
Abstract
In 2016, NHS Lothian regional sexual and reproductive health services introduced an electronic pharmacy treatment voucher that could be sent to the mobile phones of patients with Chlamydia trachomatis and their sexual contacts. A retrospective audit of the electronic treatment voucher database was conducted for vouchers issued between April and December 2016. Five hundred and forty-nine vouchers were issued and 56% were redeemed at a pharmacy within one week of issue. This suggests that electronic vouchers are a popular and effective means of providing expedited treatment for uncomplicated C. trachomatis at a community pharmacy.
Introduction
Chlamydia trachomatis is the UK’s most common bacterial sexually transmitted infection. 1 If uncomplicated, it can be treated with 1 g azithromycin as a single dose. Timely treatment is important to help reduce transmission, reinfection from untreated sexual contacts and complications of untreated infection. 2
In 2007, NHS Lothian Sexual Health Services introduced a service, whereby asymptomatic individuals with C. trachomatis could choose to receive a paper treatment voucher (collected in person or via post) that was redeemable for antibiotics at a community pharmacy.2,3 Given its popularity and the increasing use of mobile phone technologies, 4 the service adapted this paper voucher system in April 2016 to send a voucher electronically as a text message to a mobile phone. This could be sent to patients with uncomplicated C. trachomatis or non-specific urethritis (NSU) and sexual contacts. We aimed to evaluate the use of this novel electronic voucher treatment service.
Methods
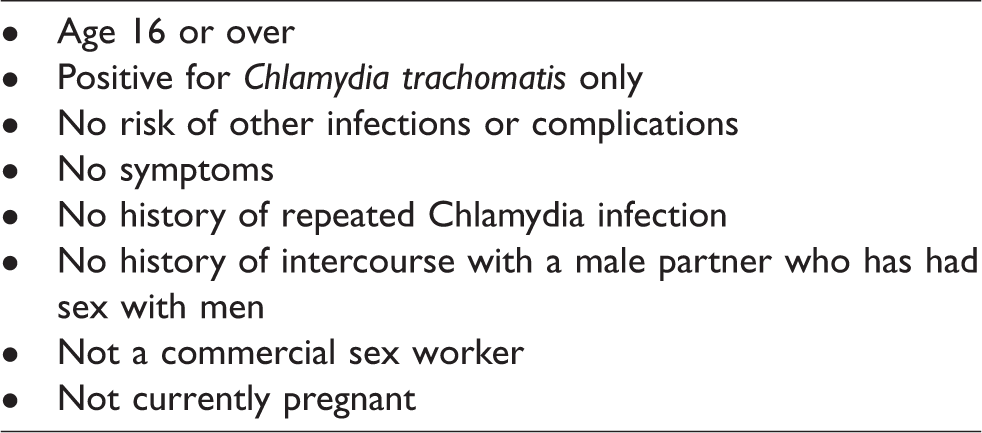
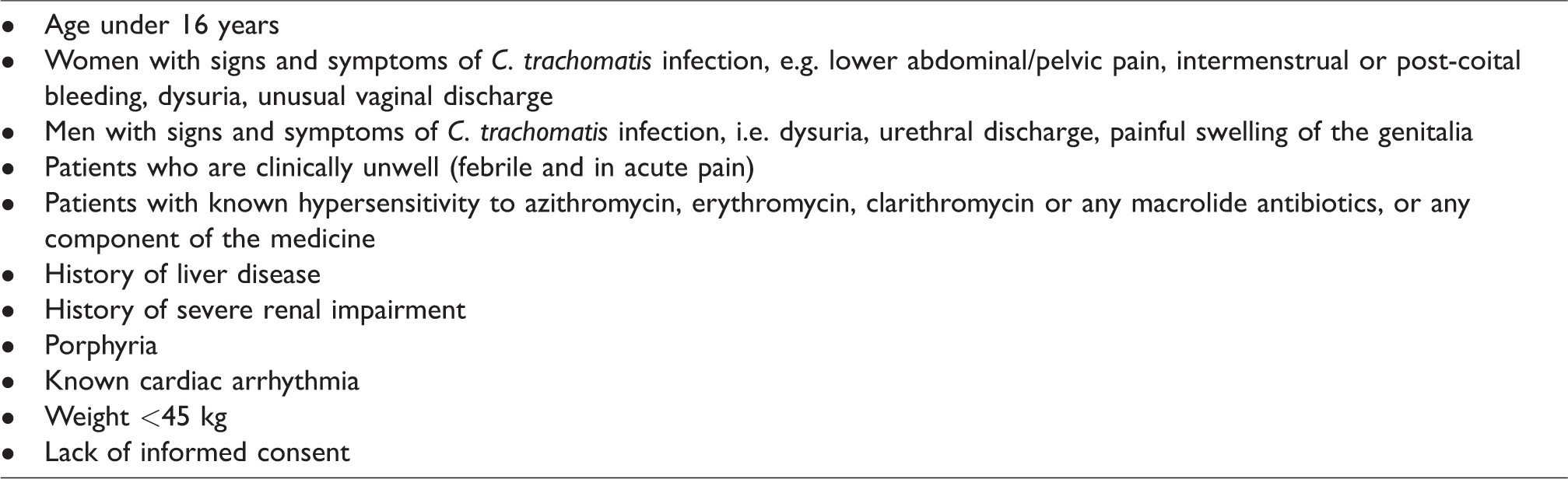
Patients diagnosed with C. trachomatis or NSU (index cases) at NHS Lothian Sexual Health Services were contacted by a health adviser (as per routine) to discuss their choice of available treatment options (Figure 1). Patients were eligible to receive the vouchers to their mobile phone if they fulfilled certain criteria (Table 1). They could also choose to receive vouchers to forward to their current or recent sexual contact(s). Vouchers each had a unique number and had to be presented within seven days at one of the 108 participating community pharmacies or else it was no longer valid for redemption. Pharmacists issued oral azithromycin 1 g at no cost to the individual, via a patient group direction (PGD), i.e. strict criteria to permit provision of specified medicines by non-prescribers (Table 2). 5 Pharmacists then returned a claim form to the Sexual Health Service to be reimbursed for the cost of azithromycin, plus a £5 fee.
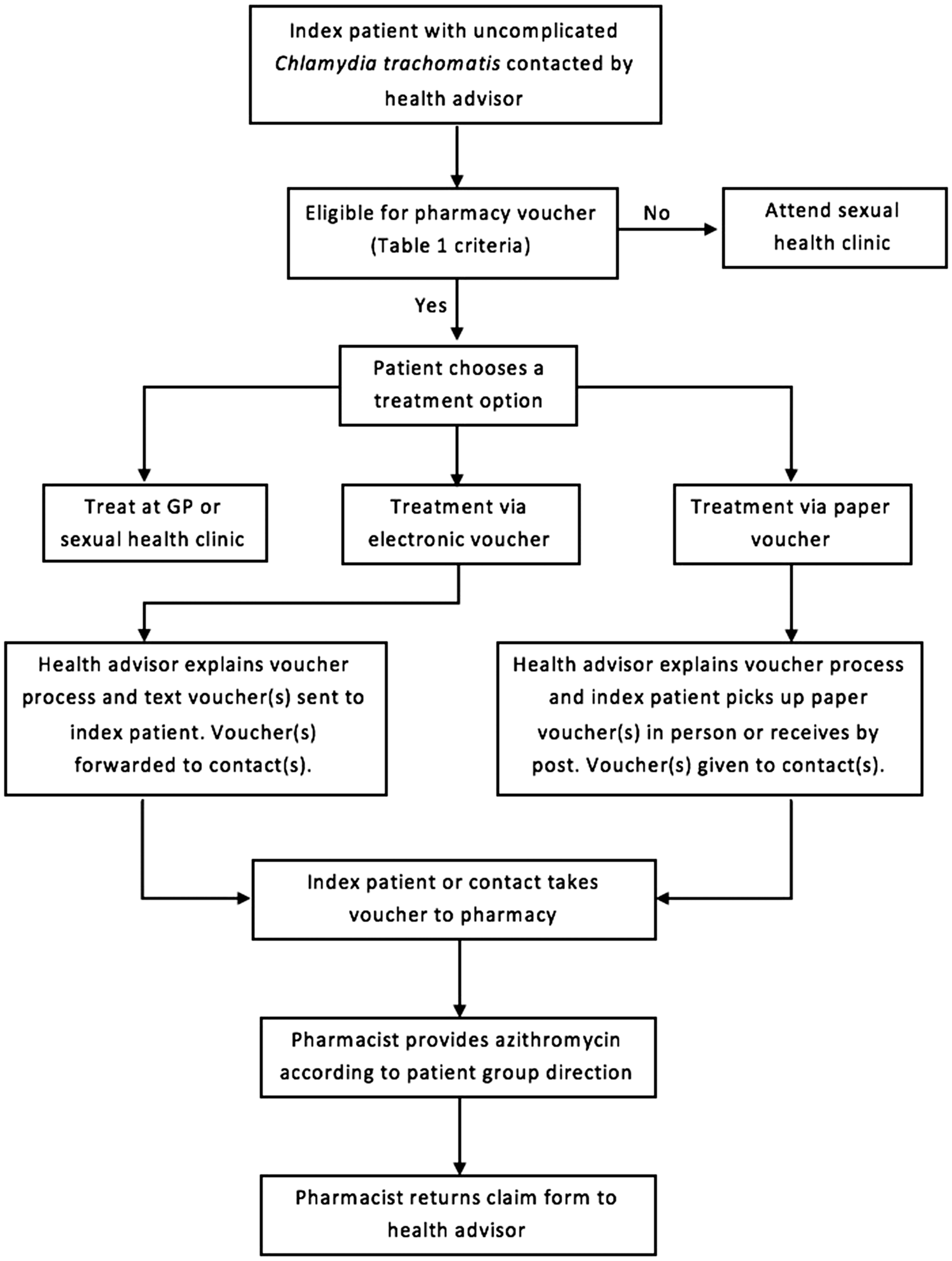
Pathway showing treatment options for index patients and contacts.
Patient eligibility criteria for receiving Chlamydia treatment vouchers.
Patient group direction exclusion criteria. 5
A retrospective audit was conducted of the electronic treatment voucher database to determine the number of electronic vouchers issued (April–December 2016), proportion of vouchers redeemed and characteristics associated with redemption. IBM SPSS Statistics, version 22.0 (IBM Corp., Armonk, NY, USA) was used to perform descriptive statistics and tests of normality, association and trend.
Results
Voucher issue
Between April and December 2016, 1400 of 24,336 samples (5.75%), sent by NHS Lothian Sexual Health Services to the regional laboratory, tested positive for C. trachomatis. A total of 549 electronic vouchers were issued to index patients (n = 381, 27% of total Chlamydia-positive samples) and to contacts (n = 168). Sixty-five per cent of index patients reported no contacts, 34% had one contact and <2% had two or more contacts issued with a voucher.
Demographic characteristics
The median age of individuals was 22 (range: 16–56 years). Two hundred and thirty-seven electronic vouchers were issued to females, 163 to males and 149 to those whose gender was unknown.
Voucher redemption
Three hundred and six out of 549 vouchers (56%) were redeemed at pharmacies (230 were index patients and 76 were contacts). An index patient was significantly more likely to redeem a voucher than a contact (p = 0.001, odds ratio = 1.84, 95% confidence interval: 1.28–2.66). The median number of days from voucher issue to redemption was zero, i.e. less than one day (range: 0–26 days).
There was a significant association between deprivation (measured using the Scottish Index of Multiple Deprivation [SIMD] quintiles) 6 and voucher redemption (p = 0.012). Those in the most deprived category (SIMD 5) were less likely to redeem their vouchers than those in the least deprived category (p = 0.008). No significant differences were found between age or gender and voucher redemption.
Discussion
It is estimated that over the nine-month study period, at least one in four individuals testing positive for Chlamydia received an electronic text voucher and more than half of these were redeemed. This suggests that this is a popular and effective means of providing expedited treatment for uncomplicated C. trachomatis at a community pharmacy. Patients do not need to attend a sexual health clinic or make an appointment with their general practitioner (GP), both of which may be associated with waiting times for an appointment. 7 The advantage of the electronic voucher is that the individual does not need to collect a voucher in person or receive it by post, potentially expediting treatment further. Treatment at a local community pharmacy compared to a sexual health setting may be convenient and less stigmatising, 2 easier to access and provide increased anonymity. 8 If patients are attending pharmacies for treatment, it will release time and resources in sexual health clinics to deal with patients with more complex problems. 3 Additionally, the PGD could easily be modified to reflect any future changes in recommended antibiotic therapy for uncomplicated Chlamydia or NSU.
This is the first study of using electronic treatment vouchers for this purpose. Given its nature as a database review, its findings are limited to the information recorded in the database. Future research should establish patient and pharmacist views on the service and the reasons for vouchers not being redeemed. The service could be expanded to include treatment of patients testing positive for Chlamydia within the GP setting.
Footnotes
Acknowledgements
The authors wish to thank Donna Nisbet for her assistance with accessing the NHS Lothian electronic treatment voucher database. They are also grateful to Katherine McClure for her previous audit of the paper treatment vouchers which assisted with the methodology used for this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.