
Abstract
We report the use of crushed dolutegravir (DTG) and tenofovir alafenamide (TAF) tablets in a 27-year-old man with progressive dysphagia due to eosinophilic esophagitis, which severely limited compliance, leading to viral resistance. Based on his drug resistance history, allergies, and inability to swallow tablets intact, he was transitioned to DTG 50 mg (crushed), TAF 25 mg (crushed), liquid abacavir (20 mg/ml) 30 ml, and liquid emtricitabine (10 mg/ml) 24 ml orally daily. After receiving this regimen for five months, the patient’s HIV viral load decreased from 9910 to 59 copies/ml and after ten total months became suppressed at <20 copies/ml. Our case report suggests administration of crushed DTG and TAF tablets may be a viable option for patients with dysphagia and limited treatment options.
Introduction
There are significant difficulties associated with administering antiretrovirals in patients with dysphagia and limited data on the effects of crushing these medications. Turley and Fulco 1 reported successful virological suppression despite decreased dolutegravir (DTG) levels in a patient receiving twice-daily dosing of DTG via an orogastric tube. Similarly, Brooks et al. 2 observed lower levels of DTG when administered once-daily via jejunostomy tube. Altered bioavailability with administration of crushed combination tablets containing either DTG or tenofovir alafenamide (TAF) has also been reported. Roskam-Kwint et al. 3 found increased DTG exposure in healthy volunteers receiving crushed DTG/abacavir (ABC)/lamivudine tablets, and Chrdle et al. 4 observed adequate concentrations and clinical efficacy in an HIV patient receiving the same therapy via a nasogastric tube. Brown et al. 5 observed decreases in Cmax and AUC for the TAF component of darunavir/cobicistat/emtricitabine (FTC)/TAF in healthy volunteers. Additionally, viral suppression with crushed tenofovir disoproxil fumarate (TDF)/FTC and once-daily DTG has been observed. 6
To our knowledge, this is the first case report describing the efficacy of crushed TAF and DTG once-daily for oral administration in person living with HIV.
Case report
Our patient had received several antiretroviral regimens prior to being trialed on the regimen described in the abstract. He was diagnosed with HIV in 2010, but did not seek treatment until 2014 (HIV RNA 37,300 copies/ml; CD4 154 cells/mm3). He was started on elvitegravir/cobicistat/FTC/TDF 150/150/200/300 mg po daily, but stopped two months later due to trouble swallowing the single-tablet regimen (Table 1). His regimen was changed to rilpivirine (RPV) 25 mg, ABC (20 mg/ml) 30 ml, and 3TC (10 mg/ml) 24 ml po daily due to RPV’s small tablet size and availability of liquid formulations for the other agents. However, the patient complained of nausea and poor palatability leading to nonadherence and virologic failure. He was found to have the following genotypic mutations: K101E, M184V, M230L, A98G, L10I, E35D, and M36I and was switched to a regimen of DTG 50 mg po BID, zidovudine/lamivudine 300/150 mg po BID, and TDF 300 mg po daily. The patient continued to have progressive dysphagia resulting in an inability to swallow any pills and inadequate dietary intake. He was referred to a gastroenterologist, diagnosed with eosinophilic esophagitis (EoE) on biopsy (Figure 1) and started on omeprazole 40 mg po daily. Further evaluation by an allergist revealed the patient’s dietary triggers included fish, eggs, milk, nuts, and mint/peppermint. His HIV medications were stopped to avoid the development of further drug resistance during initial management of his EoE with a 37-day prednisolone taper. The patient noted lessened dysphagia with glucocorticoid treatment and repeat endoscopy showed significant improvement. He was then started on DTG 50 mg po daily (crushed), TDF (40 mg/g) 7.5 scoops with soft food, ABC (20 mg/ml) 30 ml po daily, and FTC (10mg/ml) 24 ml po daily. However, the patient complained of poor palatability of the TDF powder formulation, which was replaced with TAF 25 mg po daily (crushed). After receipt of this regimen for five months, the patient’s HIV viral load (VL) decreased to 59 copies/ml and his CD4 cell count increased to 182 (11%). His VL became suppressed at <20 copies/ml after an additional five months.
Patient’s antiretroviral regimen and HIV viral load.

ABC: abacavir; ART: antiretroviral therapy; COBI: cobicistat; DTG: dolutegravir (once daily); EVG: elvitegravir; FTC: emtricitabine; liq: liquid; pow: powder; RPV: rilpivirine; TAF: tenofovir alafenamide; TDF: tenofovir disoproxil fumarate; 3TC: lamivudine; ZDV: zidovudine.
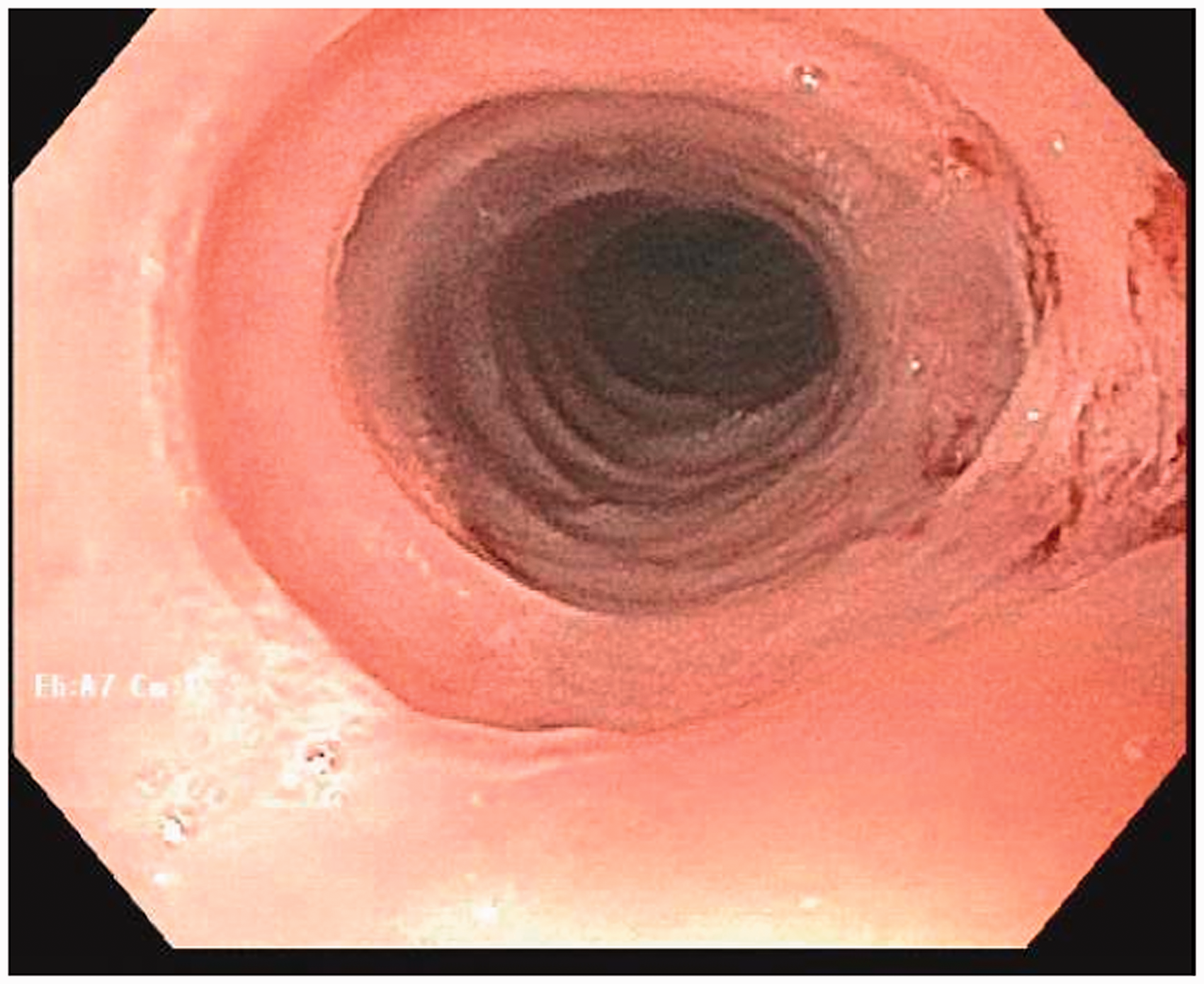
Upper gastrointestinal endoscopy with eosinophilic esophagitis of the upper third of the esophagus.
Discussion
EoE treatment includes proton pump inhibitors, glucocorticoids, and esophageal dilation. 7 EoE is exacerbated by dietary triggers; thus, diet therapy is a cornerstone of EoE management. 7 Our patient’s allergies included peppermint. Liquid ritonavir is flavored with peppermint, which precluded the use of a protease-inhibitor regimen due to EoE exacerbation risk.8,9
In this patient, effective management of EoE was essential to promoting HIV therapy adherence. In addition to treatment by a gastroenterologist, this patient was seen in our HIV clinic by a care team including a nurse practitioner, pharmacist, and social worker on a monthly basis for the first four months he received the described regimen and then every three months thereafter to support medication adherence, monitor clinical response, and ensure access to medications.
The patient was intolerant of crushed TDF and TDF powder due to taste and nausea. Based on the patient’s viral resistance patterns, allergies, and medication intolerance, the decision was made to start crushed TAF. TAF is a biopharmaceutical class (BCS) III agent, as it dissolves quickly in solvent, but is not readily absorbed within the gastrointestinal tract. 10 The FDA-approved labeling does not provide guidance on crushing TAF. 11 Per the manufacturer, the medication is soluble in water but has a bitter/burnt aromatic flavor. 12
DTG is a BCS Class II agent and would be expected to have limited solubility, but high permeability. 13 Its absorption is increased by administration with high-fat food. 14 Throughout therapy, our patient reported intermittent difficulty with oral intake due to dysphagia and nausea. However, per the package insert DTG may be taken without regard to food and as the patient responded clinically, it appears DTG absorption was adequate. 15
Therapeutic drug monitoring (TDM) may have been useful to confirm target concentrations of DTG in our patient, but this is not typically done for nucleoside reverse transcriptase inhibitors as plasma concentrations do not reflect intracellular concentrations.16,17 Given the anticipated time delay in receiving results and the fact that this patient’s clinical response was followed closely, we opted against utilizing TDM at the time.
Though concerns for adequate absorption of both crushed DTG and TAF were reasonable upon initiation of the regimen, the patient’s sustained virologic suppression demonstrated efficacy. Our case report suggests that crushing TAF and DTG in conjunction with other antiretroviral therapy may be a viable option for patients with dysphagia. Additional studies and data are needed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.