
Abstract
Immune reconstitution inflammatory syndrome (IRIS) in HIV-infected patients after initiating antiretroviral therapy usually involves worsening manifestations of overt infectious disease. Here, we describe a sporadic case of a late-diagnosed HIV-positive man who developed Graves’ disease as the first noninfectious IRIS followed by immune thrombocytopenic purpura as the second noninfectious IRIS.
Introduction
Immune reconstitution inflammatory syndrome (IRIS) after initiating antiretroviral therapy (ART) usually occurs as a worsening of manifestations of opportunistic infections. 1 Reportedly, less frequently, IRIS involves autoimmune diseases, including vasculitis, rheumatic diseases, and thyroid diseases. 2 The sequential occurrence of two autoimmune diseases in a single patient is highly unlikely. Here, we report an interesting case of a patient who developed Graves’ disease as the first IRIS followed by immune thrombocytopenic purpura (ITP) as the second IRIS 5 years later with previously normal thyroid function and platelet count.
Case report
A 66-year-old Japanese man was diagnosed with Pneumocystis pneumonia with HIV infection in June 2006. His CD4 cell count was 2 cells/μL and HIV RNA was 80,000 copies/mL. After treating his pneumonia, ART was initiated with a regimen of tenofovir disoproxil fumarate, emtricitabine and efavirenz (Figure 1). His thyroid function test and platelet count were normal. HIV RNA became undetectable in September 2006 and he had no history of Graves’ disease and ITP.

Changes in the CD4 cell count, HIV RNA, and total cholesterol value from the start of ART to the onset of IRIS. HIV RNA became undetectable in September 2006. CD4 cell count gradually increased to 429 cells/μL in December 2008.
In December 2008, his CD4 cell count gradually increased to 429 cells/μL. Around that time, he experienced weight loss, palpitations, and dyspnea after exercise. His anti-thyroid-stimulating hormone receptor antibodies were 73.7 IU/L. He was diagnosed with Graves’ disease and compound thiamazole was administered; ART was continued. The diagnosis of IRIS was likely for Graves’ disease. His thyroid function became normal in April 2009. However, in February 2010, he noticed exophthalmos and was diagnosed with thyroid-associated ophthalmopathy. He received corticosteroid pulse therapy, followed by corticosteroid maintenance therapy until October 2010 and ART was continued.
In October 2012, his platelet count was 67 × 103/μL (Figure 2). Bone marrow aspiration revealed a normocellular marrow with an increased number of immature megakaryocytes and normal granulocytic differentiation. No morphological abnormality or fibrosis were identified. These findings were compatible with ITP. Together with other blood cell findings, the possibility of myelodysplastic syndrome was unlikely. Urea breath tests for the detection of Helicobacter pylori infection were negative. After that, his platelet count gradually decreased. In January 2014, corticosteroid therapy was initiated with 0.5 mg/kg prednisolone. However, his platelet count decreased to 3 × 103/μL and nose bleeds occurred, and he required platelet transfusion; his ART was continued. Three months later, romiplostim was added, which stabilized his platelet levels. The diagnosis of IRIS causing ITP was likely.
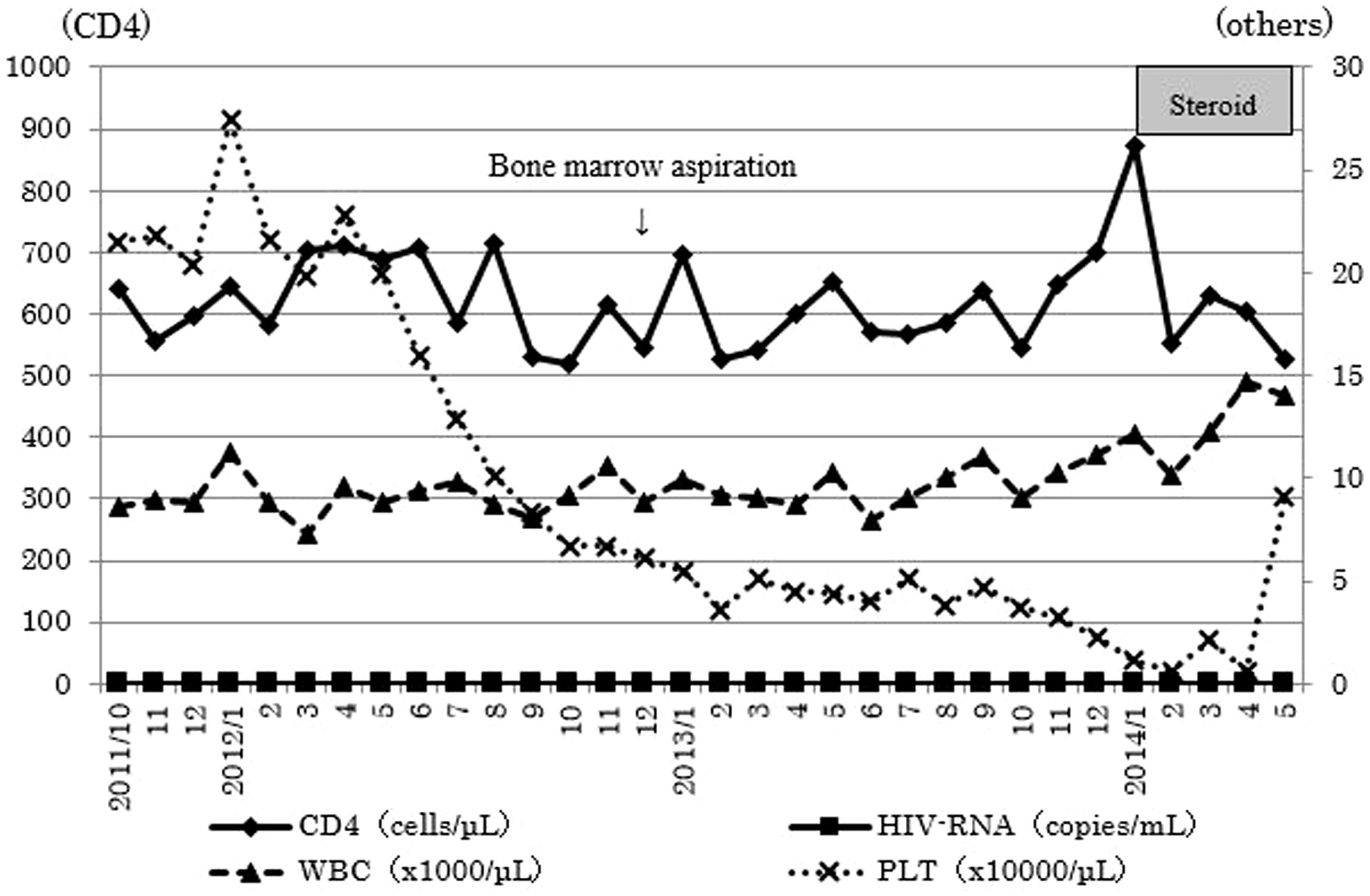
Changes in the CD4 cell count, HIV RNA, white blood cell count, and platelet count from 1 year before ITP onset to platelet count recovery after steroid therapy. Platelet count was 67 × 103/μL in October 2012. Corticosteroid therapy was initiated in January 2014.
In May 2014, compound thiamazole was discontinued, but once a week, romiplostim was injected and 10 mg prednisolone was continued as maintenance therapy. Currently, his condition is stable.
Discussion
IRIS usually develops within a few months for opportunistic infections, which sometimes includes Graves’ disease that develops 14–53 months after the introduction of ART.3,4 In our case, Graves’ disease occurred 30 months after the initiation of ART. Therefore, the timeline for Graves’ occurring does fit with an IRIS picture. However, since Graves’ disease is common, it could have been a sporadic occurrence.
In October 2012, our patient’s platelet count decreased 46 months after the diagnosis of Graves’ disease, which stable at that point. Corticosteroid therapy for Graves’ disease was discontinued in October 2010. Although thrombocytopenia is a common finding in patients with HIV, with an incidence of 30%, ITP is rare.2,5–8 ITP presenting as IRIS has only been described in three previous case reports.6,9,10 In our case, ITP occurred six years after initiation of antiretrovirals and six years of virological suppression. Therefore, we cannot draw firm conclusions that withdrawal of steroids definitely led to ITP emergence.
To the best of our knowledge, this is the first case with both Graves’ disease and ITP potentially presenting as IRIS in an HIV-infected patient. 9 The risk for IRIS is associated with CD4 cell count at the initiation of ART. Patients with CD4 cell count < 50 cells/μL have a higher risk of developing IRIS. 1 In our case, the CD4 cell count was 2 cells/μL when ART was initiated. In addition, this case demonstrated a high degree of increase in the CD4 cell count; this could be a possible reason for the occurrence of two IRIS events in a single patient.
Since the second IRIS occurred more than 6 years after the initiation of ART, physicians caring for HIV-infected patients should be aware that more than one IRIS can emerge in a patient. Based on our clinical experience, we recommend the continuation of ART with initiation of corticosteroids for the management of IRIS.
Research ethics and patient consent
The patient was not identified in this case report for reasons of confidentiality; therefore, this study was formally exempted from Kochi Medical School Institutional Review Board’s approval. A written informed consent for patient information to be published was provided by the patient.
Footnotes
Authors’ contribution
Miho Nakamura and Masafumi Okazaki wrote the paper. Tadashi Asagiri and Akiko Imai analyzed the data and critically reviewed the case. Seisho Takeuchi edited the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.