
Abstract
Chronic conditions have largely replaced opportunistic infections as the leading causes of mortality in human immunodeficiency virus (HIV) infection. Pancreas transplantation alone can be performed for people with difficult to manage diabetes associated with severe hypoglycaemic unawareness. For carefully selected patients, pancreas transplantation alone has the potential to dramatically improve quality and quantity of life. Historically, HIV was considered a contraindication to transplantation; however, today renal transplantation for people with end-stage kidney disease and HIV infection is increasingly common. We describe the use of a standard immunosuppression regimen in combination with effective antiretroviral control using a stable highly active antiretroviral therapy regimen with minimal interaction with immunosuppressants. We describe what is, to our knowledge, the first case of pancreas transplantation alone performed for this particularly challenging group, resulting in complete resolution of hypoglycaemic symptoms. We suggest that this group of patients should receive optimal diabetes management, including access to transplantation where appropriate, and demonstrate that pancreas transplantation alone is feasible for people with HIV infection.
Introduction
Human immunodeficiency virus (HIV) infection affects 39.5 million people worldwide and over 100,000 in the UK. 1 The availability of highly active antiretroviral therapy (HAART) has resulted in dramatic improvements in survival and disease, with chronic conditions largely replacing opportunistic infections as the leading causes of mortality. 2 The effects of HIV infection and HAART on metabolic regulation have resulted in an increased prevalence of dyslipidaemia, diabetes mellitus and insulin resistance in HIV-infected patients. 3 Pancreas transplantation alone (PTA) can be performed for people with difficult-to-manage diabetes associated with severe hypoglycaemic unawareness. For carefully selected patients, PTA has the potential to dramatically improve quality and quantity of life. 4 We describe the first reported case of successful pancreas transplant alone in a patient with HIV infection and difficult-to-manage diabetes.
Case
A 42-year-old man with type 1 diabetes (T1DM) and HIV infection was referred to our centre for assessment for PTA. He had a BMI of 25 kg/m2 and was affected by frequent episodes of hypoglycaemic unawareness, many of which required bystander intervention. His diabetes was associated with severe autonomic neuropathy with gastroparesis and postural hypotension, peripheral neuropathy and pancreas exocrine failure. He was managed on multiple daily injections, with a pre-operative glycosylated haemoglobin (HbA1c) of 8.5% and eGFR of 80 mL/min/1.73 m2. HIV infection was diagnosed in 2006 and managed with a stable regimen of nevirapine, abacavir and lamivudine. His CD4 cell count had remained above 250 cells/mm3. At listing, his CD4 cell count was 400 cells/mm3 and viral load undetectable, and he was monitored on a four-monthly basis on the waiting list.
Post-operative drug regimen.
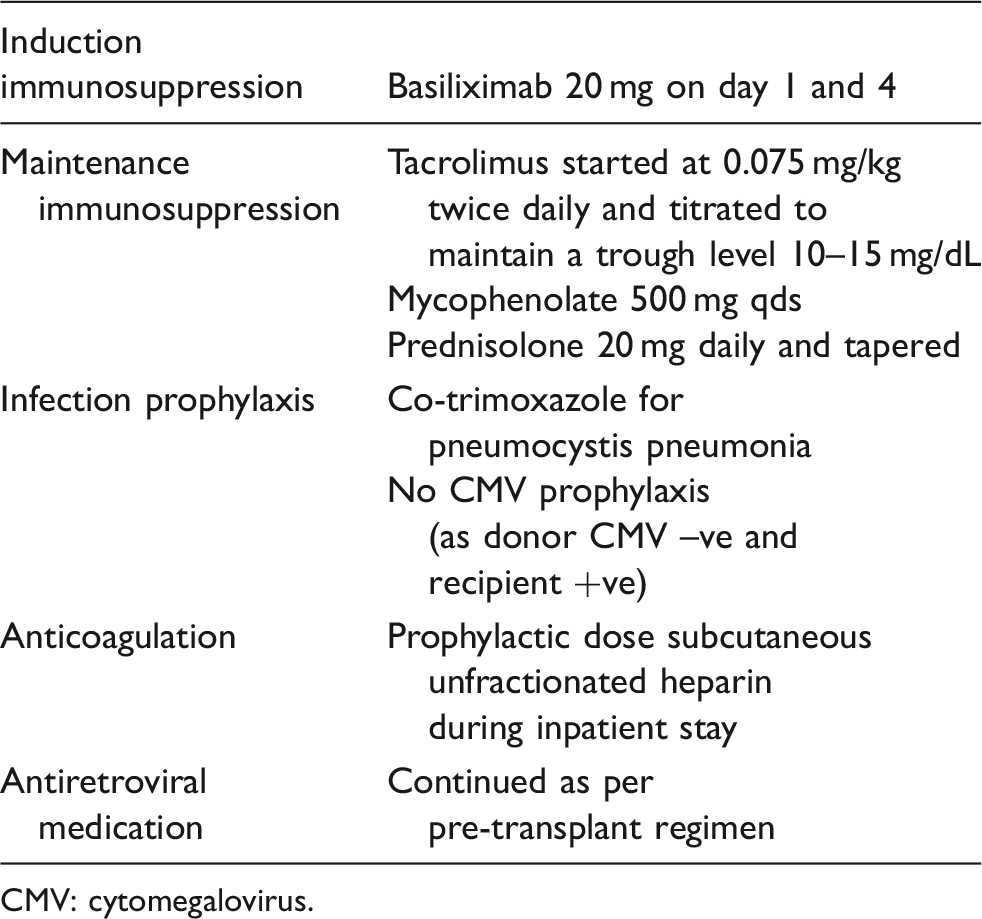
CMV: cytomegalovirus.
Euglycaemia and insulin-independence were achieved intraoperatively and maintained following discharge. The patient did not experience any episodes of hyperglycaemia or hypoglycaemia. HbA1c at three months post-transplant was 4.8%. At one month post-transplant, the patient was found to have asymptomatic cytomegalovirus (CMV) viraemia and was treated with a course of valganciclovir. At four months post-transplant, neutropenia was noted and managed with cessation of mycophenolate and co-trimoxazole. HAART was continued in accordance with his pre-operative regimen; CD4 cell counts were maintained above 250 cells/mm3, and HIV viral load remained undetectable. The patient remained systemically well, apart from nausea secondary to gastroparesis. His serum creatinine varied with fluid status between 108 and 164 µmol/L. He remains well with good control of blood glucose and HIV infection at 12 months post-transplant (Figure 1).
Graph of random serum glucose levels (mmol/L) achieved post-transplant.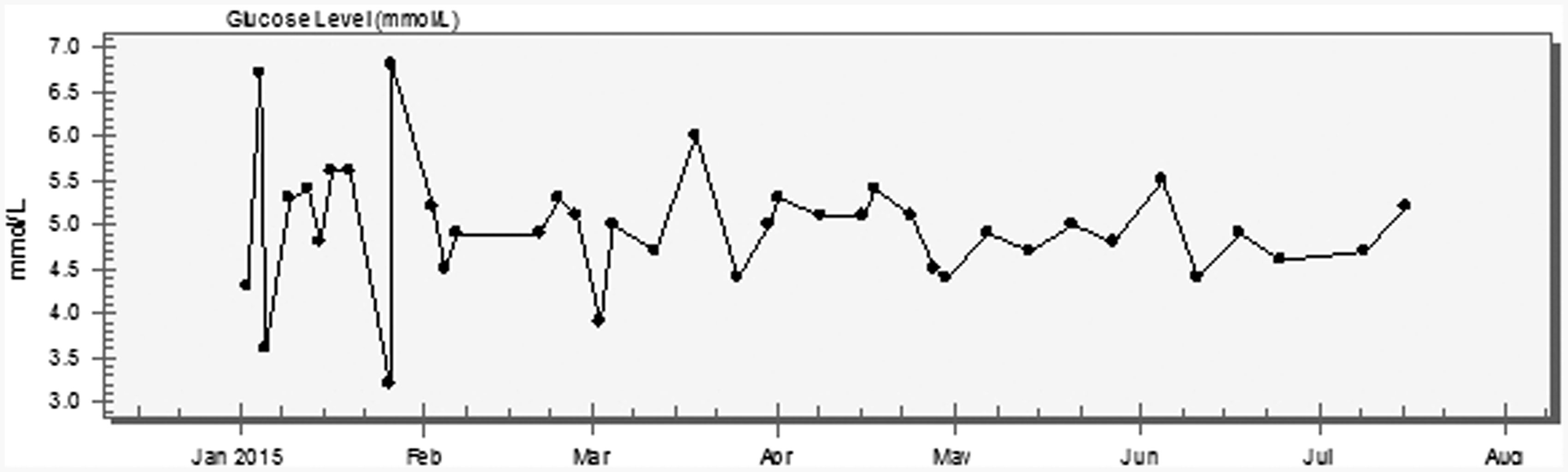
Discussion
Historically, HIV was considered a contraindication to transplantation. 5 However, today renal transplantation for people with end-stage kidney disease and HIV infection is increasingly common 6 and, although associated with higher rates of allograft rejection, patient and graft survival rates are similar to those of the non-HIV population.7,8 The published rate of HIV-associated chronic kidney disease varies widely between populations and has been reported as affecting 6.0%–48.5% of HIV-infected individuals in Africa and 3.5%–4.7% of HIV-infected individuals in Europe. Causes of renal failure also vary between populations, with HIV-associated nephropathy now less common in those with access to HAART and accounting for approximately 25%–30% of cases, the majority of remainder attributable to other glomerular and tubular diseases including diabetic nephropathy. 9
Five percent of people with type 1 diabetes have recurrent severe hypoglycaemia, which can be life-threatening. For people deemed to be suitable to undergo the operation, pancreas transplantation can offer substantial benefits to quality and quantity of life. 4 Graft outcomes after PTA have improved significantly over time, with current one-year graft survival greater than 80%. 10 A small number of cases of simultaneous pancreas–kidney transplantation (SPK) have been reported for diabetic patients with HIV infection with variable results.11–13 Nevertheless, for diabetic patients with HIV and preserved kidney function, transplant options have been limited.
Although incident diabetes has not been shown to be related to duration of HIV infection or to CD4 cell count, 14 there is some evidence that HIV replication in human T cells may affect lipid metabolism, 15 and autoimmune diabetes has been seen to develop de novo following immune restoration, particularly in those who are genetically susceptible.16,17 Furthermore, it has been noted that protease inhibitors are associated with a higher rate of diabetes in comparison with HIV-infected patients who are therapy naïve,18,19 and long exposure to antiretrovirals increases insulin resistance and impairs insulin secretion. 20 Lipodystrophy appears to accelerate failure of insulin secretion, 14 and dyslipidaemia also confers additional diabetes risk, or may induce diabetes in susceptible individuals. 20 Together, these features make management of diabetes in people with HIV complex.
We describe the use of a standard immunosuppression regimen in combination with effective antiretroviral control using a stable HAART regimen with minimal interaction with immunosuppressants. It is known that steroids increase insulin resistance and tacrolimus also has diabetogenic effects, although the mechanism is unknown. Nevertheless, these immunosuppressants remain standard in the post-operative regimen of both pancreas and kidney transplant recipients. As in PTA recipients without HIV, it is possible that renal function may deteriorate secondary to calcineurin inhibitor (CNI) toxicity and must be monitored closely, and careful balance must be achieved between avoiding the risk of rejection and avoiding CNI over-exposure. Although there is insufficient evidence to recommend a higher eGFR threshold for SPK transplantation in patients with diabetes and HIV, each case warrants careful consideration with appeal to the Pancreas Advisory Group, through established protocols, where renal function has been deteriorating or is borderline.
We describe what is to our knowledge the first case of PTA performed for this particularly challenging group, resulting in complete resolution of hypoglycaemic symptoms. We suggest that this group of patients should receive optimal diabetes management, including access to transplantation where appropriate, and demonstrate that PTA is feasible for people with HIV infection.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of the medical, nursing and laboratory teams involved in the clinical care provided in the Renal Transplantation Department, Guy’s Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.