
Abstract
Mycoplasma genitalium is an important pathogen that is transmitted through sexual contact. For patients diagnosed with M. genitalium infection, the current guidelines recommend 1 g of azithromycin as the first-line treatment. Moxifloxacin is used as a second-line drug due to its remarkable efficacy; however, increased use of moxifloxacin to treat M. genitalium infections has caused the emergence of cases of moxifloxacin treatment failure. This meta-analysis aims to estimate the treatment efficacy of moxifloxacin for M. genitalium infection. Electronic databases were searched for articles published from 1983 to the end of May 2016 using the following search terms: (Mycoplasma genitalium) AND (moxifloxacin OR 1-cyclopropyl–7-(2,8-diazabicyclo(4.3.0)non-8-yl)-6-fluoro-8-methoxy-1,4-dihydro-4-oxo-3-quinoline carboxylic acid OR Proflox OR moxifloxacin hydrochloride OR Octegra OR Avelox OR Avalox OR Izilox OR Actira OR [treatment efficacy]). All included studies were published in English; all participants were diagnosed with M. genitalium infection, and microbial cure times were measured within 12 months after treatment. Treatment efficacy was measured as microbial cure at the final follow-up after treatment. In total, 17 studies including 252 participants met the inclusion criteria. The majority of these studies were observational. The random-effects pooled microbial cure rate was 96% (95% confidence interval [CI], 90%–99%; I2 = 28.59%, P = 0.13). For studies with sample collection deadlines prior to 2010, the pooled microbial cure rate was 100% (95% CI, 99%–100%; I2 = 0.00%, P = 1.00). For studies with sample collection deadlines of 2010 and later, the pooled microbial cure rate was 89% (95% CI, 82%–94%; I2 = 0.00%, P = 0.59). The elimination rate of moxifloxacin for M. genitalium infection has decreased from 100% to 89% since 2010. This decline merits considerable attention. We suggest close follow-up to investigate the efficacy of moxifloxacin for treating M. genitalium infections. Additionally, sentinel points should be established to detect mutations in the gyrA/B and parC/E genes, which are associated with moxifloxacin resistance.
Introduction
Mycoplasma genitalium 1 was first isolated from the urethras of two patients with non-gonococcal urethritis in 1983. Møller et al. 2 demonstrated a direct association between M. genitalium infection and female pelvic inflammation based on serologic evidence. 2 M. genitalium is implicated in the pathogenesis of cervicitis, pelvic inflammation, premature delivery, spontaneous abortion, rectal inflammation and infertility3–5 and promotes HIV transmission. 6 However, whether M. genitalium is associated with male infertility and genital tract tumors remains unclear.7–9
The infection rate of M. genitalium varies depending on the source of research samples. The infection rate of a population practicing low-risk sexual behaviors is approximately 2%, while the infection rate of a population practicing high-risk sexual behaviors is approximately 7.3%. 10 The M. genitalium infection rate among patients with non-gonococcal urethritis varies by area and year, ranging from 6% to 50%. 11 The first-line treatment regimens for M. genitalium infection include the following: 100 mg of doxycycline twice daily for seven days or azithromycin 500 mg stat, then 250 mg daily for the next four days.11,12 However, a number of randomized controlled trials (RCTs) have shown the clearance rate of doxycycline to be as low as 31–45%.13,14 Therefore, the universal treatment guidelines recommend azithromycin as the first-line drug to treat patients diagnosed with M. genitalium infection. In the past several years, the curative effects of this drug have exhibited a clear downward trend. According to a meta-analysis conducted in 2015, the clearance rate of azithromycin has declined to 67% since 2009. 15 In response, there has been a recent shift away from first-line azithromycin in some countries in an attempt to lessen the risk of inducing macrolide resistance in M. genitalium. In the event of azithromycin or doxycycline treatment failure, moxifloxacin, the most commonly used drug for the second-line treatment of M. genitalium infection, has excellent therapeutic effects. However, cases of moxifloxacin treatment failure were reported by Couldwell et al. 16 for the first time in 2013. Therefore, we conducted a systematic review and meta-analysis to assess the current efficacy of moxifloxacin for treating M. genitalium infections.
Methods
Review search strategy
We performed this systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. 17 We searched articles published between 1983 and May 2016. All articles examined the microbial cure rate following moxifloxacin treatment for M. genitalium infection in humans.
The following electronic bibliographic databases were searched: PubMed, Embase, Medline, and the Cochrane Central Register of Controlled Trials. We also searched for information on Google Scholar. The following search terms were used: (Mycoplasma genitalium) AND (moxifloxacin OR 1-cyclopropyl–7-(2,8-diazabicyclo (4.3.0) non-8-yl)-6-fluoro-8-methoxy-1, 4-dihydro-4-oxo-3-quinolinecarboxylic acid OR Proflox OR moxifloxacin hydrochloride OR Octegra OR Avelox OR Avalox OR Izilox OR Actira OR [treatment efficacy]). The resultant studies were reviewed, and information was independently extracted by two authors (Yang Li and Sai Li).
First, we categorized the articles retrieved to exclude case reports and reviews; second, we read the abstract of each article to determine whether the article might be related to the present research before downloading the whole paper. An article in Chinese was found by searching Google Scholar. However, the article was excluded because of poor quality. All of the remaining articles were written in English. All articles included in the meta-analysis had been peer-reviewed. The authors discussed any differences that arose. If a difference remained unsolved, resolution was determined by the third author (Xiao-Hong Su).
The specific inclusion criteria were as follows:
Articles published between 1980 and May 2016. Limitation of the period assessed for microbiological cure to within 12 months after treatment.
Articles with the following conditions were excluded:
Articles with inconsistent data or incoherence. Case reports or reviews.
Meta-analyses
Meta-analyses were performed to calculate a pooled estimate of microbial cure of moxifloxacin for the treatment of M. genitalium infection. All meta-analyses (including general analysis and sub-group analysis) were conducted with random-effects models. Heterogeneity was assessed using I2 statistics. I2 < 25% indicated no heterogeneity, and 25% ≤ I2 < 50% indicated a low level of heterogeneity; 50% ≤ I2 < 75% indicated a moderate level of heterogeneity. I2 ≥ 75% indicated a high level of heterogeneity. The data were analyzed using Stata software version 14.0. (STATA Corp., College Station, TX). The Mantel-Haenszel method with random-effects modeling was used to calculate ES and 95% CIs.
Subgroup analyses
Possible reasons for heterogeneity were explored by stratifying the results according to the disease course of treatment, whether moxifloxacin was selected after azithromycin or other antibiotic treatment failed, and whether the samples collected in these studies were grouped by deadline of sample collection. For the variable “study period,” time points were determined through meta regression analysis. It can be seen from Figure 1 that 2010 is an important turning point.
Meta-regression of efficacy and year.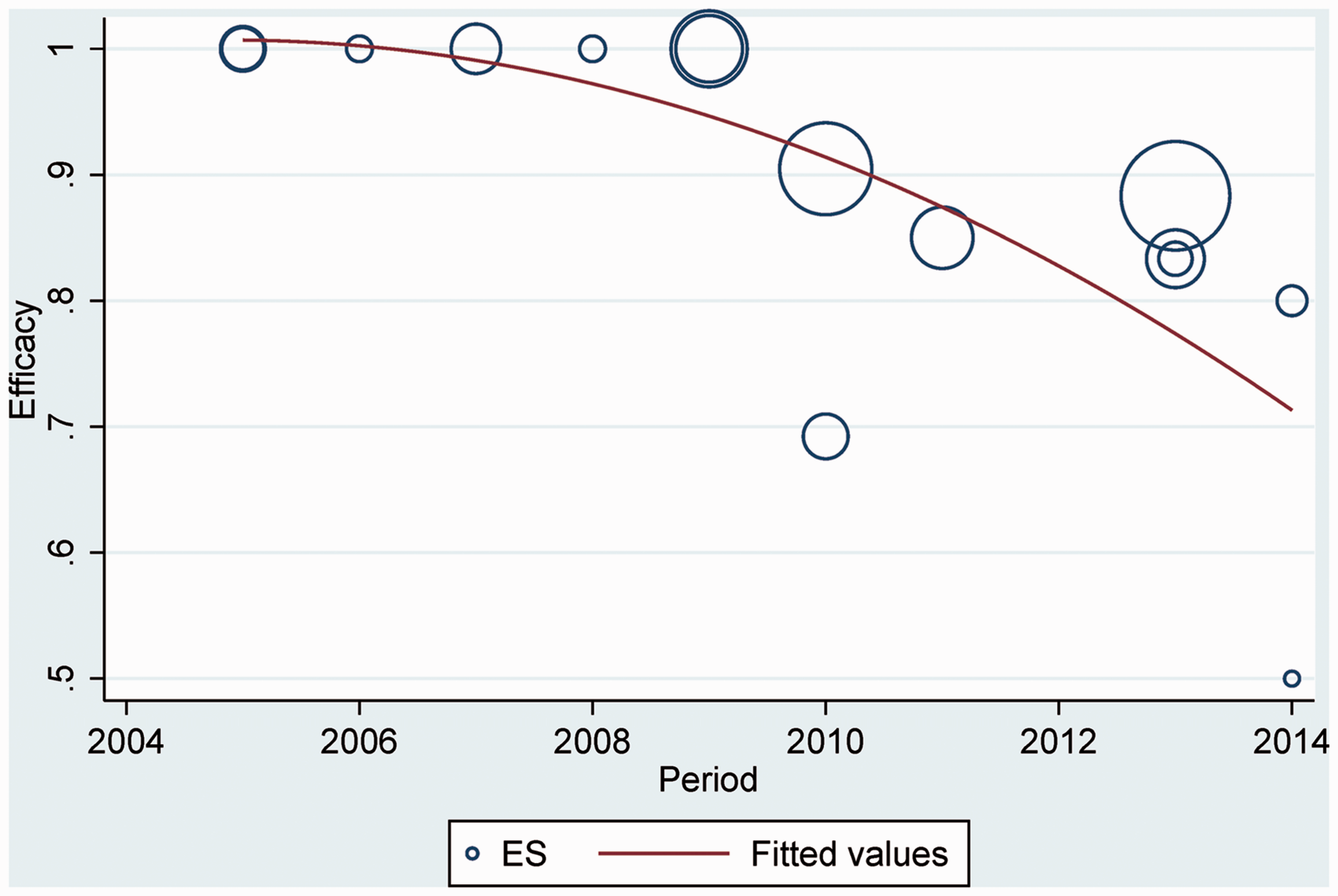
Bias and quality assessment
Publication bias was assessed using funnel plots, and asymmetry was statistically evaluated using Egger's and Begg’s correlation tests by regressing the treatment efficacy according to its standard error. Within-study bias for observational studies was assessed according to the evaluation criteria adopted by Sanderson et al. 18 in a systematic review of tools used to evaluate bias in observational studies.
Results
Selection of studies and basic characteristics of studies
In total, 17 articles were included in the present systematic review: 16 observational studies 16,19–33and one RCT.
34
The procedures for literature retrieval, inclusion, and exclusion are shown in Figure 2. See Table 1(a) and 1(b) for content summaries of the 17 articles.
Flow diagram of the selection of the studies. Summary of the 17 studies included in the analysis. Summary of risk of bias for included studies. +: low risk of bias; ++: medium risk of bias; +++: high risk of bias.


Moxifloxacin efficacy
The overall random-effects pooled microbial cure rate was 96.0% (95% CI, 90.0%–99.0%), and the heterogeneity was low (I2 = 28.59%, P = 0.13) (Figure 3).
Forest plot of the efficacy of moxifloxacin.
Subgroup analyses
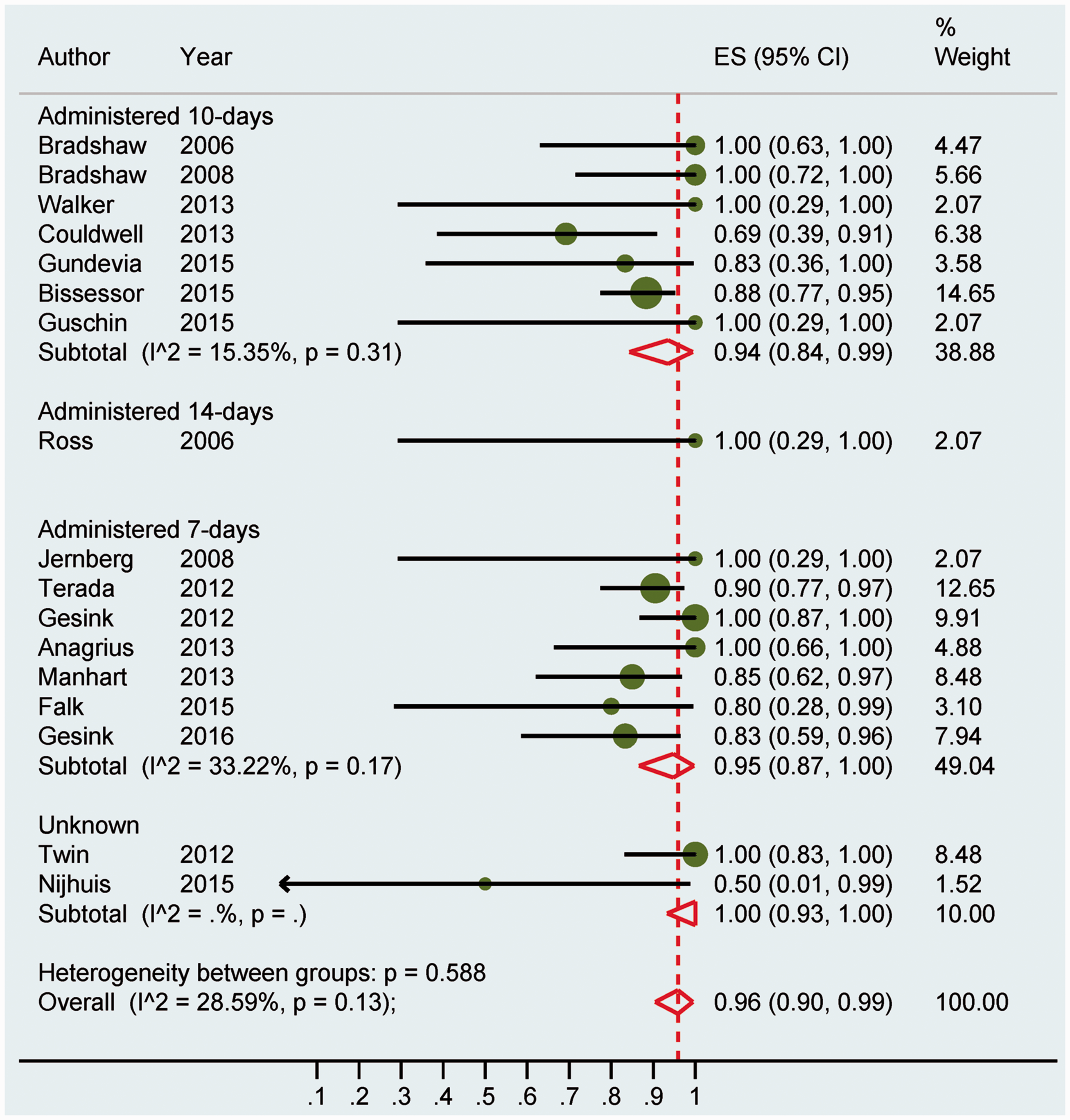
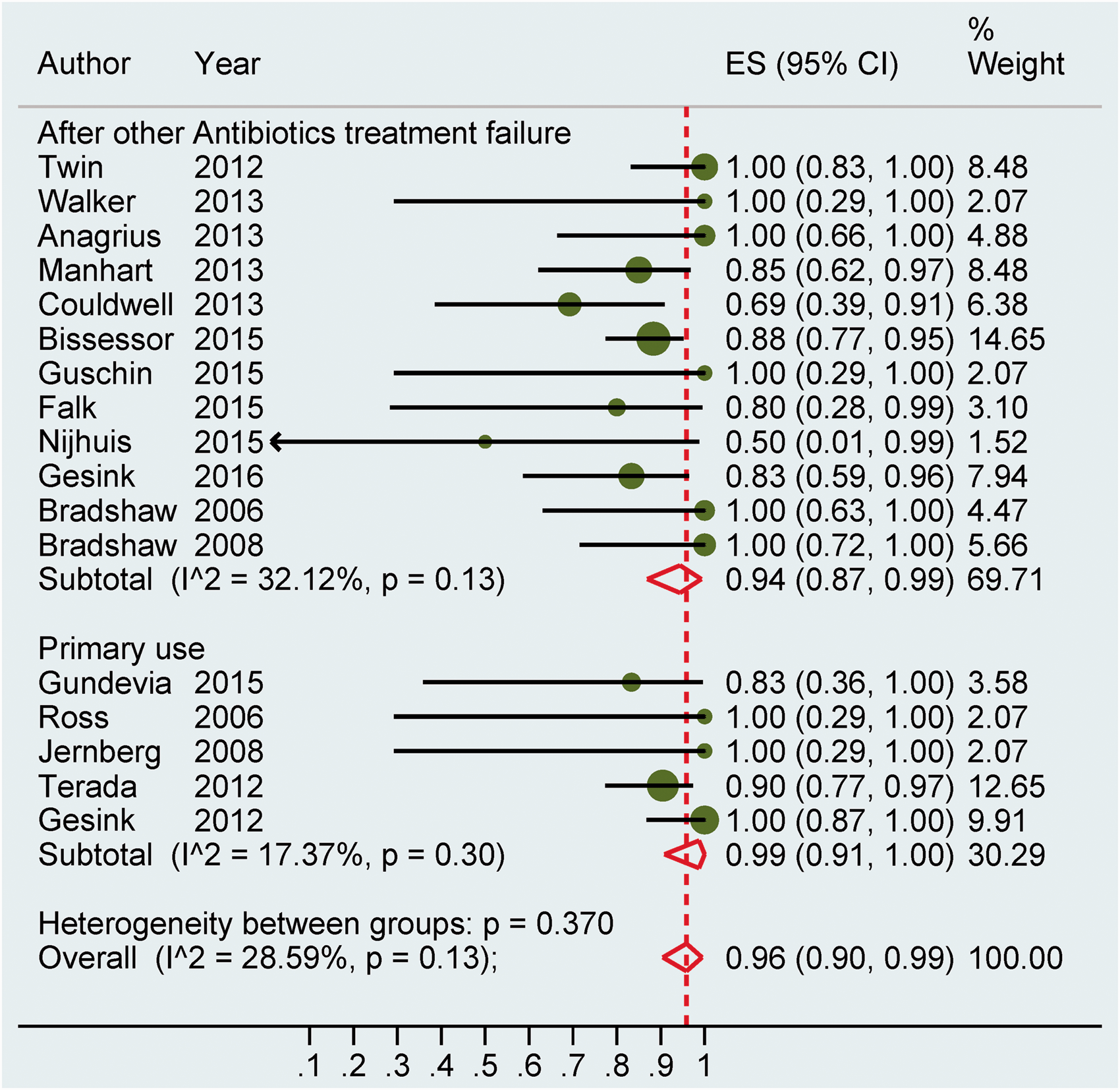
If the studies were grouped according to the years the researchers ended enrolled data collection, the pooled microbial cure rate prior to 2010 was 100% (95% CI, 99.0%–100.0%) with no heterogeneity (I2 = 0.00%, P = 1.00). The pooled microbial cure rate for studies in 2010 and later was 89% (95% CI, 82.0%–94.0%) with no heterogeneity (I2 =0.00%, P = 0.59) (see Figure 4); heterogeneity between sub-groups, P = 0.000. When stratified by the course of treatment, the pooled microbial cure rate for seven days of moxifloxacin administration was 95.0% (95% CI, 87.0%–100.0%) with low heterogeneity (I2 = 33.22%, P =0.17). The pooled microbial cure rate for 10 days of use was 94.0% (95% CI, 84.0%–99.0%) with no heterogeneity (I2 = 15.35%, P = 0.31) (see Figure 5); for the heterogeneity between sub-groups, P = 0.588. If the studies were grouped according to the initial use of moxifloxacin or the use of moxifloxacin after azithromycin or other antibiotic treatment failure, the pooled microbial cure rate for initial use was 99% (95% CI, 91.0%–100.0%) with no heterogeneity (I2 = 17.37%, P = 0.30). The pooled microbial cure rate for the use of moxifloxacin after azithromycin or other antibiotic treatment failure was 94% (95% CI, 87.0%–99.0%) with low heterogeneity (I2 = 32.12%, P = 0.13) (see Figure 6); for the heterogeneity between sub-groups, P = 0.370. Subgroup analysis based on enrolment deadline. Subgroup analysis based on duration of moxifloxacin treatment. Subgroup analysis based on treatment condition.

Study bias
Between-study bias
Funnel plots used to assess microbial cure following treatment with moxifloxacin for M. genitalium infection are shown in Figure 7. Egger’s test identified no publication bias (P = 0.963). Begg’s test also identified no publication bias (P =0.483).
Funnel plot of microbial cure following treatment with moxifloxacin.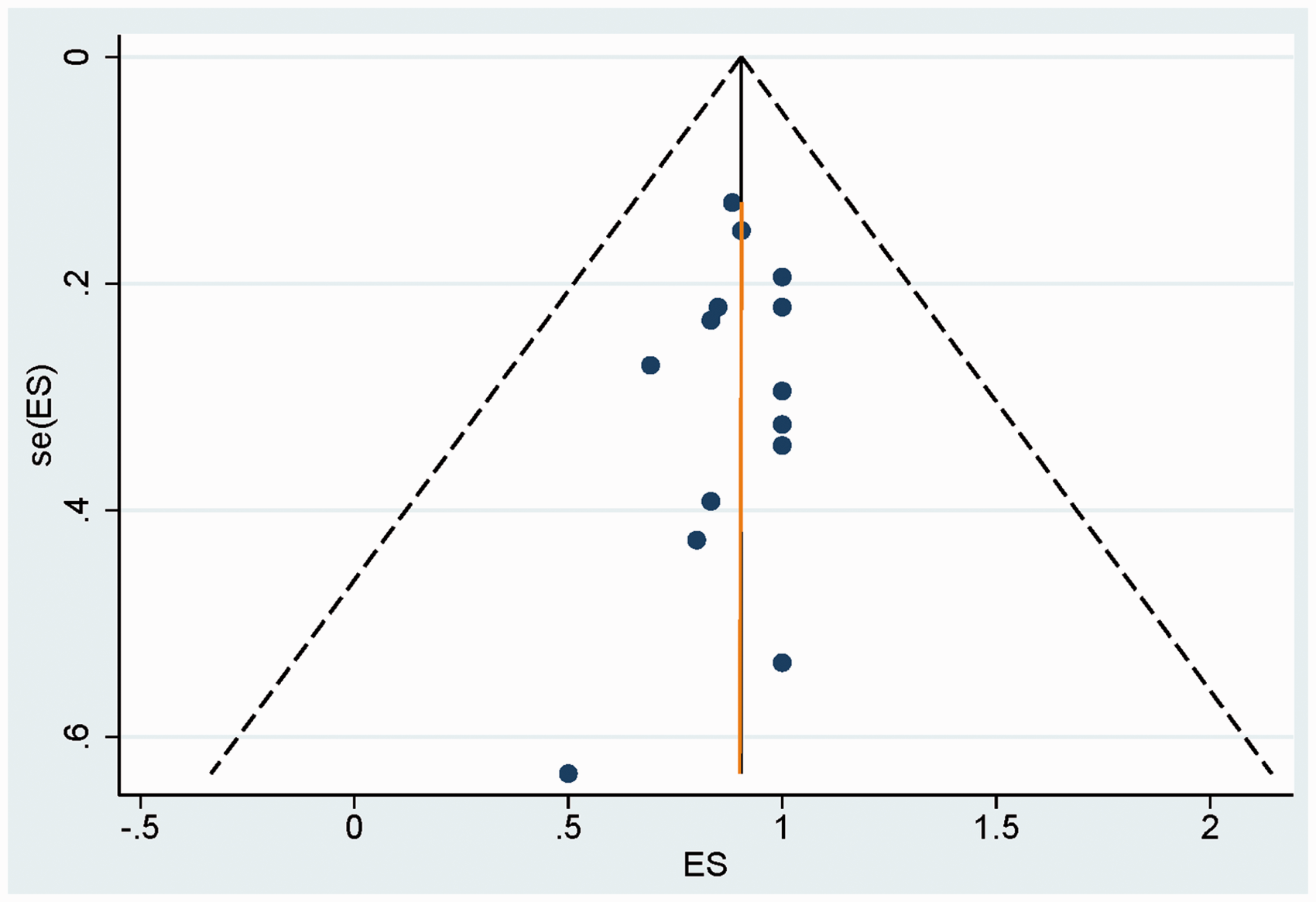
Within-study bias (see Table 2)
Most of the 17 studies included participants from sexually transmitted infection (STI) clinics. Only two studies enrolled participants from the general population.22,29 See the details in Table 1(b). Due to assessing microbial cure either too early or too late after treatment, several studies had high bias. 16,28–32 See the details in Table 1(a). The risk of loss to follow-up bias in most studies was low. See the details in Table 1(b). Given that moxifloxacin is often used as a second-line drug for those cases who failed treatment with first-line drugs, the sample sizes of most studies were very small (details in Table 1(a)).
Discussion
This systematic review and meta-analysis explored the clearance rate of moxifloxacin for the treatment of M. genitalium infection. The meta-analysis of publications over the past 10 years showed that the overall clearance rate of moxifloxacin for M. genitalium infection is 96%, with a low heterogeneity of 28.59%. It is clear that moxifloxacin still has excellent efficacy in treating M. genitalium infection. To detect the source of heterogeneity, we performed a series of sub-group analyses for duration of treatment, literature type, first use of moxifloxacin or not, and follow-up time of sample collection. It is generally considered that a longer course of antibiotic treatment results in a higher clearance rate. However, these sub-group analyses showed no significant differences between 7-day therapy and 10-day therapy. This conclusion remains to be further supported by experiments with a larger sample size. No difference was found in the sub-group analysis of first use of moxifloxacin or not. This lack of difference might exist because azithromycin and moxifloxacin have completely different mechanisms of action. The sub-group analysis of the sample collection deadline showed that microorganisms generally produced resistance to a type of antibiotics with an increased time of use. This process might be caused by selection pressure. To select a reasonable time point, the deadlines for sample collection in these articles were sorted, revealing that 2010 shows an obvious downtrend in clearance rates. A further sub-group analysis has confirmed this observation, and the clearance rate of moxifloxacin declined from 100% to 89%, a significant downtrend. Although the literature resources included in this meta-analysis mainly consisted of observational experiments and included only limited samples, the results still hold important practical value to guide clinical treatment.
Moxifloxacin is an extended-spectrum quinolone antibiotic that was developed by Dalhoff et al. 35 Bébéar et al. 36 first studied the in vitro antimicrobial activity of this drug against Mycoplasma (M. pneumoniae, M. genitalium, M. hominis, M. fermentans, M. penetrans and U. urealyticum) and noted its remarkable antimicrobial activity. Among three quinolone drugs, Hamasuna et al. 37 observed the lowest MICs, ranging from 0.03 to 0.5 mg/l, for moxifloxacin against M. genitalium; ciprofloxacin and levofloxacin demonstrated poor in vitro antimicrobial activity (MICs: 0.5 to 16 mg/l and 0.25 to 4 mg/l, respectively). Bébéar et al. 38 and Hamasuna et al. 39 further confirmed the above observations with in vitro experiments.
In the recent European Guideline on NGU therapy, 12 doxycycline is recommended as a first-choice drug for patients with no definitive M. genitalium infection. For patients with definitive M. genitalium infection, 500 mg of azithromycin stat followed by 250 mg (od) for four days is recommended. However, a meta-analysis 15 suggested that 1 g of azithromycin has had a pooled microbial cure rate of 67% since the beginning of 2009. Therefore, as a recommended second-line drug, moxifloxacin will be utilized more frequently to overcome azithromycin treatment failure.
Due to the extensive use of moxifloxacin to treat M. genitalium infection, greater numbers of M. genitalium bacterial strains demonstrating moxifloxacin resistance are likely to evolve. Couldwell et al. 16 reported cases of moxifloxacin treatment failure for samples collected between 2008 and March 2010. In total, 13 cases of azithromycin treatment failure received moxifloxacin treatment, and 4 patients reportedly failed with an oral dosage of 400 mg for 10 consecutive days. However, the observation end points were not specified. Manhart et al. 23 reported three cases of moxifloxacin treatment failure in the same year, and these samples were collected from January 2007 to July 2011. The dosage was 400 mg of moxifloxacin for seven consecutive days. The end point was 42–63 days after the end of treatment. Because the research periods partially overlapped, we were unable to determine whether the cases of failure following treatment with moxifloxacin first occurred in the United States or Australia.
Several studies have evaluated the association between mutations in topoisomerases and quinolone resistance. By selecting ciprofloxacin-resistant mutant strains, Yamaguchi et al. 40 confirmed that Gly81Cys in the parC quinolone resistance-determining region (QRDR) contributed to quinolone resistance in M. genitalium. The MICs of moxifloxacin in the ciprofloxacin-selected mutant strain also increased 4-fold as compared with that of the parent strain.
Deguchi et al. 41 used sitafloxacin, a third-generation quinolone similar to moxifloxacin, to examine levofloxacin-induced resistance in M. genitalium and observed the retention of excellent antimicrobial activity by sitafloxacin. Among the 17 articles included in this meta-analysis, only 3 articles16,24,27 detected the gyrA gene and parC gene in samples. There were 10 cases of treatment failure with a confirmed genotypic association, including 5 cases involving the joint mutation of gyrA and parC, 1 case with a single mutation of gyrA and 4 cases with a single mutation of parC. Moxifloxacin resistance-associated mutations in gyrA and parC genes presented in all 10 cases before treatment with moxifloxacin.16,24
We conducted a systematic review to assess the efficacy of moxifloxacin for the treatment of M. genitalium infection. Although the overall efficacy rate of moxifloxacin is as high at 96%, its clearance rate has obviously declined since 2010. The evidence of emerging quinolone resistance in M. genitalium and treatment failure with moxifloxacin is of great concern. For patients with persistent M. genitalium infection, one of the recommended third-line treatments is pristinamycin 1 g four times daily for 10 days. 42 Pristinamycin was highly effective in treating macrolide- and quinolone-resistant strains. 24
Study strengths and future prospects
This report is the first meta-analysis of the treatment effect of moxifloxacin in the context of M. genitalium infection. Moxifloxacin is the most effective drug for treating M. genitalium infection identified to date, but its efficacy has clearly declined. Multicenter M. genitalium resistance monitoring networks should be established as quickly as possible. Due to increasing treatment failure with moxifloxacin, it is crucial that new treatment regimens for M. genitalium infection are investigated.
Study limitations
Most of the articles included in this study are clinical observational studies of low quality. A wide range of final observation end points was used to determine whether infection was eliminated. Therefore, there is a possibility that all failure cases had actually been cured but that these subjects subsequently had unprotected intercourse with their sex partners, leading to re-infection. This phenomenon may explain the so-called failure cases. The longer the time interval between final observation end points, the higher the risk. Selective publication bias may exist, and more-recent articles tend to publish more failure cases.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.