
Abstract
Cervical cancer is the third leading cause of cancer-related death and the second most diagnosed cancer among women in developing countries. We determined the prevalence of abnormal Papanicolaou (Pap), high-risk HPV (hrHPV), and colposcopy among transactional female sex workers (FSWs) in La Romana, Dominican Republic. The results of 144 FSWs of ages 18–54 years who completed a demographic interview and Pap testing with hrHPV detection between June 2015 and April 2016 were analyzed. Women with abnormal results were referred for colposcopy. Risk factors for abnormal Pap were assessed through bivariate and multivariate analyses. Overall, 36.1% (52/144) of Paps were abnormal and 43.4% (62/143) had hrHPV. Of all women with hrHPV and/or abnormal Pap (68/144; 47.2%), 61 (89.7%) were referred and 16 (26.2) underwent colposcopy. HPV16 and/or 18/45 was detected in 33.3% (15/45) of low-grade Paps. Binge drinking, weekly (AOR 5.1, 95% CI: 1.8–14.5) or daily (AOR 4.9, 95% CI: 1.5–16.6), and age at first sexual relation (AOR 1.2, 95% CI: 1.0–1.5) were significantly associated (p < 0.05) with abnormal Pap. Although almost half of participants had abnormal Pap or hrHPV, few underwent colposcopy. Improving access to cervical cancer screening and follow-up for FSWs is imperative.
Introduction
Cervical cancer is the third leading cause of cancer-related death and the second most diagnosed cancer among women in developing countries, where approximately 80% of cervical cancer deaths occur.1,2 In the Dominican Republic (DR), cervical cancer is the most common cancer among women of ages 15–44 3 and an estimated 1507 cervical cancer diagnoses and 600 related deaths occur annually. 4 Risk factors for cervical cancer are early sexual debut, multiple concurrent sexual partners, and lifetime number of sexual partners. 5 Factors contributing to the disproportionate cancer burden in developing countries may include a lack of effective cytology-based screening programs that emphasize patient education, diagnostic treatment centers, and established national vaccination programs to prevent human papillomavirus (HPV). 6
HPV is the most common sexually transmitted infection (STI) worldwide.7,8 Persistent infection with high-risk HPV (hrHPV) subtypes can lead to cervical dysplasia and cancer. Globally, HPV subtypes 16 and 18 account for approximately 66% of cervical cancers. 9 The worldwide prevalence of HPV is 11–12% among women without cervical abnormalities, highest among younger women. 10 The Caribbean has the greatest estimated prevalence of HPV globally, affecting 35.4% of women. 10 In the DR, the prevalence of HPV 16 and/or 18 among women in the general population with low-grade cervical changes is approximately 7.6%. 11
Papanicolaou (Pap) testing is essential for early detection and treatment of pre-cancerous changes and has led to a decline in cervical cancer mortality since its consistent implementation in developed settings; 12 however, this trend is absent in developing countries lacking routine screening. 13 DR’s most recent national guidelines from 2007 recommend Pap testing every one to three years for high-risk groups including women of ages 35–64 and those who report multiple sexual partners and/or early sexual debut. 14 Clínica de Familia La Romana (CFLR) providers, where this study takes place, recommend annual Pap at sexual debut. A national survey in the DR from 2013 indicated 68% of women of ages 15–49 had ever had a Pap and 39% reported testing within the last year. 3 There is no corresponding data for transactional female sex workers (FSWs). FSWs are at greater risk of acquiring HPV and progressing to cervical cancer than women in the general population. 15 To our knowledge, no studies on the rates of HPV or cervical cancer among FSWs in the Caribbean exist. Thus, this study sought to determine the prevalence of abnormal Pap results, hrHPV, and treatment follow-up among FSWs in La Romana (LR), DR.
Methods
Design and setting
This research was conducted at CFLR in LR, the third largest city in the DR. Our study was part of an ongoing study, Risk Factors for Infections in DR in Key Populations, which aims to document the rates and risk factors of STI among five key populations in LR and Santo Domingo: FSWs, pregnant adolescents, people living with HIV, men who have sex with men, and residents of bateyes (communities of majority Haitian sugarcane workers). CFLR offers general services and STI prevention counseling, testing, and treatment; providers recommend FSWs have monthly clinical visits, quarterly government-mandated HIV and syphilis testing, and annual Pap. In 2016, of approximately 20,000 clinic visits at CFLR, 1586 were to the FSWs’ program. This study was approved by the Columbia University Medical Center Institutional Review Board, the Ethics Committee at the Instituto Dermatológico de Cirugía y Piel Huberto Bogaert Diaz, and the Dominican Bioethics Committee, Consejo Nacional de Bioética en Salud, prior to data collection.
Study population and recruitment
The FSW industry in the DR involves about 60,000 to 100,000 women. 16 Data collection occurred between June 2015 and April 2016. Initially, LR was mapped by venue and establishment type such as beer centers, bars or cabarets, restaurants, brothels, night clubs, and street-based sites where FSWs worked independently. 17 The total number of FSWs working in LR was estimated (N = 779). The number of FSWs to be recruited from each establishment type was calculated using the estimated number of FSWs per establishment type and the target sample size (N = 200). Thirty mapped venues were randomly selected for inclusion from which women of ages 18–60 years who self-identified as sex workers and had exchanged sexual services for payment or gifts within the last six months were eligible to participate. The number of participants per venue was variable, ranging from 5 to 48 women. CFLR staff recruited until the target sample size was reached. All study procedures (written informed consent, structured interview, sample collection) occurred at CFLR during the initial enrollment visit.
Data collection
Structured interviews covered sociodemographics, behaviors (health, sexual, transactional sexual, drug use), STI/HIV knowledge, symptoms, and history, and mental health. Cervical samples were collected from enrolled FSWs using a cytobrush and liquid-based cytology regardless of age. Samples were sent to BioReference Laboratories in New Jersey, United States for Pap and hrHPV co-testing. The Aptima HPV test detected the following hrHPV subtypes by transcription-mediated amplification (TMA): 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68. HPV16 and HPV18/45 were specifically reported when present, while the presence of hrHPV types other than 16 and 18/45 was noted, without indicating the specific type. Paps were screened by a cytotechnologist using the CYTYC ThinPrep(TM) Imaging System. Gen-Probe Aptima assay for Chlamydia trachomatis and Neisseria gonorrhoeae and Endpoint PCR technology for Mycoplasma genitalium, Trichomonas vaginalis, and Ureaplasma urealyticum was used.
Participant management
Study team members provided STI risk reduction counseling at enrollment and follow-up appointments (one or two depending on colposcopy referral). FSWs with symptoms consistent with STI infection were treated. After the enrollment visit, CFLR FSW program staff contacted participants via phone and in-person to remind them of follow-up appointments where results and referrals would be shared. Women positive for hrHPV and/or abnormal Pap were referred to the clinic’s gynecologist for colposcopy, regardless of age. Follow-up with colposcopy for women of all ages with abnormal Pap is standard practice at CFLR; this was reflected in the research protocol. All services, including transportation to and from study visits, were compensated.
Measures
The dependent variable was Pap result (normal/abnormal). Abnormal Pap results included: (1) atypical glandular cells (AGC), (2) atypical squamous cells of unknown significance (ASCUS) with positive hrHPV testing, (3) atypical cells of unknown significance, cannot exclude high-grade intraepithelial lesion (ASCH), (4) low-grade intraepithelial lesion (LSIL), and (5) high-grade intraepithelial lesion (HSIL).
Independent variables for the present analysis include sociodemographics and behaviors (health, sexual, transactional sexual, drug use).
Statistical analyses
Our analysis consists of data from 144 participants who completed interviews and Pap testing. Statistical analyses were performed using STATA (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP). Descriptive statistics summarized the analytic sample. Means and standard deviations characterized continuous variables. Frequencies characterized categorical variables. For bivariate analyses, potential significant associations between dependent variable and independent variables were tested using two-sample t-tests or Wilcoxon–Mann–Whitney tests for continuous variables and Chi-square or Fisher’s exact tests for categorical variables. Independent variables (p < 0.1) in bivariate analysis were included in binary logistic regression models to calculate crude and adjusted odds ratios and confidence intervals. 18 Variables were added to the model in a forward selection step-wise fashion to assess their associations with the dependent variable and in the presence of other variables. A final model was selected based on its strength with or without certain variables and was evaluated with likelihood-ratio testing. A variable was considered significant in multivariate analysis at a significance level of p < 0.05.
Results
Sociodemographics
The mean age of FSWs was 27.3 years (Table 1). Most were single (83.3%), born in the DR (97.2%), and had a high school education or above (68%). Their primary source of income was work, including, but not limited to transactional sex where irregular, temporary, or seasonal work (49.3%) was slightly more predominant than regular, fixed work (41.0%). The majority (62.4%) earned the equivalent of US$122–407 per month as of March 2018.
Sociodemographic characteristics, health, sexual, and drug use behavior, and cervical STI results of FSWs in La Romana.

aSection headings from the qualitative interview appear in bold.
bAs of March 2018, one Dominican peso equated to $0.02 US dollars.
cResponse total that does not sum to 144 has missing values.
dThere were 95 responses total; one large outlier was excluded.
eOther gift was defined as services, goods, food, drugs, or rent.
Papanicolaou
Over 70% of women reported a history of Pap testing, of whom 54.1% had testing over a year ago (Table 1). Of all Paps, 36.1% (52/144) were abnormal, divided between LSIL (27/52; 51.9%) and ASCUS (22/52; 42.3%). The remaining 5.8% (3/52) corresponded to single cases of ASCH, HSIL and AGC. Cervical cancer was not detected.
High-risk HPV
High-risk HPV DNA was detected in 43.4% (62/143) of women. One sample had insufficient quantity for hrHPV testing. Over 90% (46/51) of FSWs with abnormal Pap tested positive for hrHPV, half of whom were younger than 24 years old. When stratified by age, the frequency of hrHPV decreased with increasing age. Positive hrHPV results were subtyped as 16 and/or 18/45 (22/62; 35.5%). HPV18/45 (17/62; 27.4%) was more common than HPV16 (7/62; 11.3%). Two women (2/62; 3.2%) were positive for HPV16 and HPV18/45; their Pap results were ASCUS and HSIL. Among FSWs with HPV16 and/or 18/45, 72.3% (16/22) had abnormal Pap results: LSIL (10/22; 45.5%), ASCUS (5/22; 22.7%), and HSIL (1/22; 4.5%). A third (15/45; 33.3%) of women with low-grade cervical changes were positive for HPV16 and/or HPV18/45.
Colposcopy
Under a quarter (16/61; 26.2%) of the women referred to the clinic’s gynecologist underwent colposcopy. Cervical squamous intraepithelial neoplasia 1 (CIN1) was reported in 43.8% (7/16) of women. The remaining 56.2% (9/16) demonstrated cervicitis or squamous dysplasia within normal limits. No cases of cervical squamous intraepithelial neoplasia 2 or 3 were identified.
Bivariate analyses
FSWs with abnormal Pap (Table 2) were younger than those with negative results (p = 0.027) and had earlier sexual debuts (p = 0.067). Women with abnormal Pap had slightly more mixed responses to ease of access to condoms, whereas FSWs with negative Pap almost all indicated that condoms were easy to access (p = 0.134). Binge drinking (≥6 drinks per day) occurred more frequently in FSWs with abnormal Pap (p = 0.017). Drinking before sex was common among both groups (p = 0.539); however, drug use before sex occurred more frequently in those with normal Pap (p = 0.153), although responses were few. Inconsistent condom use was higher among FSWs who reported binge drinking at least monthly (26/46; 56.5%) compared to FSWs who did not (20/46; 43.6%; p = 0.017). Infection with hrHPV (p < 0.001) and/or U. urealyticum (p = 0.052) was more prevalent among FSWs with abnormal Pap. Frequency of doctor’s visits within the last year, condom use, and number of sexual partners within the last six months were not significantly different.
Bivariate analyses between Pap results, sociodemographic characteristics, health, sexual, and drug use behavior, and cervical STI results of FSWs in La Romana.
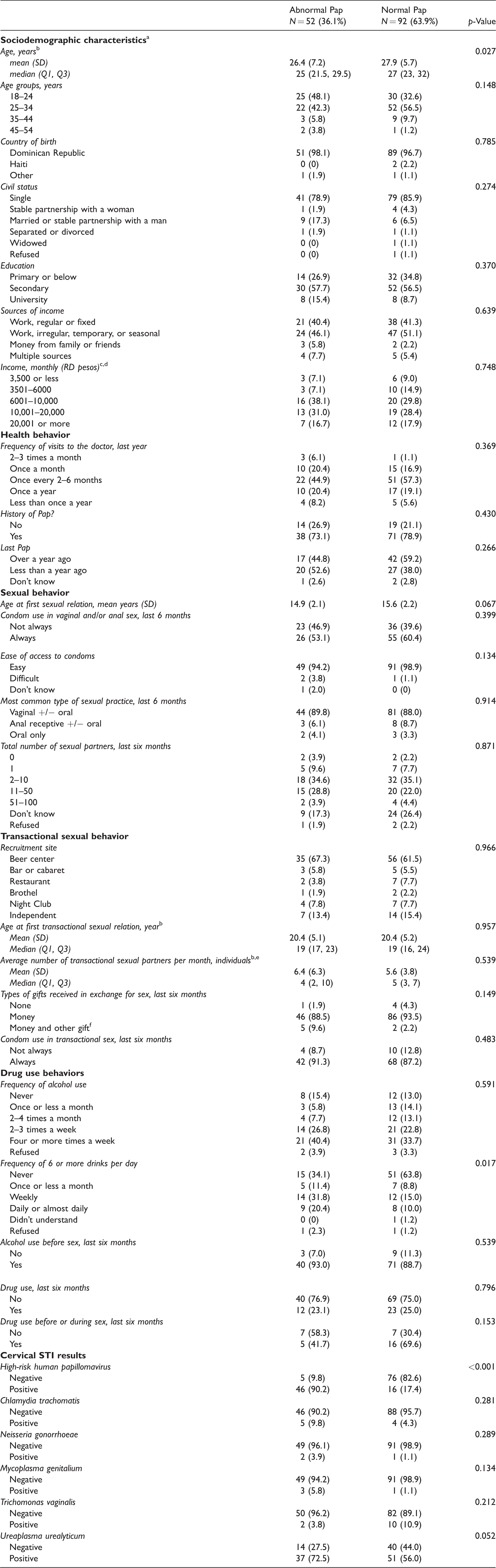
aSection headings from the qualitative interview appear in bold.
bWilcoxon-Mann-Whitney test was used.
cResponse total by Pap result that does not sum to 52 and 92 for Abnormal Pap and Normal Pap, respectively, have missing values.
dAs of March 2018, one Dominican peso equated to $0.02 US dollars.
eThere were 95 responses total; one large outlier was excluded.
fOther gift was defined as services, goods, food, drugs, or rent.
Regression analyses
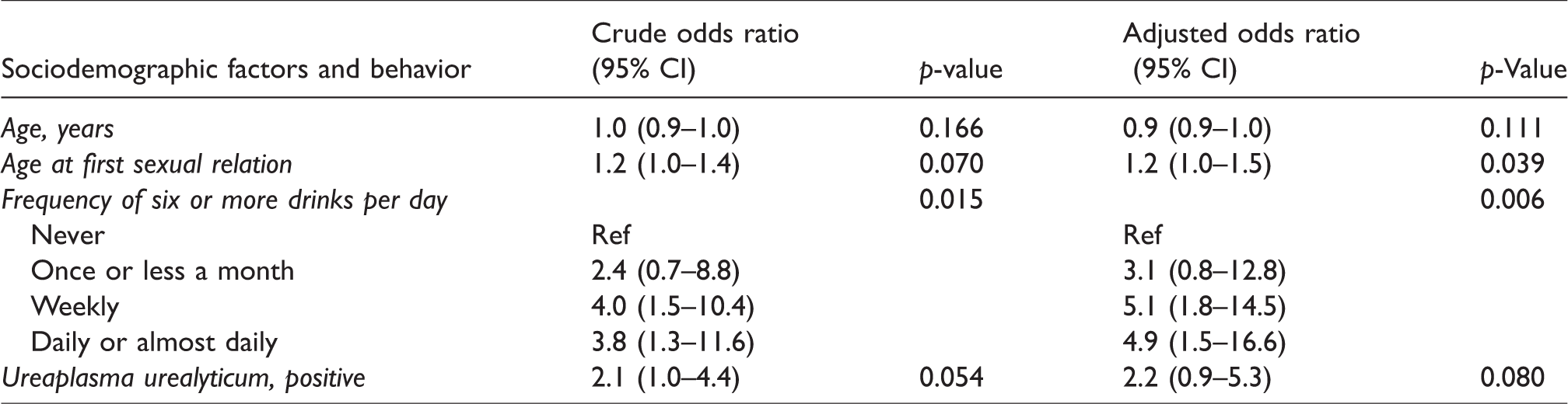
Results of the binary logistic regression model (Table 3) showed binge drinking, weekly (AOR 5.1, 95% CI: 1.8–14.5) or daily (AOR 4.9, 95% CI: 1.5–16.6), and age at first sexual relation (AOR 1.2, 95% CI: 1.0–1.5) were significantly associated with risk of abnormal Pap. Age (AOR 0.9, 95% CI: 0.9–1.0) showed a non-significant trend with abnormal Pap; it was retained in the final model since it is a known risk factor for cervical cancer. Given that in the DR condom use is considered the primary form of contraception despite low access, 19 the variable ‘ease of access to condoms’ was included in our initial regression. In many developing countries, self-reported condom use hinges on access to condoms which may serve as a proxy for understanding condom use. 20 Self-reported condom use was not included in our model as frequencies among women with abnormal Pap and those with normal Pap were similar. The final model (N = 120) approached significance (LR x2 = 21.8, p = 0.001).
Multivariate associations between abnormal Pap results, sociodemographic factors, sexual, and drug use behavior, and cervical STI results of FSWs in La Romana (N = 120).
Discussion
This paper presents the first analysis of Pap results and hrHPV among FSWs in the DR. Almost half of participants had abnormal Pap and hrHPV, suggesting greater HPV burden and cervical cancer risk among FSWs than in the general population. 21 For example, among FSWs in Peru, HPV and hrHPV were detected in 50.6% and 35.6% of women, respectively. 22 In Mexico, HPV prevalence was 48.9% (43% hrHPV) among FSWs. 23 In Latin America, including the DR, recent doctor’s visits were positively associated with recent Pap. 24 In contrast, 73.9% of our sample had seen a doctor multiple times in the last year, yet 76.8% had not received a Pap. Although all were sexually active, 23.2% had never had a Pap. Lack of Pap testing may relate to associated costs, insufficient reinforcement of clinical guidelines, or weak understanding of the relationship between hrHPV and cervical cancer.
A global review of HPV among FSWs estimated that the median overall prevalence was 42.7%, with great variability based on geographic location. 21 Our finding that 43.4% FSWs had hrHPV adds to the review as data from the Caribbean were not included. A 2017 report on HPV and related diseases in the DR indicated that the prevalence of concurrent HPV16 and/or 18 and LSIL in the general population was 7.6%, appreciably lower than the prevalence of HPV 16 and/or 18/45 among FSWs with LSIL in our study (33.3%). 11 In the literature and our analysis, hrHPV infection and abnormal Pap were most common among younger participants, likely due to more frequent metaplastic change of cervical epithelium in youth which increases risk of HPV infection. Cervical cancer is rare among young women because HPV infection is usually transient. 25 However, chronic hrHPV infection acquired in youth has the potential to progress to invasive cervical cancer which validates efforts to vaccinate youth against HPV before sexual initiation. The implementation of the DR’s first vaccination campaign with Cervarix, the bivalent vaccine against HPV16/18, began on 28 April 2017 through a collaboration of the Ministries of Public Health and Education. The vaccine was offered nationwide to 9- and 10-year-old girls at no cost. In our study, we detected an array of high-risk subtypes which could support the utility of implementing the Gardasil 9-valent vaccine for greater protection and coverage at similar cost. 26
Several obstacles to treatment follow-up for abnormal Pap among FSWs exist and are more pronounced in developing countries. A study among FSWs in Peru reported follow-up of only 30% of women with abnormal Pap results; not being informed of abnormal test results was a barrier. 27 Likewise in our analysis, some FSWs (7/61; 10.3%) who qualified for referral were never informed. Of those informed, poor follow-up may have been related to difficulties in communication resulting from the transient nature of FSWs who may frequently migrate between cities in search of anonymity that may reduce sex work-related stigma 28 or for more desirable employment opportunities. National guidelines for the DR, although out of date, recommend colposcopy follow-up for women positive for hrHPV or non-negative Pap with the exception of ASCUS; 14 however, the standard of care at CFLR is colposcopy referral for any non-negative Pap so any woman with precancerous lesions or cancer may be treated while they are present. Among our FSW population, implementing age-dependent cytology and HPV screening strategies 29 ultimately designed for women in the general population in developed settings leads to remarkable loss of follow-up. HPV testing is unavailable on-site and analysis off-site is prohibitively expensive. Based on the financial constraints of complementing cytology with HPV testing, colposcopy is the default form of follow-up for abnormal Pap.
Binge drinking among Dominican FSWs has been reported elsewhere 30 and was significantly associated with abnormal Pap in our study. Binge drinking has been significantly associated with an increased risk of HPV infection 31 and/or low-grade dysplasia in the general population. 32 Additionally, intoxication may increase the likelihood of high-risk sexual behavior and therefore, STI acquisition.33,34 A study of FSW sexual risk behavior in Sosua, DR described pressure to drink excessively with clients, resulting in impaired judgment, intimate partner violence, and compromised family dynamics. 35 Inconsistent condom use, sexual violence, and curable STI diagnoses have been demonstrated among FSWs who binge drink and/or drink before sex.36,37 Inconsistent condom use is associated with greater risk of HPV infection and, in turn, cervical dysplasia, as demonstrated in our analysis. Dominican cultural practices that normalize heavy or frequent alcohol use may be more pronounced among FSWs. A comparison of drinking patterns among Caribbean FSWs showed that 84% of Dominican FSWs were heavy drinkers (six or more drinks daily), more so than Puerto Rican (49.7%) and Haitian (2.7%) FSWs. 38 Also, certain types of transactional sex establishments may facilitate alcohol consumption such as beer centers, from which the majority (63.2%) of our study participants were recruited. In addition to how risky sexual behavior influenced by binge drinking may increase risk of an STI, a pathophysiological mechanism for the relationship between alcohol, HPV infection, and cervical carcinogenesis has been proposed. 39 Acute alcohol intake, as occurs in binge drinking, prevents cells of the innate immune system from effectively detecting, presenting and/or destroying pathogenic antigens. 40 This may modulate humoral and cellular immune responses against HPV antigens and compromise cervical lesion regression.41,42 The relationship between binge drinking and STI risk is complex and may be a focus of alcohol risk management.
Limitations
This analysis has a number of limitations. Self-reported interview responses may be subject to recall and response bias. Participants may have been hesitant to share sensitive details because of stigma or social desirability. Our sample size was small and there were few responses for certain questions. Collapsing variables maximized the number of responses per question but resulted in information loss. Lastly, some participants may have been active within CFLR’s FSWs’ program and would, in that case, represent FSWs already integrated within a clinical network. Their responses and cervical screening results may differ from FSWs who are disconnected from clinical services.
Conclusion
Our results play a critical role in improving the framework for clinical services and strengthening the foundation for future research on hrHPV and cervical cancer among FSWs. Strategies for more effective delivery of results, consistent disclosure of diagnoses, and an emphasis on ensuring follow-up should be developed since loss to follow-up rates were high despite recent contact with the healthcare system. The binge drinking patterns observed in our analysis highlight the importance of addressing alcohol consumption among FSWs in clinical settings. Lastly, research and evaluation of the recent implementation of the first nationwide vaccination campaign is warranted given its potential to prevent HPV infection in youth.
Footnotes
Acknowledgments
We thank the study participants, CFLR clinicians and research team, and the Program for Global and Population Health of Columbia University Vagelos College of Physicians and Surgeons. Jimmy Duong, Sheila Nemeth and Patrick Wong provided statistical guidance.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author SA received financial support from BioReference Laboratories, where the cervical samples for the study were processed and tested.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: During this research, the author SS was supported by the Reducing Health Disparities through Informatics (RHeaDI) training grant (T32NR007969) funded by the National Institute of Nursing Research, National Institutes of Health. The author SA received financial support from BioReference Laboratories.