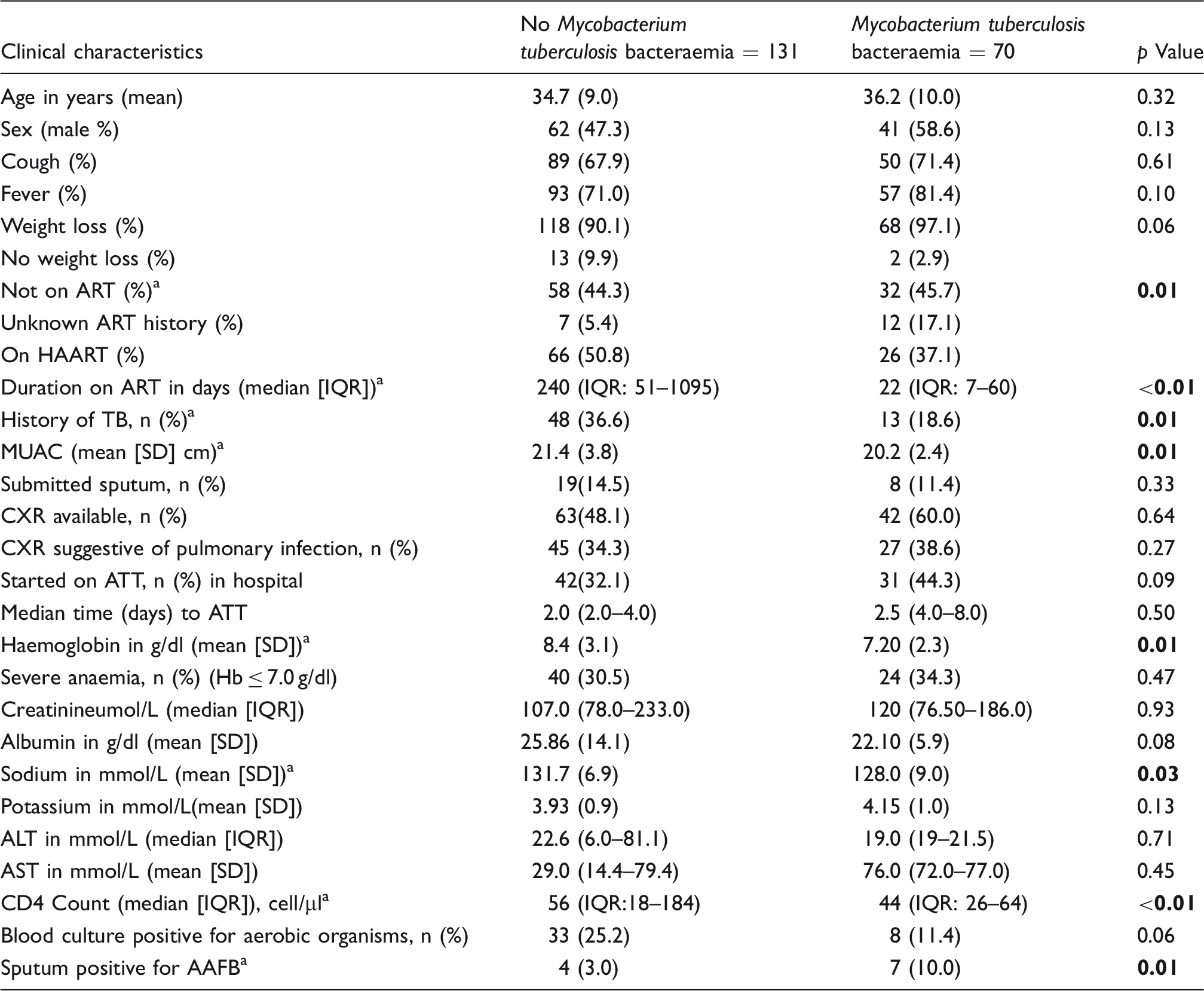
There was no significant difference statistically in the demographic characteristics of the participants with Mycobacterium tuberculosis bacteraemia in comparison to those without. Though not statistically significant, there was a higher proportion of participants who reported weight loss as the main complaint in the Mycobacterium tuberculosis bacteraemia group (68 [97.1%] vs 118 [90.1%], p = 0.06). The proportion of participants with Mycobacterium tuberculosis bacteraemia was significantly higher among patients who were not on ART or unknown ART history. We also observed a significantly higher proportion of participants without Mycobacterium tuberculosis bacteraemia in participants who were treated for tuberculosis in the past compared to those who were not (48 [36.6%] vs 12 [17.1%], p = 0.01). The MUAC was significantly lower in the group with Mycobacterium tuberculosis bactraemia (20.1 [2.4] vs 21.4 [3.4] cm, p = 0.01).
Mycobacterium tuberculosis bactraemia was observed in a significantly higher proportion of participants with confirmed tuberculosis by microscopy. Participants with Mycobacterium tuberculosis bacteraemia had significantly lower CD4 counts (44 [IQR: 26–64] vs 56 [IQR: 18–184], p < 0.01) and albumin levels (22.1 [5.9] vs 25.8 [14.1], p = 0.01) compared to the group without. The study also observed a significantly lower mean haemoglobin (8.4 [3.1] vs 7.2 [2.3] g/dl, p = 0.01) and sodium (137.7 [6.7] vs 128.0 [9.0], p = 0.03) in the participants with Mycobacterium tuberculosis bacteraemia.
Comparison of clinical characteristics between participants with Mycobacterium tuberculosis bacteraemia to those without.
Statistically significant.
Logistic regression analysis
Bivariate and multivariate analysis of factors associated with Mycobacterium tuberculosis bacteraemia in HIV-infected patients with severe sepsis.
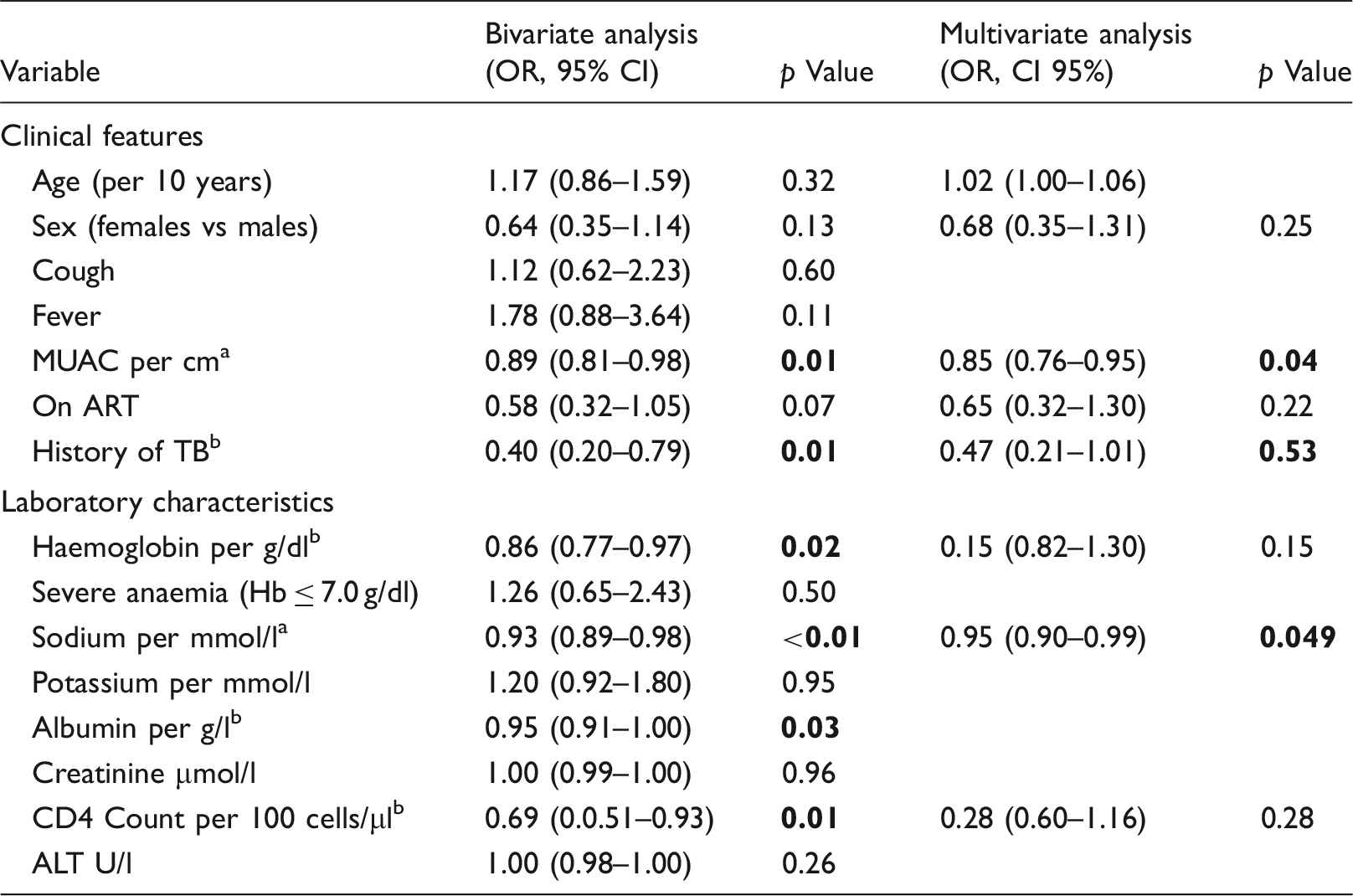
Statistically significant in both the bivariate and multivariate logistic regression analysis.
Statistically significant in the bivariate or multivariate analysis.
Multivariable logistic regression analysis
Seven variables remained in the multivariate logistic regression model after stepwise elimination. Factors that were independently associated with Mycobacterium tuberculosis bacteraemia were MUAC (OR 0.89; CI 95% 0.80–0.99; p ≤ 0.04). These results are shown in Table 4, column 4.
Discussion
The most notable finding of this study was the high prevalence of Mycobacterium tuberculosis bacteraemia of 34.8% in this cohort of HIV-infected patients. This is the highest prevalence of Mycobacterium tuberculosis bacteraemia than what we have seen documented in the region. In our study, severe sepsis due to bacterial infection other than tuberculosis was found in 33 (16.4%) of the study patients and the commonly isolated organism was Staphylococcus aureus followed by enterobactereace and streptococcus species (Streptococcus pneumoniae and Streptococcus viridans). These findings are similar to a study in Lusaka and others in different parts of the world that have evaluated the causes of sepsis among in-patients.15,21,22,24 Concomitant Mycobacterium tuberculosis bacteraemia with bactraemia from other bacterial causes is not unusual. This mixed infection of tuberculosis with other bacterial causes was observed in eight (4%) of the study participants. Clinicians should, therefore, still look out for Mycobacterium tuberculosis bactraemia in HIV-infected patients with severe sepsis who have a positive blood culture for aerobic organisms.
When we compared the participants with Mycobacterium tuberculosis bactraemia to those without, we observed a higher proportion of Mycobacterium bactraemia in the group who were either not on ART or unknown history. This could imply late presentation among our patients who wait until they become very sick before they seek medical services. In case of those who were on ART, the duration of time on treatment was much shorter in the participants with Mycobacterium tuberculosis bactraemia. These, therefore, are patients who were recently started on ART. In these patients, Mycobacterium tuberculosis could have been missed as an opportunistic infection, which eventually lead to disseminated disease and severe sepsis or it could have been part of an immune reconstitution syndrome (IRIS) which presented as Mycobacterium tuberculosis bactraemia. Mycobacterium tuberculosis bacteraemia was less common in participants previously treated for tuberculosis implying that tuberculosis was identified and treated early. This supports the notion that once tuberculosis is diagnosed and treated early, it prevents dissemination of the infection and subsequent development of sepsis.
Although the study participants were generally underweight, the group with Mycobacterium tuberculosis bacteraemia had a significantly lower MUAC. We know that weight loss is a prominent feature of tuberculosis and an indication of active disease. Co-infection of tuberculosis and HIV has synergistic negative effect on weight; this could explain the significantly lower MUAC in the patients with Mycobacterium tuberculosis bacteraemia. The chest X-ray finding in participants with Mycobacterium tuberculosis bacteraemia was not significantly different from the group without. Approximately half of the study participants had a chest X-ray done, for the remainder the clinicians did not request for it or the participants were too ill to be moved.
We observed that participants with Mycobacterium tuberculosis bacteraemia had significantly lower mean haemoglobin compared to the group without. However haemoglobin level was not an independent predictor Mycobacterium tuberculosis bacteraemia in the multivariate logistic regression model. Both Mycobacterium tuberculosis and advanced HIV disease can cause anaemia of chronic inflammation. 16 Study participants with Mycobacterium tuberculosis bacteraemia had a significantly lower mean sodium level. One study in Lusaka, Zambia, observed that 94% of HIV-infected patients presenting with tuberculosis and hypotension had adrenal insufficiency (based on the measurement of serum cortisol levels).25 Some of our study participants probably had adrenal insufficiency which could explain the hyponatraemia we observed. The group with Mycobacterium tuberculosis bacteraemia had a lower albumin, though this was not statistically significant. Albumin is an acute protein that decreases during inflammation. 17 HIV infection and tuberculosis cause chronic inflammation, which synergistically could reduce albumin levels.
We assessed factors that are associated with Mycobacterium tuberculosis bacteraemia using bivariate logistic and multivariate logistic regression. In our study factors that were associated with Mycobacterium tuberculosis bacteraemia in the Bivariate logistic regression were MUAC, a history of being treated for Mycobacterium tuberculosis in the past, haemoglobin, sodium level and CD4 count. After adjusting for other variables factors that were independently associated Mycobacterium tuberculosis bacteraemia were MUAC and sodium level.
Study limitations
The results of this study are limited to HIV infected patients with severe sepsis admitted to hospital in regions where prevalence of tuberculosis is high. Data for haemoglobin were available in 162 patients, 160 patients had CD4 count while 146 had data for albumin available. Only half of the participants were able to do chest X-rays because most of them were too ill to be moved to the radiology department and the portable X-ray machine was not functional in the emergency unit at the time of the study. In some cases the attending physician did not ask for chest X-ray because they did not suspect tuberculosis.
Conclusion
Mycobacterium tuberculosis bacteraemia is very common in patients with advanced HIV disease who present with severe sepsis. In our study factors that were independently associated with Mycobacterium tuberculosis bacteraemia were lower MUAC and lower sodium. In the absence of validated rapid diagnostic tests, clinicians should have a low threshold for suspecting and empirically treating for Mycobacterium tuberculosis bacteraemia in HIV-infected patients with severe sepsis if they have low sodium or low MUAC. Prior history of treatment for Mycobacterium tuberculosis or longer duration of ART might reduce suspicion for Mycobacterium tuberculosis bacteraemia but no clinical factors rule the diagnosis.
Footnotes
Acknowledgements
The authors thank Dr Selestine Nzala, the Assistant Dean (Postgraduate), University of Zambia, School of Medicine for the moral and financial support, the study nurses Emmanuel Chibwe, Joe Musonda, Peter Nyuma, Mary Kaonga and Jibe Milimo, and the patients who accepted to be part of the study.
Declaration of conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received financial support from the John Hopkins AIDS International Training and Research Program through the office of the Assistant Dean (Postgraduate), School of Medicine of the University of Zambia.