
Abstract
In April 2013, local authorities gained responsibility for commissioning sexual health services in England. With many services going out to tender and resultant change in services or service provider, there is anecdotal evidence that this has impacted on the education, training and morale of genitourinary medicine (GUM) trainees. The aim of this study was to evaluate the impact of tendering on GUM trainees. An electronic survey designed by the British Association for Sexual Health and HIV Trainees’ Collaborative for Audit, Research and Quality Improvement Projects (T-CARQ) was distributed to GUM trainees and newly appointed consultants. Eighty-two individuals responded (74% GUM trainees, 25% newly appointed consultants, 1% locum appointed for service). Sixty-three per cent (45/72) had experience of training within a service which was being tendered. Of these, 59% (24/41) felt their training was not considered during the tendering process and 20% (8/41) felt that it was. Forty-four per cent (18/41) felt adequately supported. Thirty per cent (12/40) reported active participation in the tendering process. On a scale of 0 (no impact) to 5 (major impact), the median score for impact of tendering on training was 2. The positive/negative impact of tendering on different training elements was rated: other than management experience the overall impact on all parameters was negative, namely morale, senior support and education. In conclusion, this survey describes the variable impact of service tendering on GUM training. Our recommendations for maintaining training standards despite tendering include actively involving trainees and education partners, inclusion of specialist GUM training in service specifications, development of guidance for commissioners and services for the management of GUM training within tendering.
Background
In April 2013, following The Health and Social Care Act in England, local authorities became responsible for the commissioning of sexual health services as well as HIV prevention and testing services. HIV services (other than prevention and testing) remained commissioned by the NHS as a specialist service. 1
As a result of these changes, many sexual health services have been tendered and some taken over by new providers. The British Association for Sexual Health (BASHH) lead clinicians survey in 2014 showed that out of a total of 280 services in the United Kingdom, one-third had had their service tendered. There have been concerns nationally that these changes could result in a destabilisation of sexual heath provision, fragmentation of services and poorer patient care. 1 This uncertainty has led to concerns about the quality of postgraduate medical education and training within affected services. There are currently no published guidance or support documents specifically addressing the issue of managing genitourinary medicine (GUM) trainees and training during the tendering process.
Aims
In 2015, the BASHH Trainees’ Collaborative for Audit, Research and Quality Improvement Projects (T-CARQ) created a survey that was distributed to trainees and newly appointed consultants (who had been through tendering as trainees) to establish the impact of the tendering process on trainees.
Methods
The survey was designed by core members of T-CARQ and reviewed by the BASHH board and Chair of the GUM Specialist Advisory Committee. All GUM trainees, doctors in locum appointment for service (LAS) posts and newly appointed consultants who had experienced the tendering process as a trainee, were invited to complete the survey via an electronic survey platform. 2 Invitations were distributed via the BASHH newsletter, regional trainee representatives and via the T-CARQ twitter account (@BASHH_TCARQ). From the most recent GUM Specialist Advisory Committee meeting it is estimated that the total number of GUM trainees nationally is between 123 and 134.
Results
There were 83 responses to the survey. One response was excluded from further analysis as it was not from a trainee or newly appointed consultant, leaving 82 responses for analysis.
Demographics
GUM trainees made up 72% (59/82) of respondents (grades ST3–6). The remainder consisted of one LAS doctor and 20 (24%) newly appointed consultants; two respondents did not provide their grade of training. Responses were received from trainees from all English Local Education and Training Board areas (76/82, 92.7%) and from Scotland (7.3%, 6/82). London trainees were the largest represented group (34%, 28/82). No responses were received from Wales and Northern Ireland although trainees in these areas and Scotland are not affected by the changes in the Health and Social Care Act. However, as trainees may move between deaneries in their career, all were invited to participate.
Understanding of tendering
When asked to describe their understanding of tendering in relation to sexual health services 64 (78%) responded. Three members of the T-CARQ core committee independently assessed answers, with the majority view taken as to whether they were correct: 70% (45/64) accurately described the meaning of tendering, 54% (44/82) had read relevant tendering documents and 77% (53/69) wanted to learn more about the process.
Experience of the tendering process
Survey respondents were divided into two groups: those who had worked in any service that had been tendered during the past five years (Group A, 62.5%, 45/72) or those who had not (Group B, 37.5%, 27/72). Within Group B, 6 (8%) were in a pre-tender phase, 14 (19%) had not experienced tendering at all and seven (10%) ‘Did not know’. Ten trainees did not respond to this question.
In Group A, 22% (9/41) reported tendering of HIV, 61% (25/41) GUM, 39% (16/41) sexual and reproductive healthcare (SRH) and 56% (23/41) integrated GUM and SRH services. The remainder did not know. Where GUM, SRH and HIV services were all tendered, 32% (8/25) reported that these were tendered together, 40% (10/25) separately, 16% (4/25) did not know and 12% (3/25) reported ‘other’ (two lost HIV services in the tender, one reported previously separate services merged).
An NHS provider won the tender in 83% of cases (33/40). The remaining nine respondents did not know (1/42), had pending results (7/42) or worked in services won by a non-NHS provider (1/42).
Consideration of training needs during the tendering process
In Group B, 52.4% (11/21) anticipated that provision and delivery of their training programme would be considered within tendering, whereas 19.5% (8/41) of Group A respondents felt that this had actually happened. In terms of specific individual training needs, 14% (3/21) of Group B but only 9.76% (4/41) of Group A felt that these would be or had been considered, respectively.
Trainee support during tendering
Sources of support for trainees.
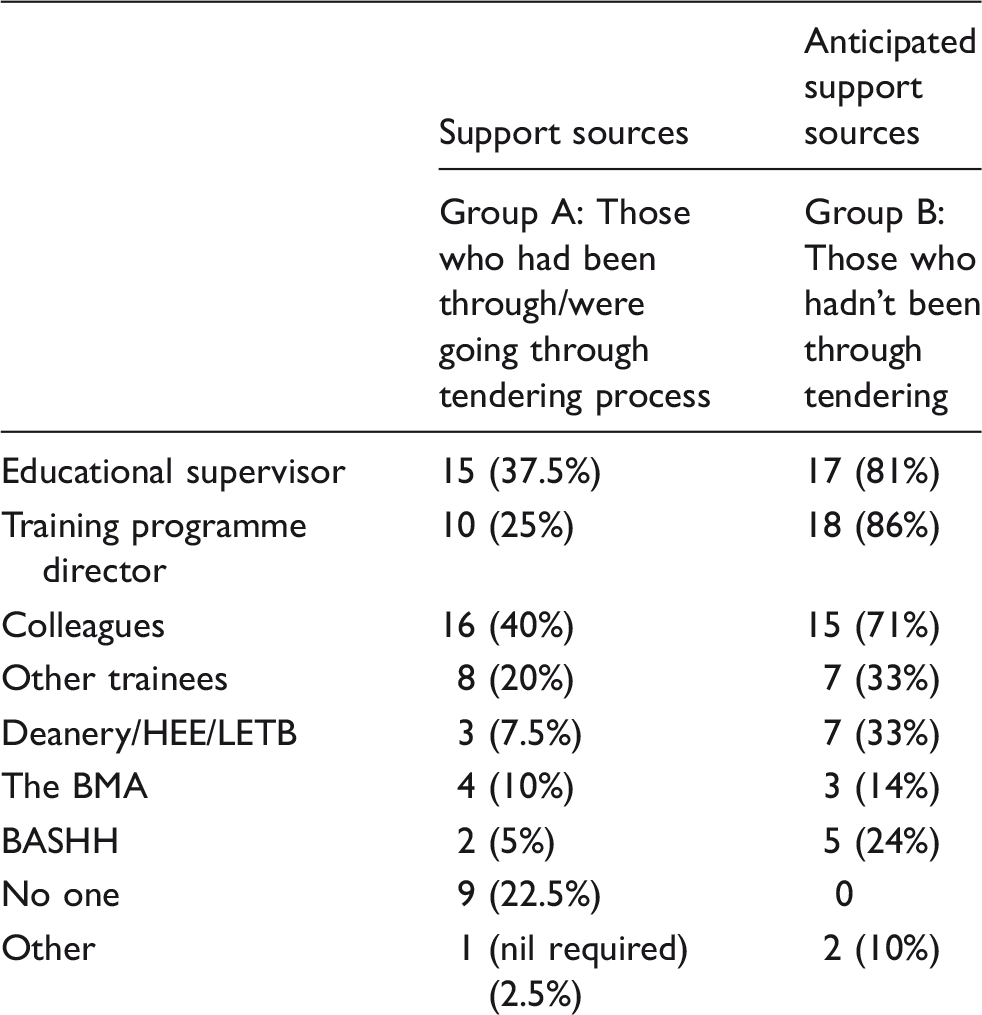
BASHH: British Association for Sexual Health; BMA: British Medical Association; HEE: Health Education England; LETB: Local Education and Training Board.
Group A rated how useful they found the support they had received, on a scale of 0–5 (0: not helpful at all to 5: extremely helpful). Median score was four (range 0–5).
Communication to and involvement of trainees during the tendering process
In Group A, 32.5% (13/40) felt that any changes during and following tendering were communicated in a timely and appropriate manner. Similarly 33% (7/21) of those in Group B felt there would be adequate communication.
In Group A, 30% (12/40) felt actively involved and encouraged to contribute to tender-related meetings and decisions whereas 33% of Group B (7/21) anticipated active involvement.
Impact of tendering on training
Respondents were asked to rate the impact the tendering process on their training on a scale from 0 to 5 (0: no impact to 5: major impact). The median response was two (range 0–5) for Group A and four (range 0–5) for the tendering naive (Group B).
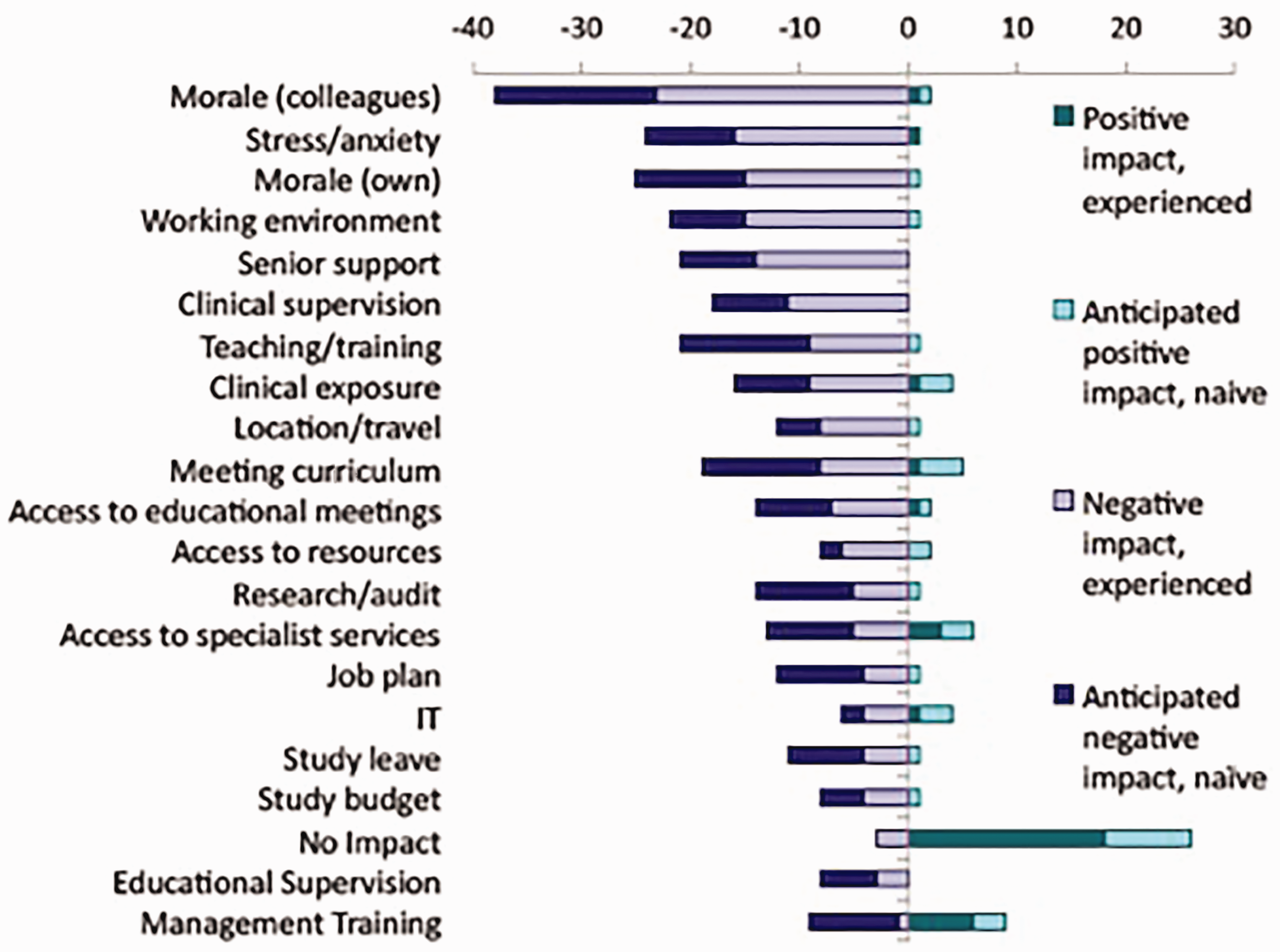
When Group A were asked whether this impact had been positive or negative on a scale from −5 to +5 (−5: major negative impact to +5 major positive impact), the median response was zero (range −5 to 3). Figure 1 demonstrates the spread of these results. Figure 2 demonstrates how respondents felt the different training areas were/would be impacted positively and negatively.
Assessing the positive/negative impact of tendering on training in tendering experienced trainees (Group A). Areas of training impacted by tendering. Experienced and anticipated impacts of tendering for trainees.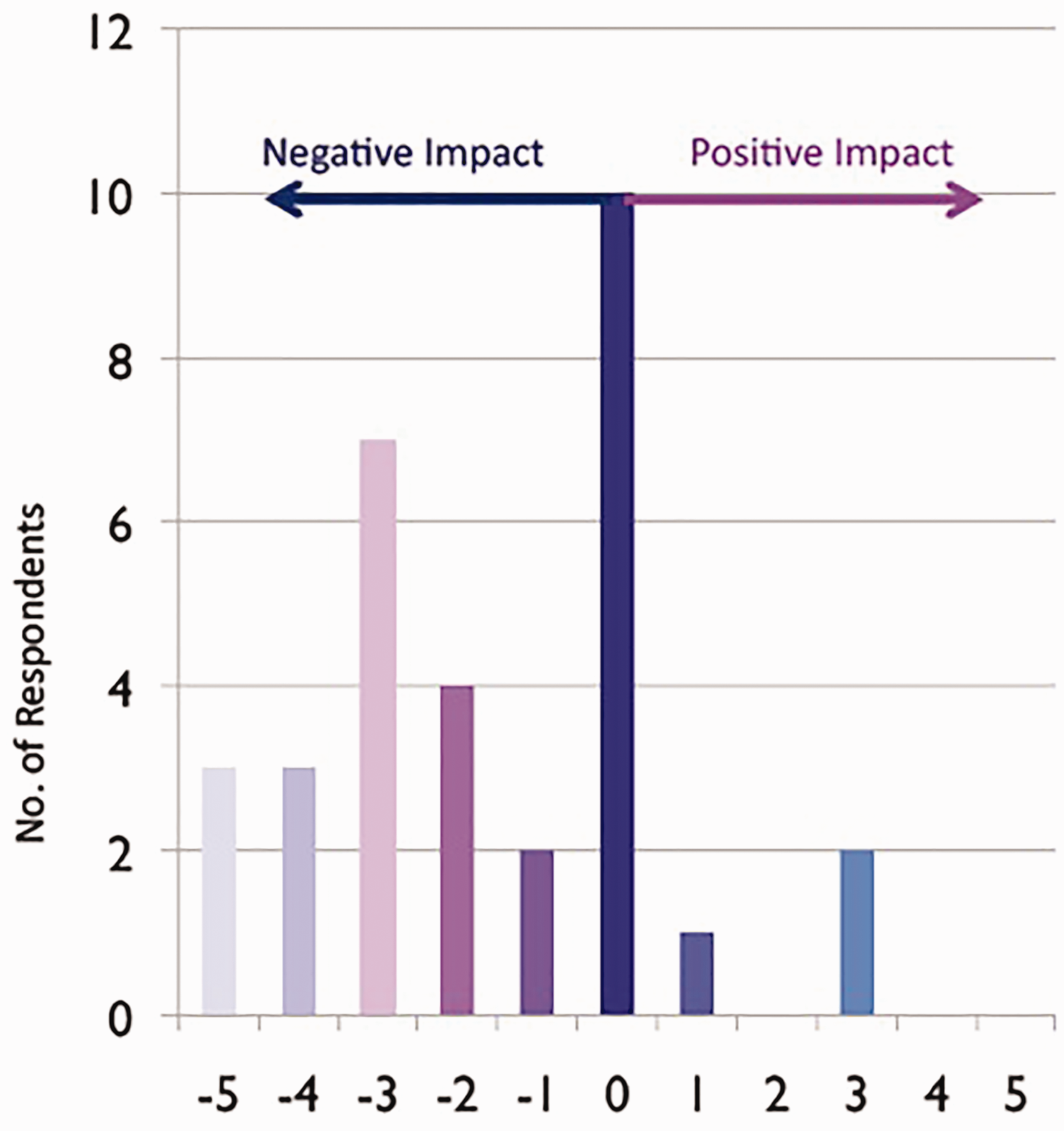
How can services undergoing tendering minimise the impact on trainees?
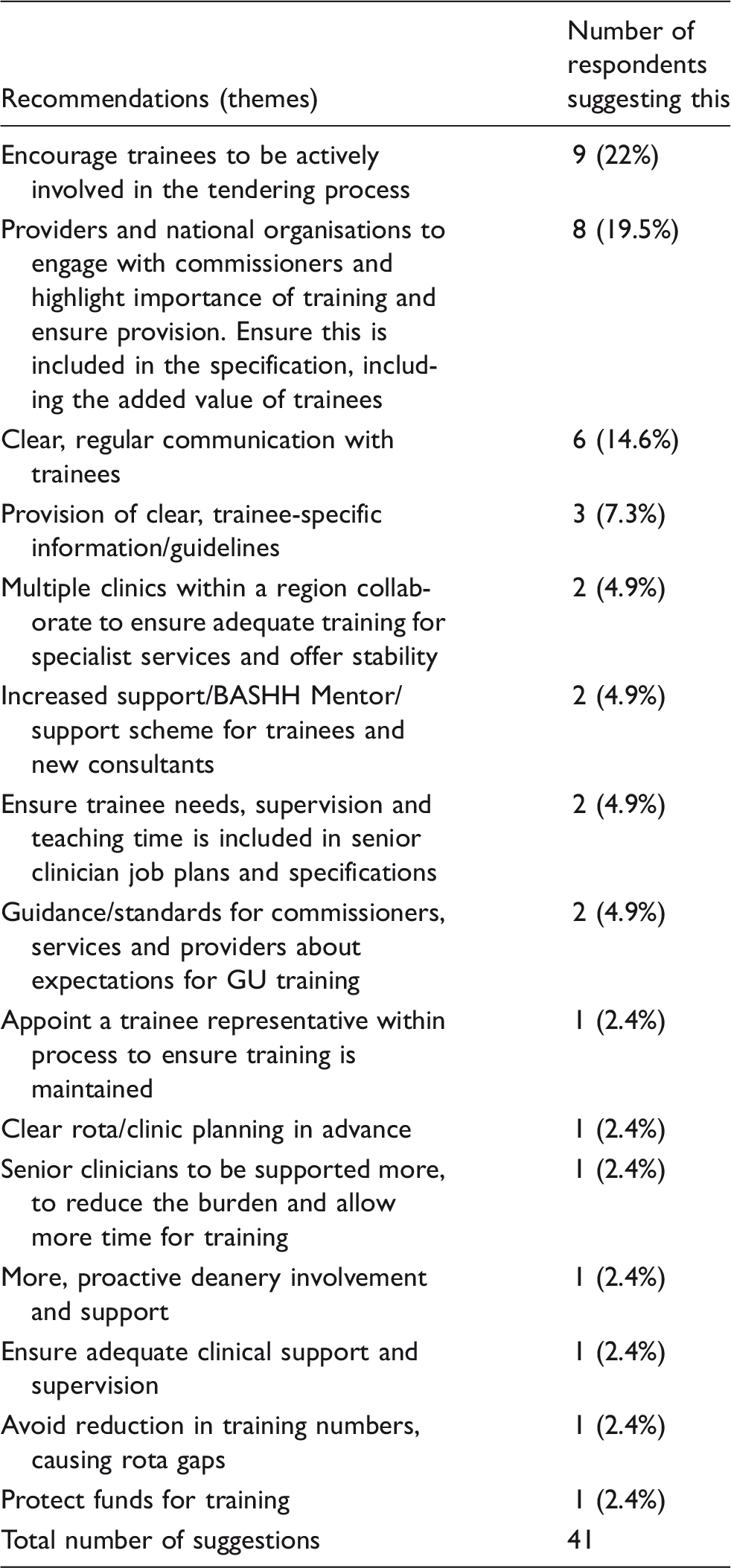
BASHH: British Association for Sexual Health and HIV; GU: genitourinary.
Discussion
Tendering of sexual health services has the potential to create anxiety and increased pressure on staff who work within these services, medical and non-medical. This UK-wide survey demonstrates both positive and negative impacts of tendering on trainees and newly appointed consultants. Most respondents seemed to have an understanding of the tendering process but the majority (77%) also wanted to learn more. A large proportion of survey respondents had experienced or were currently experiencing the tendering process (63%), making this a representative sample of trainees’ experiences.
It is concerning that of respondents who had experienced tendering, only 19.5% felt that their training programme was taken into consideration and 9.76% that their individual training needs were taken into consideration. Less than half of respondents felt adequately supported through the process and only 19% of those who had not experienced tendering anticipated adequate support. However, those who had received support found it useful (median score of 4/5), with most support sought from educational supervisors, colleagues and other trainees.
Importantly, tendering does not appear to have been a wholly negative experience for all trainees with some reporting that it had offered training opportunities. One respondent described taking time out of programme to focus on tendering and writing a successful bid. This proactive, trainee-focused way of dealing with tendering could afford many opportunities to trainees. Unfortunately, only 30% of respondents felt that they were encouraged to get actively involved in the tendering process. To maximise the positive impact of tendering, ensuring trainees are well informed and actively participate in the process is critical, especially as trainees felt that management training was the most likely aspect of their training which had/could be improved post tendering.
A number of negative impacts of the tendering process on training were identified, including morale, stress and anxiety; teaching and training; working environment; clinical supervision and senior support. However, it seems that the anticipation of the negative impact on training may be greater than the actual impact as when asked to rate the impact from −5 to +5 from negative to positive impact, the median score for Group B was −2 where for Group A, who had actually experienced tendering, it was 0.
Some specific concerns raised by a number of trainees included less exposure to specialist services which were not being commissioned by new providers, less teaching time with senior doctors who are pre-occupied with tendering, recruitment and the long-term viability of a career in GUM.
The results of this survey highlight that the impact of the tendering process on trainees varies between locations depending on how this is managed by sexual health staff, deaneries, programme directors and commissioners. However, there are some steps that could be taken to try to minimise any negative impact on trainees. Communication and active involvement is key; trainees should be kept informed of the tendering process and how it is progressing locally. A trainee-focused document about tendering could help trainees feel more informed, alleviate unnecessary anxiety and encourage active involvement. Clinics and commissioners should be encouraged to actively involve trainees in the whole tendering process. This could be an excellent opportunity for trainees to develop key management and leadership skills.
In order for training to be considered within the tendering bid, commissioners need clear guidelines about the GUM training programme, the minimum requirements for adequate training and also the benefit of having trainees within clinics. Including the provision of training within the tendering bid is vital to ensure a high-quality training programme is maintained. This should include support for senior clinicians to enable continued delivery of GUM teaching despite extra pressures of the tender and a clear plan as to how trainees would meet all curriculum requirements within the new service. The provision of unbiased, external sources of support such as BASHH mentors could be beneficial in both supporting trainees through this process and highlighting potential problems and solutions.
Limitations to this survey include difficulties in determining what percentage of eligible trainees and consultants responded to the survey.
A number of consultants (20) responded to the survey; however, it was not clear at what stage these consultants went through the tendering process. Although the email invitation specified ‘consultants who had been through the tendering process as trainees’ the stage of their training was unclear in their responses. This did highlight that the challenges posed to newly appointed consultants who are experiencing tendering at such an early stage of their career and the need for extra support for some individuals.
Conclusion
The tendering process can be a challenging and anxiety-provoking time, but if managed well, the process could offer trainees new educational opportunities and should not impact on GUM training. The process could offer trainees new educational opportunities. This survey highlights that trainees’ views on how the tendering process has affected them vary but overall they report negative experiences. However, we suggest that there are steps that can be made to minimise any detrimental effect on training. We recommend the development of formal guidelines for commissioners and educational supervisors about GUM training requirements that emphasise the importance of support and supervision, ensuring clear information and communication with trainees before and during the process and allowing trainees the opportunity to take a proactive role in the process.
Since 2013, competition and fill rates for GUM specialist training posts have decreased dramatically. In 2015 only 46% (17/37) of available GUM national training posts were filled, 3 compared to 100% (24/24) in 2013. 3 The reasons for these changes are likely to be complex and multifactorial; however, concerns exist that the tendering process, both its effect on training and risk to future job prospects, could be a contributing factor. Further studies looking at this may be informative and help to direct further development of training programmes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.