
Abstract
Partner notification (PN) in the UK is of limited effectiveness. Expedited partner therapy improves PN outcomes but does not comply with existing UK professional guidance. We developed two new strategies, known as accelerated partner therapy (APT), based on elements of PN practice for which there is evidence of efficacy, and which conform to UK prescribing guidance. We explored the acceptability and feasibility of these models qualitatively in genitourinary medicine clinic attenders. Both strategies were viewed favourably. Preference was influenced by age, relationship type, whether participants were delivering or receiving APT and whether the sex partner was aware of the participant's clinic visit. APT provides a new approach to PN, which has strong patient support and complies with existing UK regulations. The complex factors that influence patients' choice of PN method suggest that provision of a range of PN options including APT may be central to improving the effectiveness of PN in the UK.
INTRODUCTION
Current UK methods of partner notification (PN) only reach 40–60% of named sexual partners 1 and re-infection/persistent infection rates are high. 2 In the USA, some states have adopted expedited partner therapy (EPT) 3 in which sex partners of people with curable sexually transmitted infections (STIs) are treated without the need for medical evaluation. 4 This usually entails giving the index antibiotics or a prescription to give to their sex partner, a practice known as patient delivered partner therapy. A systematic review of PN strategies 5 concluded that EPT improves PN outcomes. However, the differences in professional and statutory prescribing guidance between the USA and the UK currently prevent adoption of EPT approaches in an unmodified form into routine UK practice, although some UK specialists and patients support its use. 6–8
The UK National Institute for Health & Clinical Excellence highlights the need for research into development of new strategies for delivering PN more effectively appropriate to the UK setting. 9 Working within current UK prescribing guidance 10 and incorporating those elements of PN for which there is evidence of efficacy in published studies, 5,11,12 we developed two novel rapid partner treatment strategies that we refer to as accelerated partner therapy (APT). The aim of this study was to explore the factors that influence genitourinary (GU) medicine attenders' choice of PN method and their opinions of our APT models using a qualitative approach, in order to further develop maximally effective and acceptable versions of APT for further research in a clinical trial.
METHODS
The APT models are shown in Figure 1.
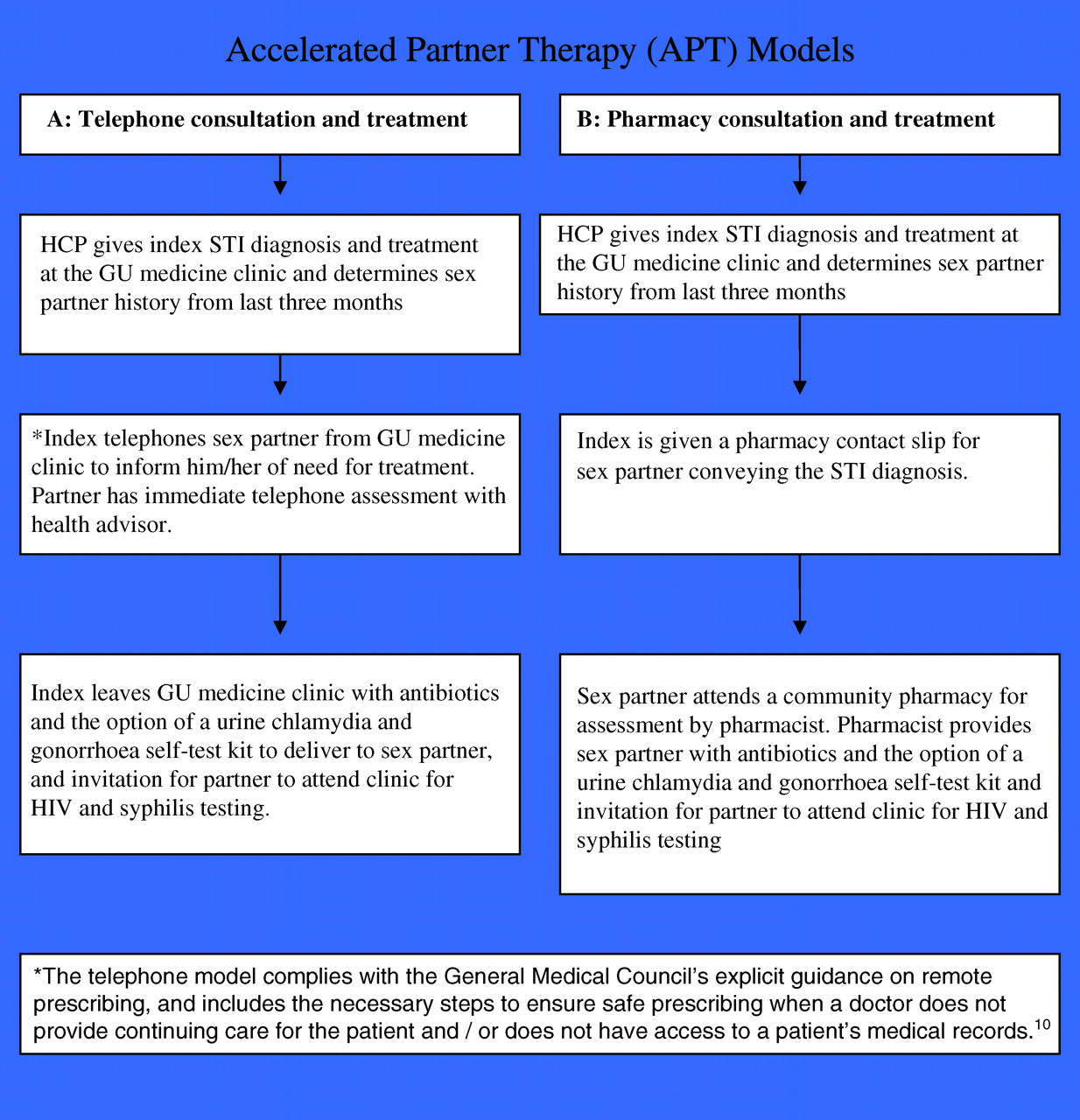
Accelerated partner therapy models. HCP = health-care professional; STI = sexually transmitted infection; GU = genitourinary
We developed a topic guide to use in semistructured interviews with GU medicine clinic attenders to explore: the acceptability and feasibility of our novel APT models; factors that influence choice of PN method; how and when people communicate with their sex partners about their clinic attendance; treatment without clinic attendance; and feelings about receiving and delivering APT.
We undertook the study in Patrick Clements Clinic, Central Middlesex Hospital, an outer London GU medicine clinic with ethnically diverse attenders who have high rates of STIs, during November 2004. Our sampling frame included patients aged over 16 years representing a range of demographic variables and risk profiles, who were diagnosed with an acute STI or who were contacts of people with acute STIs. The researcher (LS) approached all eligible patients, and obtained informed written consent from those who wished to participate. LS undertook 25–30-minute, audiotaped, face-to-face interviews in a quiet consulting room during the clinic visit. Tapes were labelled with an identity number to protect confidentiality and transcribed verbatim.
Analysis
We analysed the data using the ‘Framework’ approach. 13 Recurring themes and concepts were identified to make up a thematic framework, which we then applied systematically to the transcripts. LS and JLC undertook analysis, and reliability was enhanced by double coding a subset of transcripts and comparing inter-rater reliability.
Ethical approval was obtained from Brent Medical Ethics Committee (04/Q0408/41).
RESULTS
Forty eligible patients were approached: two declined due to insufficient time, and one interview was unintelligible on transcribing.
Ten participants were aged 16–24 years (four men, six women); 15 aged 25–30 (six men, nine women) and 12 were over 30 (six men, six women). The participants were ethnically diverse: eight white British, six white non-British, five black British and the remainder a mix of ethnicities reflecting the clinic attending population. Thirty-five described themselves as heterosexual (14 men, 21 women) and two were men who have sex with men (MSM).
Three main themes emerged.
Views on PN and communication with sex partners around the time of clinic attendance
All participants understood how STIs are transmitted and recognized the importance of treating sex partners.
The type of relationship (current/primary partner/casual/ex partner) was an important influence on whether the participants had told their partners that they were attending clinic for STI tests. The majority stated that their primary sex partners were aware and participants intended to inform them of the outcome of their attendance after they left the clinic. Participants whose partners were unaware of their clinic attendance (more common among participants with ex, new or casual partners) only intended to tell their partners if an STI was diagnosed.
‘I'll tell him [new partner] depending on the results. I haven't told him I'm at the clinic because he will think I don't trust him’. (F, 24 years)
Feelings about the different APT options and urine self-testing kits
APT Option A
Most participants liked the convenience of taking tablets home with them for their partner and valued the telephone consultation with a health-care professional as it would save their partner time by avoiding a clinic attendance while providing a way of obtaining advice and reassurance.
‘Good idea…..and if you've got the same thing what's the point of them coming in and getting treated – you might as well just do two in one go’. (F, 21 years)
APT Option B
This was acceptable to most participants especially those whose partners were unaware of their clinic attendance. As such, participants thought that pharmacy treatment was more feasible than telephoning their partners from the clinic and they liked the fact that they would be able to discuss the diagnosis with their partner(s) in person before needing to arrange partner treatment. This option was also preferred for ex-partners (a partner with whom the index did not anticipate future sex) as participants felt that giving a pharmacy contact slip to an ex-partner would be easier and less embarrassing.
‘If I knew the person well I would prefer the tablets there and then. If it was a one night stand and I still had the person's contact, then a prescription [pharmacy contact slip]’. (M, 43 years) ‘It would be easier and less embarrassing than having to come in [to clinic] with her [participant's current partner] as you know it's going to cause arguments’. (M, 44 years)
Participants voiced mixed feelings about provision of the urine self-test kit in the treatment packs. Some thought that it brought the issue of infection ‘closer to home’.
Some also perceived that it would be a way for their partners to get tested and treated without the stigma and embarrassment of coming to the GU medicine clinic.
‘With tablets kinda you can skirt around the issue, but if you've got test kits, it's in your face, it's real’. (F, 33 years)
Preference for the different APT options when delivering and receiving APT
Preference seemed to be influenced more by the age of the participant, relationship type and whether or not their partner knew they were attending a GU medicine clinic, rather than by gender or ethnicity of the participant.
If delivering APT, the majority of participants would choose APT Option A. Younger participants (16–24 years) supported the inclusion of a self-test kit for their partners but this was less important to the older participants who particularly valued the convenience and speed of this approach. This was particularly noticeable in those participants who had attended a GU medicine clinic before.
However, if receiving APT from a partner the younger participants' preference was equally split between APT Option A and attending clinic in person. Of note, we did not present clinic attendance as an option and participants raised this without prompting. Two factors emerged as important influences: the desire for face-to-face advice and reassurance from a health professional at the GU medicine clinic; and reservations about receiving tablets from their partners, which suggests that trust may be an issue when deciding on options within the younger age group. The older participants found it acceptable to receive APT Option A.
‘I wouldn't take the tablets if they were brought to me. I would want to come to clinic and get proper tests, and go through proper procedures’. (M, 18 years) ‘Nah, I wouldn't like it, I wouldn't take the tablets before finding out what they were especially off casual partners, they might be anything. I would have to believe them and see that she had discharge or something, innit’. (M, 22 years)
APT in the forms described does not include a requirement for HIV, syphilis or hepatitis testing to be offered at the time of antibiotic treatment. However, our models do include a recommendation for the partner to attend clinic at a later stage to undertake these tests. The majority of participants perceived that they would take up this offer, mainly for the opportunity to seek reassurance about their health.
DISCUSSION
Participants found APT as acceptable and feasible approaches to PN. Elements that were particularly appealing included: telephone assessment of sex partners enabling them to take away antibiotics from clinic to give to their sex partners (assuming their partner was aware of their clinic attendance); pharmacy-based assessment and treatment (assuming pharmacist had specialist sexual health knowledge and a private consultation area); and for some participants, the ability for sex partners to have a test for chlamydia and gonorrhoea without the need for clinic attendance. Participants also perceived that they would want to attend clinic for HIV and other blood-borne infection testing after they had received their antibiotics.
Many factors influenced preference for PN method including: age; relationship type; issues of trust; whether participants were delivering or receiving APT; whether the sex partner was aware that the participant was attending clinic; and the need to balance the desire for face-to-face reassurance from a specialist sexual health-care professional with difficulties in accessing clinic; and perceptions about what their partner would prefer.
Patient referral is the most common and preferred method of PN for curable STIs in the UK 5,6,14 but in most sexual health care settings it fails to reach half of exposed sexual partners requiring treatment. 1,3 Primary health-care providers are already undertaking elements of EPT in their current practice. 15 Despite this, novel PN strategies have not been extensively evaluated in the UK.
This is the first UK study to explore patients' views of novel rapid PN strategies that are consistent with current UK prescribing guidance. The qualitative approach provides deeper understanding of the complex factors that guide patient acceptability and choice of PN method. The range of views from a diverse sample of clinic attenders on the various APT models proposed here have important implications for the feasibility and development of new models of PN in this context.
Our findings are biased in favour of those who perceive fewer barriers to attending sexual health services than those who choose to access sexual health care elsewhere and this may have impacted on preference for the different APT options, high perceived uptake of HIV testing at a later stage and desire by some participants to have their partners attend clinic for testing and treatment in preference to either APT option. We acknowledge that MSM were under-represented in our sample. However, MSM have more complex PN needs and would require an adapted interview.
These APT models offer the opportunity for widening access to rapid treatment of sex partners of people with curable STIs within existing UK prescribing guidance and in ways that are acceptable to patients. GU medicine clinic attenders want a choice of PN options, which may or may not include clinic attendance, depending on complex factors relating to age, partnership type and issues of trust. This finding is particularly important for the design of future trials and evaluations of new PN strategies as the effectiveness of different PN strategies may be greatly influenced by participants' ability to choose the strategy, which best suits their needs and this may vary for different sexual partners.
It will be important to determine the acceptability of APT in those who choose to access care in community services as there may be differences in APT preference and willingness to attend for subsequent HIV and syphilis testing. Newer HIV testing technologies based on oral fluid may enable pharmacy-based testing in the future and provision of APT via this route could then include an offer of an HIV test at the time of treatment. Similarly, MSM's views of APT require further investigation as PN in this group presents particular challenges. We are currently conducting an exploratory trial of APT in two hospital sexual health services in order to further explore the feasibility of implementation and to inform future trials of clinical efficacy. 16
Footnotes
ACKNOWLEDGEMENTS
We are grateful to patients at Patrick Clements Clinic for participating in this study and the staff for helping with recruitment. The financial support for this study was received from the Medical Research Council: APT study: Can Accelerated Partner Therapy (APT) improve outcomes of partners? UKCRN ID 2564. National Institute for Health Research.