
Abstract
Summary
Diverse manifestations of ocular syphilis may involve any structure in the eye, at any stage of the disease. Posterior uveitis in the form of posterior placoid chorioretinitis has been described in secondary- and tertiary-acquired syphilis. In this case report, we present a 47-year-old man with late latent syphilitic infection and fundoscopic, as well as angiographic findings consistent with acute syphilitic posterior placoid chorioretinitis. To our knowledge this form of patchy multifocal choroiditis has never been described in the latent stage of the disease.
INTRODUCTION
Acquired syphilis is a sexually transmitted, chronic and systemic infection, caused by the spirochete Treponema pallidum. The disease if left untreated may progress through four stages named primary, secondary, latent and tertiary.
Eye involvement typically occurs during the secondary and tertiary stages, although syphilitic ocular manifestations have been reported at any of the four stages of the disease. 1 The treponemal infection can cause various patterns of inflammation in the anterior chamber, vitreous, retina, choroid and optic nerve, often mimicking other diseases. 2
Posterior uveitis is the most common ocular complication seen in secondary- and tertiary-acquired syphilis. One recognized form of posterior uveitis in syphilis is posterior placoid chorioretinitis. 3
In this article, we present a 47-year-old man with late latent syphilitic infection and lesions consistent with acute syphilitic posterior placoid chorioretinitis (ASPPC) in his angiogram.
CASE REPORT
A 47-year-old man was referred to our clinic with a five-day history of progressive visual loss in his left eye. Prior to this, he had an upper respiratory tract infection and developed some ache in his left eye. Twenty years earlier he had a history of loss of vision in his left eye, with complete recovery after treatment. No further details were available.
On examination, visual acuity was 6/6 in the right eye and hand movements (HM) in the left eye. He had no relative afferent pupillary defect, very quiet anterior chambers and no signs of vitritis bilaterally. Fundoscopy revealed greyish, placoid lesions at the level of the retinal pigment epithelium (RPE) with minimal pigmentation, involving the macular region in the left eye (Figure 1). One or two discrete punctate lesions were also noted in the right eye. There was no evidence of any retinal vasculitis or retinitis bilaterally.
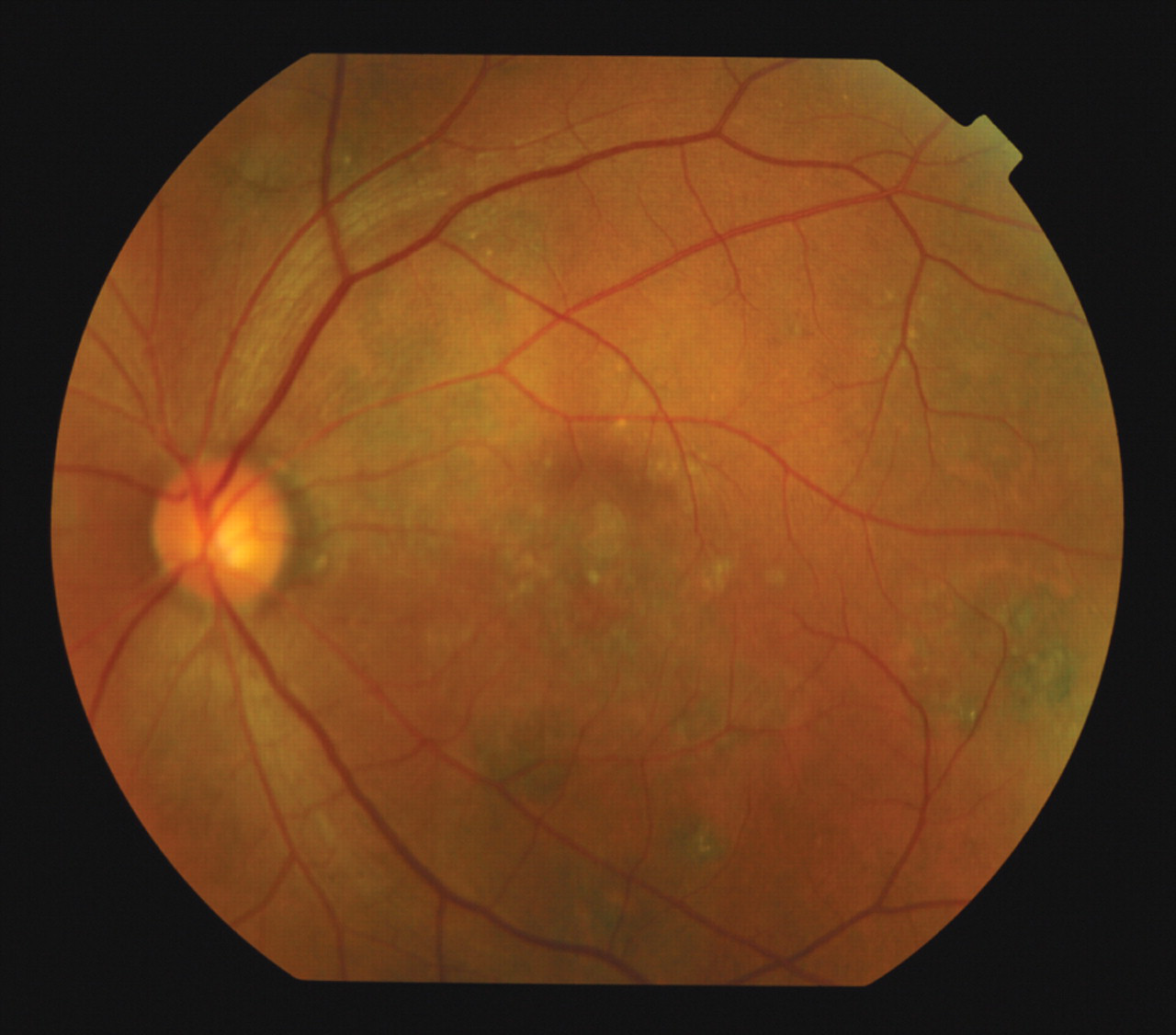
The posterior pole of the left eye
The angiogram showed areas of early hyperfluorescence with no increase in the late frames (window defects). These ‘window defects‘ indicate RPE atrophy. In addition, he had scanty focal areas of hyperfluorescence, which increased through the angiogram, suggesting ‘active hot spots’ of choriocapillaries dye leakage (Figure 2).
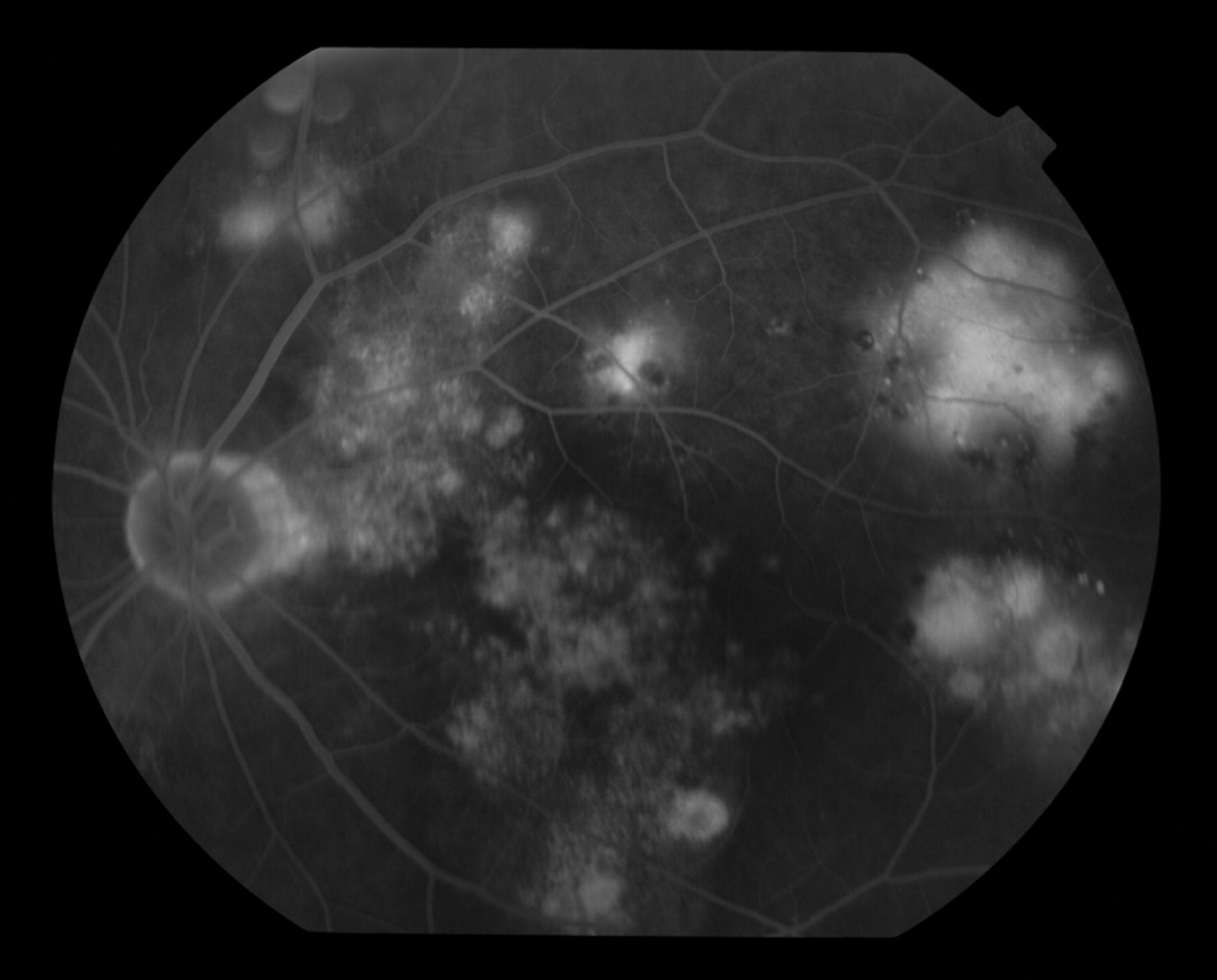
Late phase showing choriocapillaries dye leakage
The patient's treponemal serology was as follows: enzyme immunoassay- and T. pallidum particle agglutination assay-positive, Venereal Disease Research Laboratory (VDRL)-negative. He had a clinical diagnosis of late latent infection, defined as no evidence of primary, secondary, and tertiary syphilis and negative rapid plasma reagin. He reported last sexual intercourse two years earlier. The patient was subsequently treated with daily i.m. procaine penicillin 1.8 MU with oral probenecid 500 mg q.d.s. for 17 days.
Following treatment, the vision in his left eye was unchanged to ‘count fingers’, while his right visual acuity was 6/12 with pin-hole correction. His choroiditis resolved in the left eye, to leave some chorioretinal scarring. A repeat angiogram two months later showed a right sub-foveal serous detachment. As he had already completed antibiotic treatment, this was believed to be inflammatory, and he was given a right orbital triamcinolone injection (40 mg) via a posterior subtenons route.
At follow-up examination three months later, the right visual acuity was 6/9 with pin-hole correction and the left visual acuity was HM, with a preserved field of vision. Fundoscopy revealed extensive chorioretinal atrophy at the macula in the left eye, with presumed photoreceptor loss. His previous right serous sub-foveal detachment had settled.
DISCUSSION
ASPPC has been reported to be associated with large, flat, yellowish or grey placoid lesions with faded centres at the level of the RPE in the macula and juxtapapillary areas. In our patient, fundoscopy showed greyish lesions at the level of the RPE in both posterior poles consistent with active chorioretinitis as described above.
Our patient was clinically and serologically diagnosed with late latent syphilis. Although lumbar puncture was not performed, asymptomatic neurosyphilis was excluded in the differential diagnosis. According to Wöhrl 4 neurosyphilis is unlikely in patients with late latent syphilis and a negative blood VDRL-test.
To our knowledge this form of patchy multifocal choroiditis has never been described in the latent stage of the disease.
This case report shows the diverse manifestations of ocular syphilis and demonstrates that atypical presentations are often encountered. Conventional syphilis staging can be problematic in ocular disease because of the multiple syphilitic ocular manifestations that have been reported in any of the four stages.
Footnotes
ACKNOWLEDGEMENT
The work was carried out at the Ophthalmology Department of Barts and the London NHS Trust.