
Abstract
Many patients who take antiretroviral drugs also take alternative therapies including dietary supplements. Some drug–supplement combinations may result in clinically meaningful interactions. We aimed to investigate the evidence for dietary supplement interactions with antiretrovirals. A systematic review was conducted using multiple resources including PubMed, Natural Medicine Comprehensive Database, The Review of Natural Products, and Google Scholar. All human studies or case reports evaluating an interaction between a dietary supplement and an antiretroviral were selected for inclusion. Twenty-eight pharmacokinetic studies and case-series/case reports were selected for inclusion. Calcium carbonate, ferrous fumarate, some forms of ginkgo, some forms of garlic, some forms of milk thistle, St. John's wort, vitamin C, zinc sulfate, and multivitamins were all found to significantly decrease the levels of selected antiretrovirals and should be avoided in patients taking these antiretrovirals. Cat's claw and evening primrose oil were found to significantly increase the levels of antiretrovirals and patients should be monitored for adverse effects while taking these dietary supplements with antiretrovirals. This systematic review shows the importance of screening all human immunodeficiency virus patients for dietary supplement use to prevent treatment failure or adverse effects related to an interaction.
Introduction
Human immunodeficiency virus (HIV) infections have continued to be an epidemic in the 21st century. Over 35 million people worldwide are currently living with HIV, including over 1.2 million patients in the US. The Centers for Disease Control and Prevention estimates that approximately 50,000 people are newly infected each year in the US, with the highest incidence occurring in men who have sex with men, blacks/African Americans, and injection drug users. 1
Many HIV patients who are managed on antiretroviral therapy also use complementary or alternative medicine (CAM). 2 CAM includes a variety of different therapeutic modalities including acupuncture, meditation, chiropractic, energy healing, and biological therapies. Biological therapies are among the most commonly used and include vitamins, minerals, herbal products, and other types of dietary supplements. 3 Among HIV patients, dietary supplements are among the most common forms of CAM therapy used.2,4,6
In the US, a dietary supplement is defined by the Dietary Supplement Health and Education Act of 1994 as a product that is intended to supplement a person's diet. Dietary supplements can include ‘vitamins, minerals, herbs or other botanicals, amino acids, a dietary substance for use by man to supplement the diet by increasing the total dietary intake, or a concentrate, metabolite, constituent, extract, or combination of any ingredient previously listed’. 5
A 2008 survey of 128 HIV-positive patients in the US found that 67% took a dietary supplement along with their antiretroviral therapy. 6 The reasons for use included perceived therapeutic benefit, reduction of adverse events associated with antiretrovirals, or increased quality of life. Despite these perceived or potential benefits, there are concerns about dietary supplement interactions with antiretrovirals. A 2002 survey of 118 HIV-positive patients found that 40% reported not disclosing their use of supplements to their prescriber. 7 This lack of awareness is concerning since dietary supplements have the potential to interact with medications.
One of the primary concerns related to interactions with antiretrovirals is that these agents have narrow therapeutic ranges and their efficacy and safety is related to their plasma concentrations.8,9 Subtherapeutic concentrations of these drugs can cause treatment failure and the emergence of viral resistance. Conversely, supratherapeutic concentrations of antiretrovirals can increase the risk of adverse events and potential toxicity.4–9
Among the antiretrovirals, protease inhibitors, non-nucleoside reverse transcriptase inhibitors, and integrase inhibitors have a high risk of potential interactions due to their metabolism by cytochrome P450 (CYP450) isoenzymes and metabolism from other phase II enzymes. Other antiretroviral classes (e.g. nucleoside reverse transcriptase inhibitors or entry inhibitors) are not known to be affected by the CYP450 system or P-glycoprotein (P-gp).4–13
The purpose of this systematic review is to identify and evaluate the documented and clinically meaningful interactions between dietary supplements and antiretrovirals in humans.
Methodology
A systematic review was conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14
A systematic literature search was conducted to identify all relevant literature evaluating interactions between dietary supplements and antiretrovirals utilizing four databases: PubMed, Natural Medicine Comprehensive Database, Review of Natural Products, and Google Scholar. No date restrictions were applied in the resources. The search was conducted between the dates of 23 July and 31 August 2015.
PubMed was searched using the terms ‘Dietary Supplements’ (MeSH) AND ‘Drug Interactions’ (MeSH) OR ‘Herb-Drug Interactions’ (MeSH) AND ‘Anti-Retroviral Agents’ (Pharmacological Action) with the filters of clinical trials conducted in humans and published in ‘English’. A separate search was conducted using the terms ‘Anti-HIV Agents/pharmacokinetics’ (MeSH) AND ‘Area Under Curve’ (MeSH) with the filters of studies conducted in humans and published in ‘English’. Each of the searches was also done with the removal of the limits or filters (i.e. humans and English) to identify articles that may not have been appropriately indexed. These specific search terms and variants of these terms were used as search terms in Google Scholar. In Google Scholar, the results were limited to the first 100 search results to find the most relevant information.
All currently Food and Drug Administration-approved antiretrovirals were evaluated in the Natural Medicines Comprehensive Database using the ‘Natural Product/Drug Interaction Checker’ function. The Review of Natural Products resource was searched to identify references in the ‘Evidence-Based Herb-Drug Interactions’ section.
The reference sections of all literature identified were also hand-searched to identify additional studies.
Article selection
All article types addressing a dietary supplement and antiretroviral interaction in humans were initially screened and considered for inclusion. Articles were selected for full review and inclusion in this systematic review if they evaluated the interaction between a dietary supplement and antiretroviral in humans. In vitro or animal studies were excluded.
An initial screening of article titles or abstracts was conducted by one author (MJ). Irrelevant search results were excluded. Articles that were not initially excluded were then independently screened and evaluated for inclusion by two authors (PJG, DH). Discrepancies were resolved via discussion among authors (MJ, PJG, DH).
Data extraction
Articles selected to be included had the following information extracted: Author name, year of publication, study type or design, number of patients, HIV status of patients, dietary supplement (proprietary name, manufacturer information), dietary supplement dosing information, antiretroviral medication (proprietary name, manufacturer information), antiretroviral dosing information, approximate days of dietary supplement and antiretroviral coadministration, and pharmacokinetic outcomes, if applicable.4–13,15 Two (PJG, DH) authors independently reviewed the included studies. Discrepancies were resolved via discussion among authors (MJ, PJG, DH).
Results
The systematic search identified 533 articles that were screened for potential inclusion. Of these, 28 were selected for inclusion (Figure 1). Five-hundred and five articles were excluded because they were in vitro or animal studies, review articles, or studies not utilizing a dietary supplement preparation.
PRISMA diagram for included studies.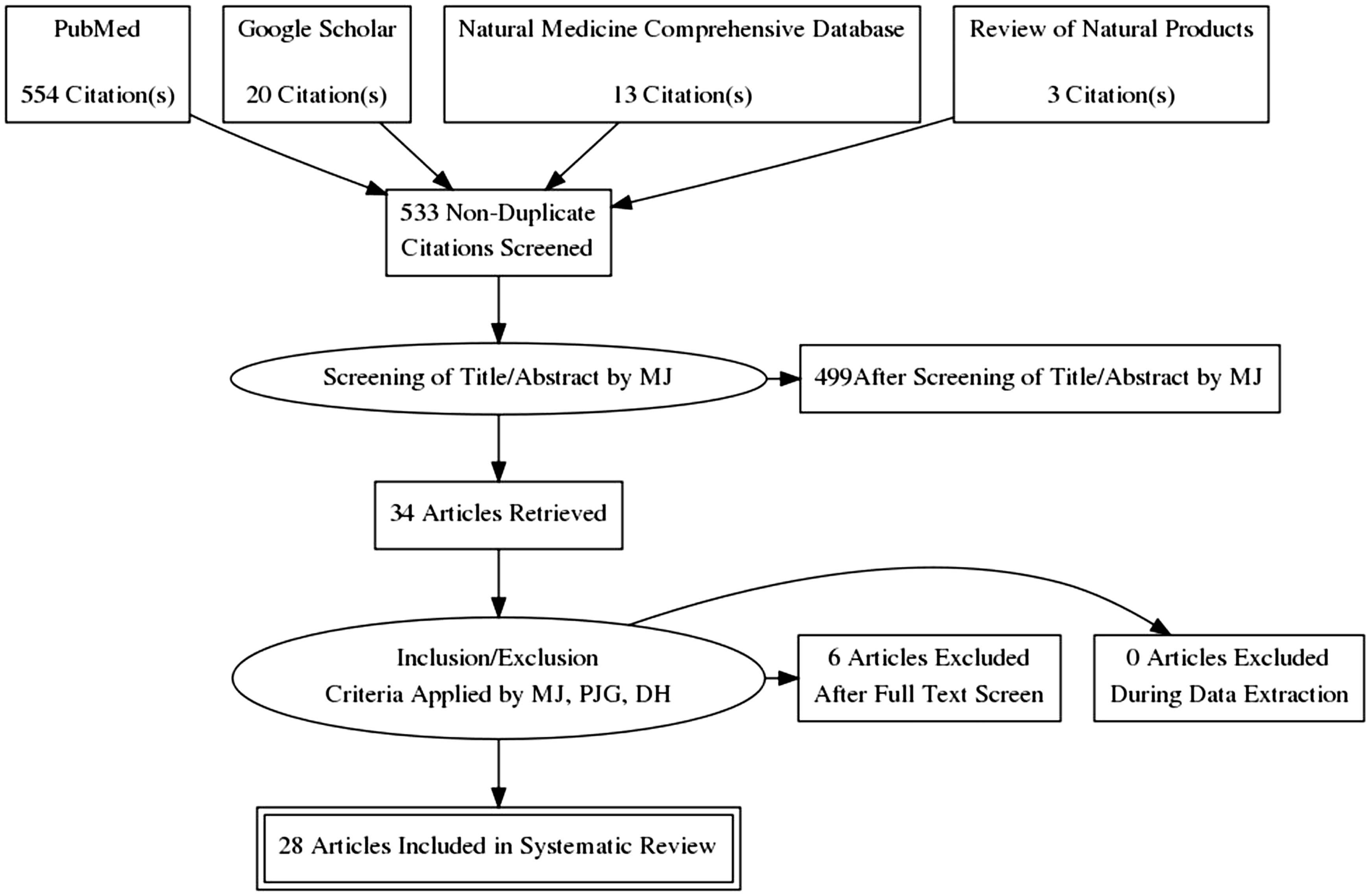

Another pharmacokinetic study found that milk thistle decreased Cmin of indinavir by 25% but did not affect indinavir’s AUC or other pharmacokinetic parameters. 34
The other 17 pharmacokinetic studies found no significant effect of the dietary supplement on antiretrovirals levels. The supplements evaluated in these studies included African potato (Hypoxis hemerocallidea or H. obtusa), beta-carotene, Echinacea, fish oil, ginseng, goldenseal root, and Panax ginseng.16–18, 21–23,25,26,28,29,30,32,33,35–38
In two case reports, dietary supplement use was associated with increased levels of selected antiretrovirals. Evening primrose oil appeared to increased lopinavir levels in one case report. 24 In another single case report, cat’s claw was suspected to have increased atazanavir, saquinavir, and ritonavir levels. 20
In one case report, ginkgo use was associated with treatment failure in a patient taking efavirenz. 31 A case series also found that St. John’s wort was associated with decreased the nevirapine levels. 40
Synthesis of these data shows that some of the findings are contradictory for certain dietary supplement ingredients, including garlic, ginkgo and milk thistle. In two pharmacokinetic studies, daily use of garlic extract 20 to 1200 mg (Natural Source Odourless Garlic from Life Brand, Canada; Garilpure from Natrol Inc., USA) did not significantly change the pharmacokinetics of a single dose of ritonavir 400 mg or saquinavir 1200 mg.26,28
However, in another pharmacokinetic study, using a different garlic product (GarliPure, Natrol Inc., USA) 4.64 mg twice daily, saquinavir levels were reduced by over 50% after approximately two days of coadministration. 27 However, these findings may be unreliable due to the methodological concerns of this pharmacokinetic study (e.g. use of fixed-sequence versus cross-over study design). This study did not account for the ability of saquinavir to alter its own metabolism, therefore increasing the risk of bias within the study.10,46
This phenomenon was comparable to ginkgo, where two pharmacokinetic studies with specific formulations of ginkgo (Tavonin from Willmar Schwabe GmbH, Germany and Ginkgo from Nature’s Way, Inc., USA) did not a change the pharmacokinetics of either raltegravir, lopinavir, or ritonavir after 1 to 14 days of coadministration.29,30 However, a case report suggested that ginkgo (unknown manufacturer) significantly reduced the levels of efavirenz, resulting in treatment failure. 31 The reasons for these differences in findings are not clear.
Similar to garlic and ginkgo, some milk thistle preparations (e.g. Standardized Milk Thistle, Legalon) doses ranging from 450 mg to 1368 mg per day did not significantly change the pharmacokinetic parameters of indinavir, darunavir, or ritonavir after 1 to 14 days of coadministration.33,35,36 However, the daily coadministration of a different preparation of milk thistle (Thisilyn, Nature’s Way, USA) significantly reduced the Cmin of indinavir after three days of coadministration. 34 Differences in product formulation or concentration of active constituents may explain these different findings.
Discussion
This systematic review identified 28 articles addressing dietary supplement interactions with antiretrovirals. Most of these were pharmacokinetic studies; however, fewer than half of these detected a clinically meaningful interaction. Eleven dietary supplements were identified that may result in a clinically significant interaction when used in combination with selected antiretrovirals. Although most studies evaluated only one combination of dietary supplement and antiretroviral, these findings have implications for interactions with other antiretrovirals. For example, some supplements may impact antiretrovirals via inhibition or induction of isoenzymes of CYP450. In these instances, it is plausible that these supplements have the potential to interact with many other antiretrovirals that are metabolized through these pathways.

NNRTI: non-nucleoside reverse transcriptase inhibitor; INSTI: integrase inhibitor; NRTI: nucleoside reverse transcriptase inhibitor; PI: protease inhibitor.
While this systematic review was comprehensive in the search and evaluation of human studies or case reports, there are many limitations to the drug–supplement interaction data related to antiretrovirals.
A primary limitation of the drug–supplement interaction data is simply the lack of comprehensive data in this subject area. The top ten most commonly used dietary supplements in the US are co-enzyme Q10, cranberry extract, Echinacea purpurea, fish oil/omega-3 fatty acids, garlic extract, ginkgo, ginseng, glucosamine/chondroitin, melatonin, and prebiotics/probiotics products. 41 Of these common dietary supplements, only four dietary supplements (E. purpurea, fish oil/omega-3 fatty acids, garlic extract, and ginkgo) have been evaluated in combination with antiretrovirals.21–23,25,26–31 The potential for antiretroviral interactions with the remaining dietary supplements has not been evaluated. There are various in vitro data suggesting many dietary supplements can impact with CYP450 and therefore potentially interact with many more antiretroviral drugs, but these interactions remain to be studied in humans.4–13
All of the studies evaluated used only one specific dietary supplement preparation. The formulation studied may not have the same effects as another preparation due to the differences in extraction methods, active constituents, or concentrations of the active constituents in the dietary supplement formulation. Also, the pharmacokinetic studies may have used different study protocols (e.g. use of fixed-sequence versus cross-over study design). Therefore, some forms of the dietary supplement may interact while others may not. This phenomenon was most interestingly noted for garlic. While one pharmacokinetic study suggested a significant interaction with garlic and saquinavir, presumably through induction of CYP3A4, the majority of the in vivo evidence suggests that various preparations do not have any clinically significant effect on various CYP isoenzymes.45,46 This phenomenon was also observed with ginkgo and milk thistle.45,46
Also, some of the pharmacokinetic studies used only a single dose of the antiretroviral to evaluate the interaction, while other studies allowed for patients to reach steady-state. In the pharmacokinetic study by Gallicano et al., 26 patients were only given a single dose of a ritonavir to evaluate its interaction with a garlic supplement, and no significant interaction was observed. However, Piscitelli et al., 27 observed a significant reduction in saquinavir levels after patients were given two days of coadministration with its garlic preparation. 27 Therefore, while some studies may not have found a significant change in the pharmacokinetics of the antiretroviral, this may be due to not reaching steady-state, which would more closely emulate clinical practice. Unfortunately, no validated quality standards or scales are available to consistently appraise the quality or risk of bias of such pharmacokinetic studies. This limitation was also noted by researchers who conducted a previous systematic review in 2005. 12
Overall, due to the high prevalence of dietary supplement use in HIV patients, healthcare providers need to screen all HIV patients for dietary supplement use to avoid potentially harmful drug-supplement interactions. If a clinician identifies a dietary supplement that has documented evidence suggesting a potential interaction, he or she should consider stopping the dietary supplement to prevent treatment failure or potential adverse outcomes. Additionally, clinicians should be vigilant to monitor HIV patients who may be taking dietary supplements with unknown interaction potential to ensure that antiretroviral treatment effectiveness is not compromised.
Conclusion
Clinical evidence suggests that coadministration of specific formulations of some dietary supplements with antiretrovirals causes significant interactions. Only a small number of drug–supplement combinations have been studied to identify potential interactions. Therefore, it is important recognize that many potential interactions may not have been identified at this time. Healthcare providers should investigate the use of dietary supplements in all HIV patients to successfully intervene and discuss the risk of treatment failure or adverse events while using any of these interacting dietary supplements. Patients should be advised to avoid dietary supplements known or suspected to cause clinically meaningful interactions especially if any potential benefit of the dietary supplements is unproven or unclear in the HIV population.
Footnotes
Acknowledgements
This research was conducted during the completion of the clinical and translational sciences graduate certificate program at the Creighton University Department of Clinical and Translational Science. This research was conducted during the drug information and evidence based practice post-doctoral research fellowship at Creighton University under the excellent mentorship of Philip J Gregory, Darren Hein, Zara Risoldi Cochrane, and Aleah Rodriguez.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.