
Abstract

Dear Editor,
Anal cancer used to be a rare cancer prior to the HIV epidemic in the 1980s. 1 Since then, the number of anal cancer cases have risen sharply and continuing to rise despite effective HIV treatment. Studies have shown rates to be as high as 137 in 100,000 individuals.2,3 Anal cancer has now become one of the most common non-AIDS-defining cancers amongst HIV-positive individuals. 4
HIV-positive men who have sex with men (MSM) are particularly affected, with a mean age of presentation in their fourth decade of life. 5 Prognosis is directly correlated with tumour size at diagnosis. Data from US National Cancer Institute have shown that tumours less than 2 cm had an 80% five-year survival compared with a prognosis as low as 45% when the tumour was more than 2 cm and 20% in metastatic tumours. 6 Currently, most tumours are detected with a mean size of 3–4 cm. 7
There is uncertainty in UK guidelines regarding the most effective method of screening HIV-positive MSM for anal cancer,8,9 with one guideline implying that patients self-examine and report any lumps noticed in the anal canal. 8 The European AIDS Clinical Society Guidelines recommend that HIV-positive MSM should have ‘a digital rectal exam +/− a Papanicolau test’ every one to three years. 10 However, evidence to support this is currently only based on expert opinion with a lack of evidence from randomised controlled trials. Paucity of evidence in this area contributes to physician ambivalence in offering regular digital ano-rectal examination (DARE). 11
Before anal cancer screening can be implemented into routine HIV care of MSM, it is important to assess its acceptability to patients. Two Australian studies have shown that DARE is acceptable.12,13 Patients were more willing to have DARE in sexual health clinics than in other settings (General Practice or Infectious Diseases clinics). 13 No such study has been done in the UK, and the benefit of such a strategy in a sexual health managed HIV cohort is still unknown.
A departmental policy was introduced in 2015 to offer annual DARE to HIV-positive MSM following two mortalities due to delayed diagnosis of anal cancer. We carried out a questionnaire survey of a consecutive sample of HIV-positive MSM to investigate the acceptability of having DARE as screening for anal cancer. Secondary outcomes were to assess the patient experience and clinical outcomes of DARE. Ethical approval for this service evaluation was granted by the Trust Research and Clinical Audit department.
From pre-published clinic lists covering the eight-week recruitment period, patients fitting the inclusion criteria (HIV-positive MSM aged ≥ 35 years) were invited to participate in the service evaluation when they attended clinic for their routine HIV appointments. Patients were asked to complete a questionnaire and invited to have DARE as part of their consultation. We adapted a validated questionnaire used in the Australian study 12 after obtaining consent from the lead author.
Attitudes towards anal cancer screening and DARE were assessed through a two-part acceptability questionnaire using a Likert scale. The first part of the questionnaire aimed to assess patient attitudes towards DARE as an anal cancer screening tool and their perceived risk of developing anal cancer. This was completed prior to their consultation in the waiting room. For those who consented for DARE, it was performed as part of the consultation. If a patient had consented for the study but opted out of having DARE, the information they provided on the initial part of the questionnaire was used for analysis. Following DARE, patients were asked to complete the second part of the questionnaire when they returned to the waiting room. This assessed their experience of having DARE. Clinicians recorded DARE findings on a separate record which were matched to questionnaires by the researcher using the study number.
Of the 44 patients invited, 30 (68%; 95% CI 54–82) agreed to participate; 29 (97%) of the 30 patients proceeded to have DARE. The one patient who completed the first part of the questionnaire but did not proceed to DARE gave no reason for opting out of DARE.
Fourteen patients (32%; 95% CI 21–43) declined to take part. Principal reasons for decline were ‘lack of time’ (n = 7; 50%; 95% CI 24–76) and ‘not feeling clean’ (n = 3; 21%; 95% CI 0–42). Other reasons for patient refusal included men now identifying themselves as heterosexual (n = 1; 7%), men currently not sexually active (n = 1; 7%) and men perceiving a low risk for anal cancer because they are non-receptive for anal sex (n = 2; 14%).
The mean age of men recruited was 50 years (range 35–67 years). All patients were on antiretroviral therapy. Mean CD4 cell count was 693 cells/µL (range 200–1650 cells/µL). Only three patients (10%) had a detectable viral load of over 40 copies/mL (‘blip’ in two patients as they subsequently re-suppressed, one was a recent treatment starter).
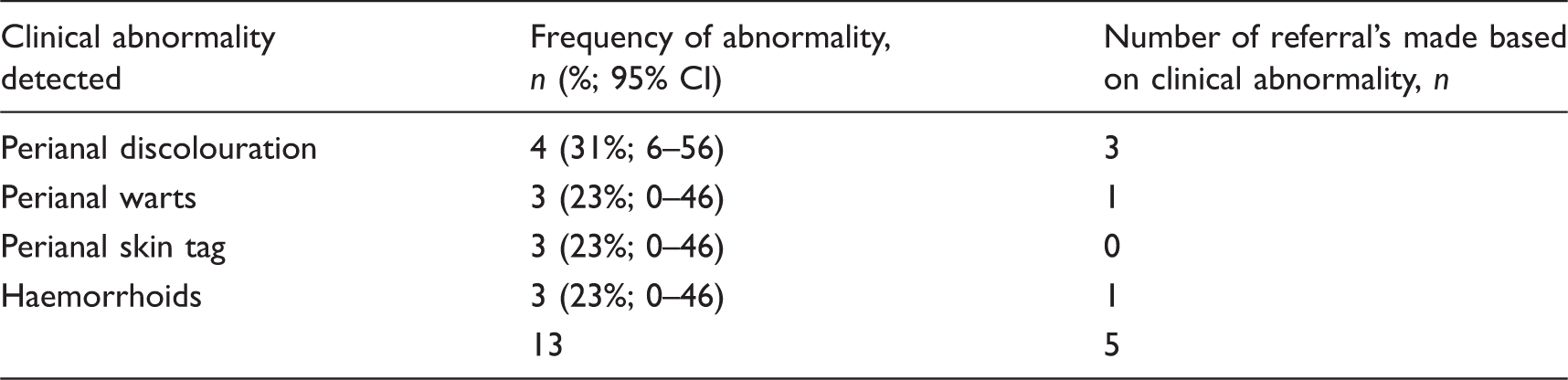
Description of the clinical abnormalities found during DARE.
Clinician’s description of DARE findings that required a colorectal referral and outcomes.
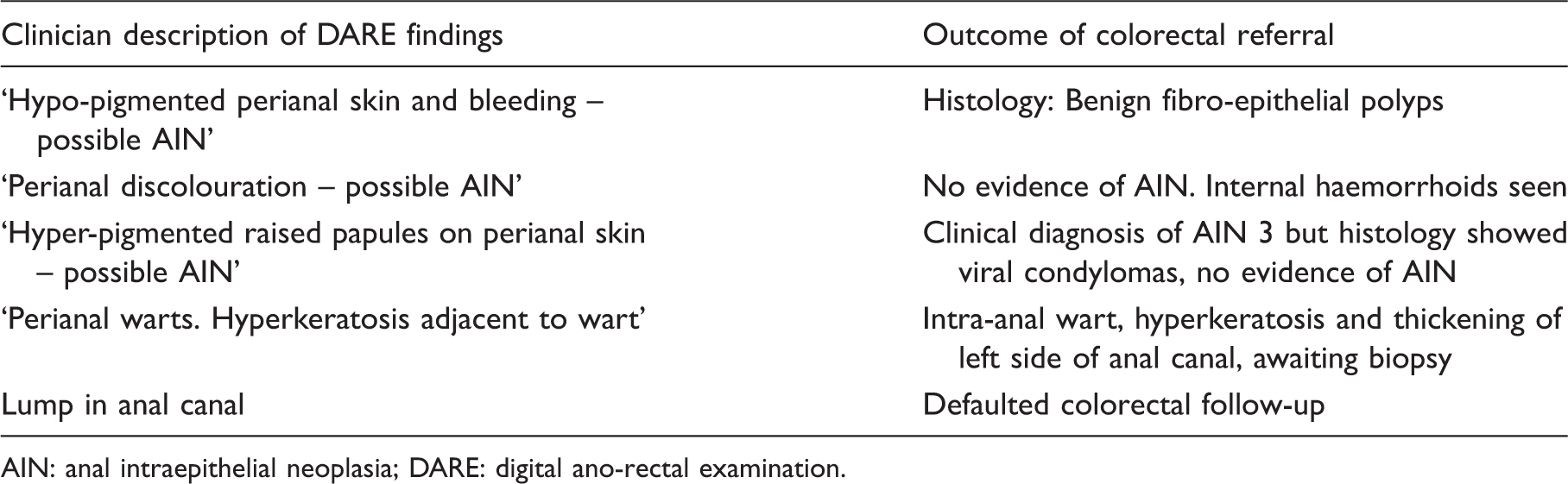
AIN: anal intraepithelial neoplasia; DARE: digital ano-rectal examination.
Less than 5% of patients reported significant discomfort or stated that having DARE was unpleasant. No patients reported significant pain or high levels of emotional upset by the examination; 100% of patients were satisfied with the amount of information given prior to the examination. The issue concerning most men was the worry that they might not be feeling clean. Four patients (14%; CI 1–27) expressed high levels of concern. One patient (3%) reported high levels of concern over losing control of his bowels during the examination; 100% of respondents said they would have DARE again.
Our service evaluation is limited by the small sample size yet results show that all men who consented for DARE were willing to continue with annual DARE. Principal reasons for refusal were time constraints and worry about ‘not being clean’. We also found that DARE may identify peri/intra-anal abnormalities of clinical significance needing onward referral. Forewarning patients to expect DARE at a routine visit when it is due, and providing information in advance about what DARE involves may further improve acceptability and uptake in clinic.