
Abstract
There are no evidence-based guidelines for the treatment of Mycoplasma genitalium-positive genital infection. In a retrospective survey, we analysed the treatment results of patients tested for M. genitalium at Olafia, Unit for Sexual Transmitted Diseases in Oslo. Out of 10,109 patients, 452 had a positive polymerase chain reaction. Between 72% and 100% of patients in the different treatment groups returned for test of cure after four to five weeks. First-line treatment with 1 g single dose azithromycin had a recovery rate of 79%. It was as effective as an extended five-days’ course of azithromycin. Ofloxacin 200 mg b.i.d for 10 days cured 56% and moxifloxacin 400 mg o.d. for seven days as either second-, third- or fourth-line treatment after azithromycin or ofloxacin failure cured 100%. Azithromycin 1 g as a single dose seems to be the best choice of treatment for M. genitalium, with moxifloxacin 400 mg × 1 for seven days if treatment fails.
Introduction
Mycoplasma genitalium was first isolated in 1980 from two men with urethritis. 1 The difficulties in isolating the microbe by culture, made further clinical studies on M. genitalium problematic for a long time. However, the development of nucleic acid amplification tests has allowed detailed clinical studies, the first of which were published in 1993.2,3 Since then, many studies on the microbe and its connection to clinical disease have been conducted and it is now accepted that M. genitalium is sexually transmitted, causing urethritis in men and women and cervicitis in women. M. genitalium most likely also causes upper genital infection in women. 4 In vitro studies suggest that the organism is susceptible to tetracyclines, macrolides and most of the fluoroquinolones,5–7 although reduced susceptibility to tetracyclines and some macrolides and fluoroquinolones has been reported.7–9
There are no evidence-based guidelines for the treatment of M. genitalium-positive genital infection. However, a randomized, double-blinded treatment study comparing doxycycline with azithromycin in men has been designed and started recruitment in July 2007. 10 Open clinical studies have shown a high failure rate of doxycycline and levofloxacin, whereas azithromycin seems to be more efficacious.7,11–16 One of these studies, published as an abstract only, was a randomized study that compared azithromycin 1 g in a single dose with doxycycline 100 mg b.i.d for seven days. 16 This study confirmed the superior efficacy of azithromycin with a failure rate of 16% compared with 64% in the latter group. A recent study, however, reports a significant failure rate of 28% after 1 g azithromycin, but a 100% efficacy and a high in vitro susceptibility to moxifloxacin. 17
In Norway, 1 g stat. of azithromycin is routinely given for treatment of non-gonococcal urethritis/cervicitis (NGU). In Sweden, a seven-days’ course of doxycycline is used. 10 Our hypothesis, when we started testing all our patients for M. genitalium, was that azithromycin had a lower cure rate in Norway than in Sweden. We rationalized that this may have resulted from inadvertent selection of azithromycin-resistant M. genitalium strains in Norwegian patients. It is therefore of interest to know if general treatment of non-gonococcal urethritis/cervicitis patients with azithromycin has led to higher treatment failures of M. gentialium infection with azithromycin.
In this article, we describe the results from a retrospective survey of treatment of patients who were tested for M. genitalium at Olafiaklinikken, a drop-in clinic for sexually transmitted infections in Oslo, Norway.
Material and Method
From May 2005 through December 2006, 10,109 patients were tested for M. genitalium at Olafiaklinikken. The patients tested had either symptoms of sexually transmitted infections or they had a sexual partner with diagnosed urethritis/cervicitis or a partner with laboratory verified M. genitalium or Chlamydia trachomatis infection. Urethritis and cervicitis were diagnosed clinically and by microscopic examination of stained urethral smear obtained with a metal curette in men, and stained urethra and cervical smears as well as vaginal smears in women. Patients that were diagnosed with NGU at their first visit were given a single dose of azithromycin 1 g before laboratory test results for M. genitalium and C. trachomatis were available. Partners of index patients diagnosed with NGU were examined and treated regardless of symptoms or signs.
To test for M. genitalium, first void urine was collected from both men and women. In addition, an endocervical/vaginal swab was collected from women, using a sterile sexually transmitted disease swab (Amplicor® STD Swab, Roche Molecular Systems Inc., Branchburg, NJ, USA). Urine and cervical swabs were sent to Fürst Medisinsk Laboratorium in Oslo for analysis. In addition to being examined for M. genitalium by realtime polymerase chain reaction, 18 the specimens were examined for C. trachomatis using the Roche Cobas amplicor. M. genitalium-positive patients were called back for a follow-up visit, four to five weeks after the initiation of treatment. If patients were positive for M. genitalium from specimens taken in the follow-up test, they were given a new treatment and asked to come back for a second follow-up visit after four to five weeks. This regimen was kept up until the patient tested negative. Patients were also questioned to assess the possible reinfection from untreated partner. In cases of obvious reinfection, the patient was registered as a new case in this study and not as treatment failure.
In the later stages of the study period, we introduced a new treatment regimen, whereby the patients received an additional dose of azithromycin 1 g within five to seven days after the first dose given for NGU, if results from urine and/or cervical/vaginal swab subsequently showed M. genitalium infection.
If the patient had not been treated on the first visit, and laboratory test results for M. genitalium proved positive, a five-day treatment with azithromycin, 500 mg day 1 and 250 mg the following four days, was given as a first-line treatment. Typically, this started one to two weeks after the patients’ first visit.
As a second or third-line treatment, a five-days azithromycin regimen as described above, ofloxacin 200 mg b.i.d. for 10 days or moxifloxacin 400 mg stat. for seven days was given, depending on what medication the patient had been given previously. Moxifloxacin was the only medication given as a fourth-line treatment.
When patients were diagnosed with urethritis/cervicitis or a laboratory-verified M. genitalium or C. trachomatis infection, they were told to abstain from sexual contact during the treatment or at least one week after the single dose treatment and until their current partner also had been examined, tested and treated. Despite the intention of keeping ofloxacin and moxifloxacin as second-, third- or fourth-line treatments, a small number of patients were given one of these medicaments as a first-line treatment. These were mainly new partners who received their first treatment somewhat later, when the index patients’ infection had not been successfully eradicated with azithromycin.
After deletion of identification, the patient data were analysed in the program Epi-Info. Local Ethics Committee approved the study.
Results
A total of 10,109 patients were tested for M. genitalium, 5423 men and 4683 women. In three cases, information about the patient's gender was missing. Four hundred and fifty-two (4.5%) were shown to have M. genitalium infection, 234 (4.3%) men and 218 (4.7%) women. Forty-eight patients (10.6%) had a co-infection with C. trachomatis.
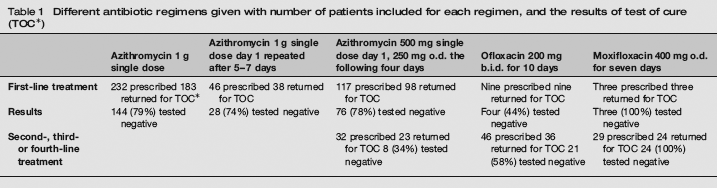
The results of different regimens are summarized in Table 1 and described below.
Different antibiotic regimens given with number of patients included for each regimen, and the results of test of cure (TOC*)
Azithromycin
Altogether 232 patients with a positive test for M. genitalium were given a single dose of azithromycin 1 g as first-line treatment. One hundred and eighty-three (79%) of them attended for the follow-up visit and of those, 144 (79%) had a negative test of cure (TOC).
Forty-six patients received a first-line treatment of azithromycin 1 g on day 1 and another 1 g after five to seven days. Out of the 38 (83%) who came back for TOC, 28 (74%) tested negative.
One hundred and seventeen patients were given a five-day treatment with azithromycin as a first-line treatment, 500 mg on day 1 and 250 mg o.d. the following four days. Ninety-eight (84%) returned for TOC and 76 (78%) tested negative.
Thirty-two patients were given the five-day treatment with azithromycin as a second or third-line treatment, after having tested positive on the follow-up visit. Twenty-three (72%) of the patients came for TOC and 8 (34%) tested negative.
Ofloxacin
Ofloxacin 200 mg × 2 for 10 days was given as a first-line treatment to nine of the patients with M. genitalium infection. These were mainly partners of patients who had had an ineffective azithromycin treatment. All nine (100%) came back for TOC on which four (44%) of them tested negative.
Forty-six patients were prescribed ofloxacin as a second- or third-line treatment. Thirty-six (78%) of them returned for TOC, and 21 (58%) tested negative.
Altogether 55 patients were given ofloxacin as a first-, second- or third-line of treatment after having tested positive for M. genitalium. Out of the 45 (82%) patients who came back for TOC, 25 (56%) tested negative.
Moxifloxacin
Thirty-two patients were given moxifloxacin following a positive test for M. genitalium, three as first-line treatment of partners who had treatment failures and 29 as second to fourth-line treatment. Twenty-seven (84%) came back for TOC on which they all (100%) tested negative.
Side-effects
Moxifloxacin has been associated with hepatic failure and serious skin reactions, such as toxic epidermal necrolysis. While rare, these side-effects can be life-threatening. We have not seen any side-effects in our patients, except a high rate of gastrointestinal complaints after treatment with azithromycin. Taking azithromycin with food reduces these side-effects.
Discussion
Our early clinical impression, when we first started testing patients with NGU for M. genitalium, was that the treatment failure after 1 g stat dose azithromycin was higher than the near 100% efficacy reported from small studies in Sweden.11,13 This study, where we evaluated the efficacy of different treatment regimens against M. genitalium based on laboratory findings, confirmed our preliminary observations, we found a higher treatment failure than reported from Sweden. An explanation could be the selection of azithromycin-resistant strains due to routine treatment of patients with NGU with azithromycin in Norway. In Sweden, doxycycline is used as first-line treatment for this condition.11,12,19 Another explanation could be that azithromycin-resistant strains are susceptible to tetracycline and eradicated with the first treatment. Despite geographical proximity and travel between Norway and Sweden, differences in strains of sexually transmitted infectious isolates have been observed, such as the cryptic plasmid variant strain of C. trachomatis that is found in 20–40% of patients in some geographical regions of Sweden, 20 but seldom in Norway. It is therefore of clinical interest to determine if treatment of M. genitalium with azithromycin is still the method of choice if observed failure rates are higher than in neighbouring countries, and to determine the most effective dose. Previous studies have concluded that azithromycin is more efficient against M. genitalium than doxycycline11–13 in particular when given as an extended five-day course. 15 There have been discussions about the most suitable azithromycin regimen for best cure, a single dose of 1 g stat or a five-day treatment where the patient is given 500 mg day 1 followed by 250 mg daily for four days. 11
In our study, we compared three different azithromycin treatment regimens, a single dose of 1 g, a single 1 g dose with an extra 1 g given after one week and 1.5 g over five days. They all showed similar efficacy with 74–79% microbiological cure when given as a first-line treatment. This is similar to the clearance rate of 72% in an Australian study. 17 It is worth noting that the five-day treatment, when given as a second or third-line treatment, seems to have a poorer clearance compared to the same regimen given as a first-line treatment. Most of the patients who received the five-day regimen as a second or third-line treatment had already been given azithromycin 1 g as a first-line treatment for NGU. A logical conclusion is that many of these patients had an azithromycin-resistant M. genitalium infection, making the five-day treatment no more efficient than the single dose.
A relatively small number of patients were given ofloxacin as a first-, second- or third-line treatment. However, the number of patients testing negative after this treatment was low.
Moxifloxacin was effective at treating all our cases of M. genitalium infection. This finding is similar to that of Bradshaw et al. 17 who concludes that treatment with moxifloxacin is effective in eradicating macrolide-resistant M. genitalium isolates. 17 Moxifloxacin is not registered in Norway, but is available on special license and five times more expensive than azithromycin and ofloxacin. Moxifloxacin is thus mainly used in cases of azithromycin treatment failure, which is in accordance with recommendations. 21 Treatment of genital chlamydia and NGU is free of charge due to the legislation in Norway, but M. genitalium infection is not included in the law and patients have to pay for this treatment. In cases of persistent NGU, a clinical recommendation has been to switch to tetracyclines if there is clinical failure with macrolides. We have isolated M. genitalium in many of these cases, with successful eradication and clinical cure after treatment with moxifloxacin.
In summary, we found that azithromycin is the drug of choice when M. genitalium infection is detected or suspected. A dose of 1 g stat seems to be as effective as 1 g single dose followed by 1 g a week later, or a five-day regimen. One-dosage treatment is the simplest treatment, with the highest compliance, and the least expensive. In cases of persistent infection after treatment failure with azithromycin, moxifloxacin seems to be the best choice. A seven-day course of moxifloxacin seems to have the same high efficacy as a 10 days course. 17 Moxifloxacin may also be a choice in cases of recurrent urethritis in clinics that do not have access to M. genitalium testing.
Addendum
Azithromycin 1 g as a single dose was shown to be as effective as a five days regimen. However, after finishing this study, it has been shown that a single dose of azithromycin may induce resistance in Mycoplasma genitalium. The gene for this resistance has been localized (Jensen JS, personal communication). The use of azithromycin 1 g stat as first line treatment for non-gonococcal urethritis in Norway instead of doxycycline, which is used in Sweden, may be the reason for the higher treatment failure of azithromycin in Norway. Therefore, it may be advisable to use doxycycline as first line treatment of non-gonococcal urethritis. As second line treatment, if there is treatment failure or positive PCR for M. genitalium, a five days' course of azithromycin is given, 500 mg day 1 followed by 250 mg daily for four days, as recommended by Bjornelius et al. 15
Footnotes
Acknowledgements
Fúrst Medical Laboratory provided funding for the project. The authors acknowledge the assistance of the nurses and physicians at the Olafia Clinic who wholeheartedly facilitated and supported the study.