
Abstract
We assessed prevalence and correlates of bacterial vaginosis (BV) and sexually transmitted infections (STIs) including herpes simplex virus type 2 (HSV-2), gonorrhoea (GC), syphilis (SYP), Chlamydia (CT) and HIV among Kenyan women aged 18–34 years who were screened for a contraceptive intravaginal ring study. Women provided demographic, behavioural and medical information, and underwent medical evaluation, including a pelvic exam. We computed crude and adjusted prevalence ratio (aPR) and 95% confidence interval (CI) using log-binomial regression. Of 463 women screened, 457 provided laboratory specimens and were included in the analysis. The median age was 25 years, interquartile range (21–28), and 68.5% had completed primary or lower education. Overall, 72.2% tested positive for any STI or BV. Point prevalence was 55.6, 38.5, 3.9, 2.0, 4.6, and 14.7% for HSV-2, BV, GC, SYP, CT, and HIV, respectively. Co-infection with HSV-2, BV, and HIV occurred in 28 (6.1%) participants. Having ≥1 STI/BV was associated with younger age at first sex (≤13 versus 17–19 years, aPR=1.27, 95% CI 1.07–1.51), history of exchange sex (aPR = 2.05, 95% CI 1.07–3.92), sexual intercourse in the past seven days (aPR = 1.17, 95% CI 1.01–1.36), and older age (30–34 versus 18–24 years, aPR = 1.26, 95% CI 1.06–1.48). STI/BV diagnosis was less likely for women reporting one lifetime sexual partner compared to women with ≥4 lifetime sexual partners (aPR = 0.70, 95% CI 0.54–0.92). Combination prevention approaches (biomedical, behavioural, social, and structural) tailored to women with diverse risk profiles may help mitigate STI/BV prevalence in this setting.
Introduction
A more robust commitment to sexually transmitted infections (STIs) prevention, diagnosis, and treatment is needed given that more than one million new STIs are acquired globally every day. 1 Worldwide, Chlamydia (CT) accounts for 131 million of those new STIs, gonorrhoea (GC) for 78 million, syphilis (SYP) for 5.6 million, and trichomoniasis for 143 million cases annually. 1 Left untreated, STIs can lead to severe acute and chronic sequelae, e.g. infertility, pelvic inflammatory disease, unfavourable pregnancy and perinatal outcomes. 2 Importantly, STIs may also facilitate the risk of sexual transmission and acquisition of HIV among women in sub-Saharan Africa (SSA).3–5 Condoms are theoretically highly effective in preventing STIs and unintended pregnancy; however, inconsistent use makes these less effective in protecting against either. 6 Women not using condoms with hormonal contraceptive methods (dual use) may be at increased risk of infection. Lack of STI prevention education, absence of routine STI screening, and limited access to STI services may lead to lower STI testing among contraceptive-using women.
STIs, especially HIV, overall are a leading cause of disease in Kenya. 7 Emphasis on HIV, however, may minimize attention given to other STIs. 7 STI control is predominately subsumed within HIV programme priorities. STI control relies on syndromic management and diagnostic testing is largely unavailable. To our knowledge, Kenya’s national prevalence and incidence data for STIs other than HIV are unavailable. Data collection typically includes self-report of genital ulcers and abnormal genital discharge as opposed to diagnosis of specific STIs, and health programmes rely on such syndromic surveillance and management rather than more specific testing.
The 2012 Kenya AIDS Indicator Survey showed that 0.9% of adolescents and adults aged 15–64 years of age self-reported having an STI (based on presence of genital ulcers and abnormal genital discharge) in the past 12 months, and that among those diagnosed with an STI, about 70% indicated that they had received treatment. 7 A prospective cohort study conducted in Mombasa, Kenya, found an association between HIV and trichomoniasis among women. 8 Some studies conducted in SSA suggested that prevalent genital herpes simplex virus type 2 (HSV-2) may increase acquisition of a new HIV infection. A longitudinal analysis of a cohort of high-risk Zimbabwean and Ugandan women showed that the population attributable risk of prevalent HSV-2 on HIV acquisition remained chronically high at approximately 50%. 9 This study also demonstrated a causal link between HSV-2 infection and disruption of the vaginal microbiota leading to a higher prevalence of bacterial vaginosis (BV) among Kenyan women with HSV-2. 9 BV is known to expedite lower genital tract HIV shedding and transmission.10–12 It has been shown to diminish vaginal acidity and lactic acid levels, thereby increasing susceptibility to other STIs in addition to facilitating innate immune response associated with acquisition of HIV.13–16 Laboratory studies have demonstrated that CT infection of endocervical endothelial cells may facilitate HIV crossing the mucosal barrier and targeting the underlying cells. 13
A systematic review of epidemiological studies conducted from 1986 to 2006 in SSA countries showed an association between HIV infection and number of sex partners, history of paid sex (transactional or commercial sex), and HSV-2 infection or other STIs. 17 A more recent review of the socio-demographic and behavioural risk factors of female sex workers in SSA demonstrated linkage of HIV risk to limited economic opportunities, multiple dependents, marital disruption, low education, gender-based violence, erratic condom use, higher number of clients, heavy episodic drinking, duration of sex work ≥3 years, STI co-infection, and engaging in anal sex. 18
Global STI and HIV studies typically focus on high-risk individuals such as antenatal clinic attendees, sex workers, and men who have sex with men, while information on women from the general population is limited. 19 Thus, our objectives were to (1) describe the baseline prevalence of SYP, GC, CT, HSV-2, HIV, and BV, among contraceptive-using women from the general female population screened for a contraceptive intravaginal ring study; and (2) identify behavioural and demographic factors associated with prevalent STI or BV infections, including HIV.
Material and methods
Ethical statement
The Scientific Ethical Review Unit of the Kenya Medical Research Institute; an Institutional Review Board for the US Centers for Disease Control and Prevention; and the Kenya Pharmacy and Poisons Board reviewed and approved the study protocol, consent forms, and data collection instruments. This trial is registered with ClinicalTrials.gov, number NCT02529683. Prior to administering a brief pre-screening assessment (described below), volunteers completed a verbal informed consent process in English, Kiswahili, or Dholuo, the three most common languages in our study’s geographical setting. Volunteers did not receive any incentives for completing the brief pre-screening questionnaire. Women proceeding to a more detailed behavioural and medical screening completed written informed consent, also available in each of the aforementioned languages, before initiation of data collection, medical procedures, and testing. Women taking part in the in-depth data and specimen collections received a bar of soap, 500 Kenya Shillings (approximately $5 USD) for transport, feminine sanitary pads, and a treated malaria bed net.
Setting and design
Between April 2014 and November 2014, we undertook recruitment, screening, and enrolment for an open-label, single group observational study of the contraceptive intravaginal ring, NuvaRing®. Study procedures have been described elsewhere. 20 Contraceptive-using women 18–34 years of age were drawn from the general population as opposed to specific key populations at increased risk of HIV or other STIs.
Our catchment area included Kisumu and surrounding villages within a 150-km radius. In brief, with the assistance of ten community health workers, we used convenience sampling to conduct venue-based recruitment in village gathering places and family planning clinics. In addition, participant referral without incentive occurred. Within our recruitment venues, the study staff delivered a study overview and obtained verbal consent privately from the interested volunteers in their preferred language (English, Swahili, or Dholuo) before administering a brief pre-screening computer-assisted personal interview (CAPI). Women who met the pre-screening criteria listed in Table 1 presented for a clinic-based screening visit, which involved an in-depth behavioural and medical eligibility assessment.
Eligibility criteria for the Kisumu Contraceptive Intravaginal Ring Study, Kisumu, Kenya, 2014.
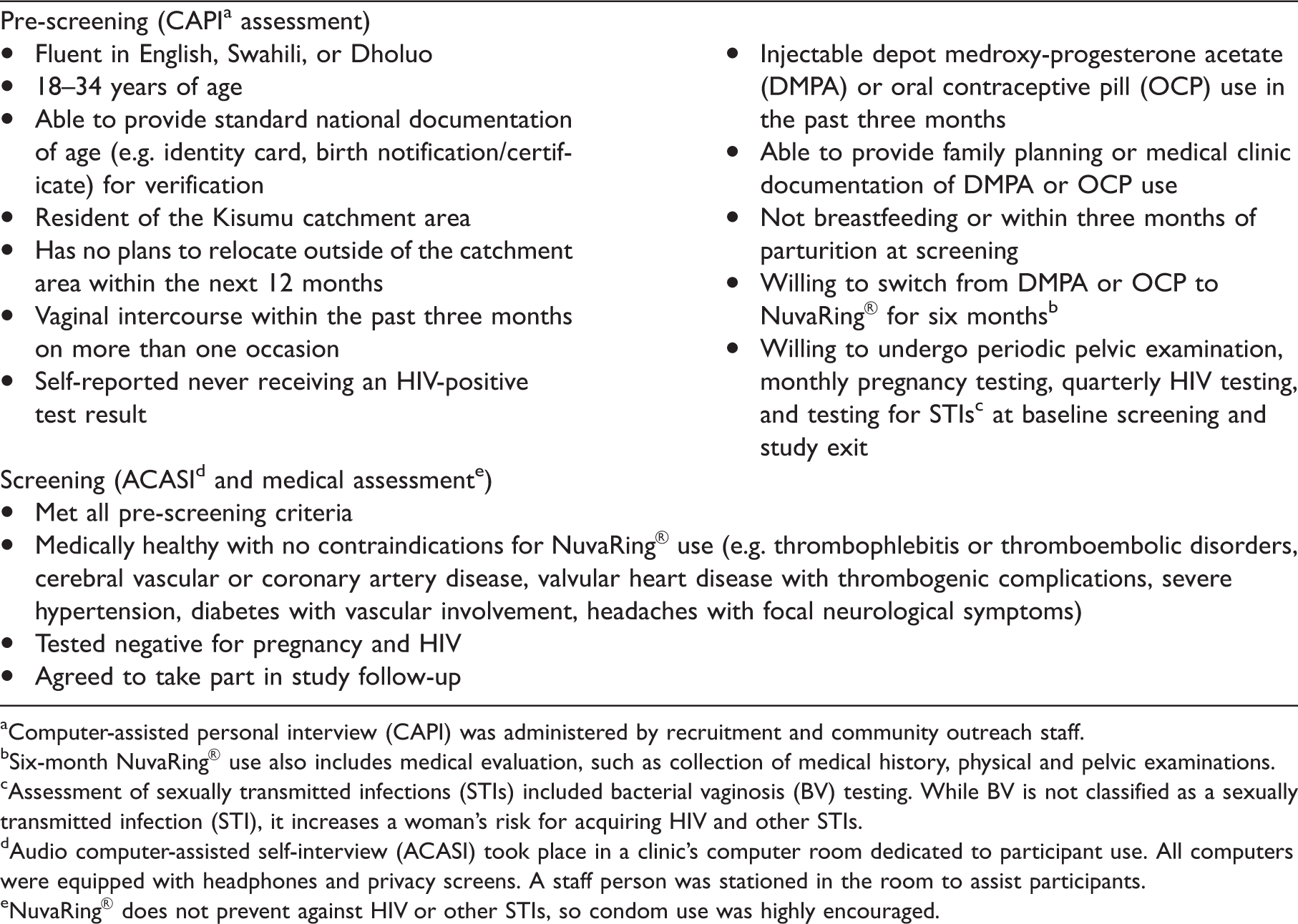
aComputer-assisted personal interview (CAPI) was administered by recruitment and community outreach staff.
bSix-month NuvaRing® use also includes medical evaluation, such as collection of medical history, physical and pelvic examinations.
cAssessment of sexually transmitted infections (STIs) included bacterial vaginosis (BV) testing. While BV is not classified as a sexually transmitted infection (STI), it increases a woman’s risk for acquiring HIV and other STIs.
dAudio computer-assisted self-interview (ACASI) took place in a clinic’s computer room dedicated to participant use. All computers were equipped with headphones and privacy screens. A staff person was stationed in the room to assist participants.
eNuvaRing® does not prevent against HIV or other STIs, so condom use was highly encouraged.
Before initiating in-depth screening procedures, all women provided written informed consent on the second more comprehensive form describing study follow-up and contraceptive ring use. Collection of demographic and behavioural information took place using audio computer-assisted self-interview (ACASI). To facilitate computer use, all women completed a self-directed, hands-on tutorial before beginning the ACASI questionnaire. A study clinician administered a medical evaluation CAPI, which included questions on three symptoms potentially indicative of an STI (currently having genital ulcers anywhere on the vagina and/or vulva, abnormal or smelly vaginal discharge, or pain during sexual intercourse), and performed a general physical examination as well as a pelvic examination. We used the collected venous blood samples for rapid and confirmatory testing of HIV using Determine HIV-1/2 Ag/Ab Combo test and Biorad 3rd Gen enzyme-linked immunosorbent assay (ELISA), testing of HSV-2 using Kalon IgG HSV-2 ELISA, a screening Plasma Reagin and confirmatory SD Bioline SYP testing, and performed real-time polymerase chain reaction testing of GC and CT using COBAS AMPICLOR/COBAS Taqman assay on self-collected vaginal swab samples. We also performed BV assessment using Nugent Scoring (Gram stain of vaginal swab) and tested the collected urine samples for pregnancy using SAS Ultra human chorionic gonadotropin test. Rapid HIV testing and delivery of results as well as pre- and post-test counselling followed Kenyan Ministry of Health guidelines. 21
Women who tested positive for SYP, GC, or CT received free treatment, which was consistent with national and World Health Organization guidelines, and were encouraged to invite their sexual partners to the study clinic for free STI testing and treatment. Women testing positive for HSV-2 did not receive treatment unless they had active skin infection with vesicles. Women who tested HIV-positive received additional counselling, CD4 and viral load testing, and referred to a patient support centre for appropriate HIV care services. Women who tested positive for pregnancy at screening received referrals to local antenatal care clinics and services.
Statistical analysis
We descriptively characterized women who completed the in-depth screening by frequencies and percentages for demographic, sexual history, vaginal health, and recent behavioural variables.
The dependent variable for our analysis combined laboratory screening test result for any STI (SYP, GC, CT, HSV-2, HIV) or BV and is henceforward referred to as STI/BV. Employing generalized linear modelling framework and log-binomial regression, we modelled occurrence of STI/BV and compared it among categories of explanatory variables using crude and multivariable-adjusted prevalence ratio (aPR) and 95% confidence interval (CI). Variables significant at the 0.2 level in univariable analysis underwent further examination using a multivariable regression model. Potential confounding effect of each covariate and two-way interactions was addressed and we obtained final variable selection by applying backward elimination and retaining predictors significant at the 0.05 level. The analyses were completed using STATA version 14.1 (STATA Corporation, College Station, Texas, USA).
Results
Characteristics of the study population
Of 692 pre-screened women, 463 completed the in-depth screening. Our analysis was restricted to 457 women who provided laboratory specimens. Among the 457 women, 47.5% were 18–24 years of age, 68.5% had completed primary or less education, including no schooling. Approximately one-third (31.2%) reported having been inherited (a traditional cultural practice - see Table 2). An estimated 63.8% reported being unemployed (Table 2). Among the current symptoms potentially indicative of an STI/BV, which were provided by 456 out of the 457 screeners, genital ulcers were self-reported by 2.4%, abnormal or smelly discharge by 3.1%, and pain during sexual intercourse by 6.1% (data not shown).
Demographic and behavioural characteristics of women at screening (n = 457), by sexually transmitted infection or bacterial vaginosis (STI/BVa) status, for the Kisumu Contraceptive Intravaginal Ring Study, Kisumu, Kenya, 2014.
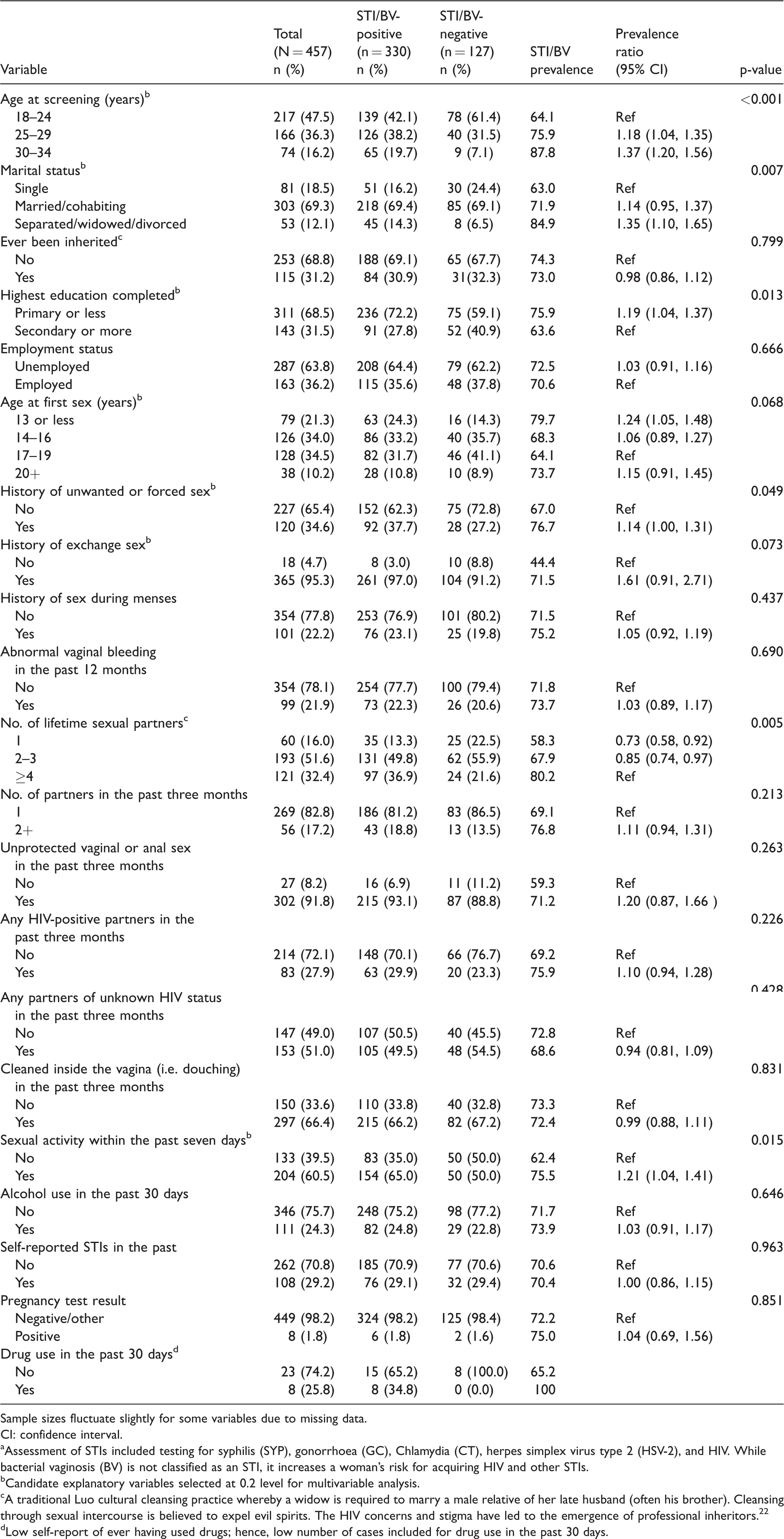
Sample sizes fluctuate slightly for some variables due to missing data.
CI: confidence interval.
aAssessment of STIs included testing for syphilis (SYP), gonorrhoea (GC), Chlamydia (CT), herpes simplex virus type 2 (HSV-2), and HIV. While bacterial vaginosis (BV) is not classified as an STI, it increases a woman’s risk for acquiring HIV and other STIs.
bCandidate explanatory variables selected at 0.2 level for multivariable analysis.
cA traditional Luo cultural cleansing practice whereby a widow is required to marry a male relative of her late husband (often his brother). Cleansing through sexual intercourse is believed to expel evil spirits. The HIV concerns and stigma have led to the emergence of professional inheritors. 22
dLow self-report of ever having used drugs; hence, low number of cases included for drug use in the past 30 days.
Overall, 72.2% (330/457) tested positive for STI/BV. The prevalence was 55.6% for HSV-2, 38.5% for BV, 14.7% for HIV, 4.6% for CT, 3.9% for GC, and 2.0% for SYP. Any three simultaneous infections occurred in 33 (7.2%) cases. Co-infection with HSV-2, BV, and HIV occurred in 28 (6.1%) participants. Among 67 (14.7%) women testing HIV-positive, 81.8% tested positive for HSV-2, 48.5% for BV, 10.6% for GC, and 1.5% for SYP (data not shown).
Univariable analysis
Univariable analysis showed that testing positive for our combined STI/BV outcome variable was more likely for women who were 25–29 years of age (PR = 1.18, 95% CI 1.04–1.35) or 30–34 years (PR = 1.37, 95% CI 1.20–1.56) compared to 18- to 24-year-olds, were separated/widowed/divorced (PR = 1.35, 95% CI 1.10–1.65) compared to single, had primary or less education (PR = 1.19, 95% CI 1.04–1.37) compared to those with secondary or more education, had history of unwanted or forced sex (PR = 1.14, 95% CI 1.00–1.31), or were sexually active within the past seven days (PR = 1.21, 95% CI 1.04–1.41) (Table 2).
Testing positive for STI/BV was less likely for women reporting having one (PR = 0.73, 95% CI 0.58–0.92) or 2–3 (PR = 0.85, 95% CI 0.74–0.97) lifetime sexual partners compared to those with ≥4 lifetime sexual partners (Table 2).
Table 3 shows the association between age at screening and BV, HSV-2, and HIV status, separately. Compared to women who were 18–24 years of age, those 25–29 years of age and those 30–34 years of age were more likely to be infected with HSV-2 (PR = 1.40, 95% CI 1.15–1.70 and PR = 1.87, 95% CI 1.55–2.26, respectively) or HIV (PR = 1.84, 95% CI 1.11–3.06 and PR = 1.87, 95% CI 1.01–3.45, respectively).
Association of age with bacterial vaginosis (BV), herpes simplex virus type 2 (HSV-2), and HIV at screening (n = 457) for the Kisumu Contraceptive Intravaginal Ring Study, Kisumu, Kenya, 2014.

CI: confidence interval.
Sample sizes fluctuate slightly for some variables due to missing data.
CI: confidence interval.
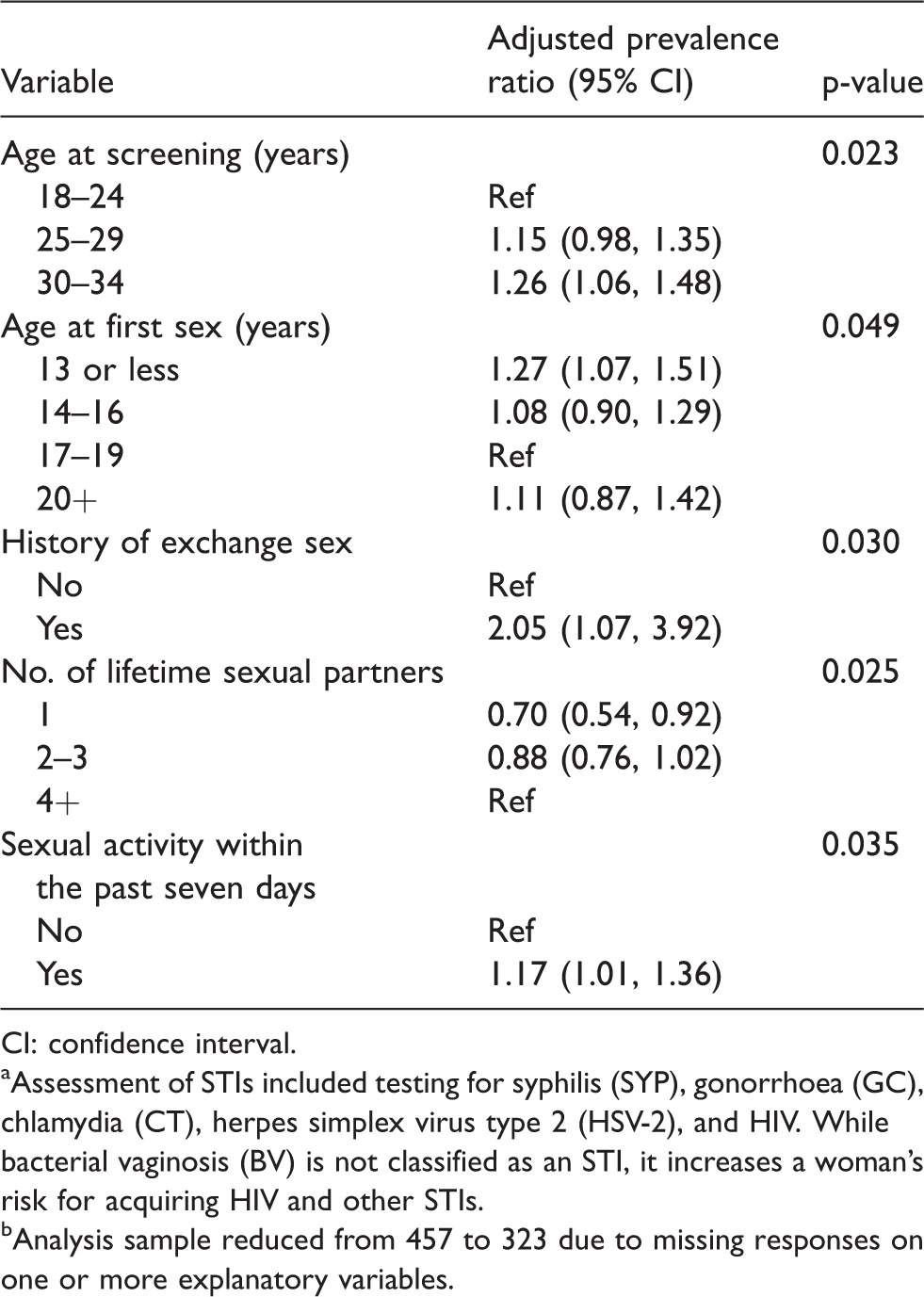
aAssessment of STIs included testing for syphilis (SYP), gonorrhoea (GC), chlamydia (CT), herpes simplex virus type 2 (HSV-2), and HIV. While bacterial vaginosis (BV) is not classified as an STI, it increases a woman’s risk for acquiring HIV and other STIs.
bAnalysis sample reduced from 457 to 323 due to missing responses on one or more explanatory variables.
Multivariable analysis
Testing positive for STI/BV increased with age and was highest among those aged 30–34 years (aPR=1.26, 95% CI 1.06–1.48) compared to those aged 18–24 years; it also showed positive association with early age at first sex (≤13 years) compared to those who initiated sexual activity at 17–19 years (aPR = 1.27, 95% CI 1.07–1.51), history of exchange sex (aPR = 2.05, 95% CI 1.07–3.92), and reporting sexual activity within the past seven days (aPR = 1.17, 95% CI 1.01–1.36) (Table 4). Testing positive for one or more STI/BV was less likely among women reporting one lifetime sexual partner compared to women reporting four or more lifetime sexual partners (aPR = 0.70, 95% CI 0.54–0.92) (Table 4).
Discussion
Among sexually-active, contraceptive-using women screened for a contraceptive intravaginal ring study in Kisumu, Kenya, 72.2% tested positive for STI/BV. This prevalence is consistent with estimates obtained from high-risk women 18–35 years of age surveyed in Beira, Mozambique 23 and other SSA countries.24,25 Co-infection with BV, HSV-2, and HIV in our sample further supports potential relationships between imbalances in the vaginal microflora that increased risk for either viral or bacterial infections. While prevalence of BV was high among our sample of women, it is somewhat lower than what has been reported for studies targeting high-risk women.26,27 This may be due to our recruitment approaches and eligibility criteria which focused on current contraceptive use rather than specific risk behaviour characteristics.
We found that HSV-2 was the most prevalent STI in our sample. We observed HSV-2 infection among slightly more than half of the women who completed the in-depth behavioural and medical screening. HSV-2 infection has been independently associated with increased risk of HIV-1 acquisition. Compared to other studies, we observed a higher HSV-2 prevalence that may be explained by age and other differences in study populations. A Kenyan population-based household survey found 42.0% prevalence of HSV-2 among women aged 15–64 years. 28 Kisumu Incidence HIV Cohort study, likewise, found HSV-2 and HIV prevalence of 44.8 and 21.2%, respectively, among women. 29 In one meta-analysis, HSV-2 was associated with a three-fold risk of HIV-1 among women in the general population. 30
Our findings also showed the association between several demographic characteristics and testing positive for STI/BV. The higher likelihood of testing positive for STI/BV among women 30–34 years, as compared to those 18–24 years, may have multiple explanations. Older women of reproductive age may be more likely to have long-standing vaginal infections, including those transmitted via sexual activity due to lasting exposure and limited access to diagnostic and treatment services. These women may be less educated and have less awareness of STI symptoms; therefore, have greater fear of stigmatization and higher rate of underreporting. Later life marital status change (divorce, separation, or widowhood) may lead some women to new sexual networks with high STI prevalence, or situations whereby sex is exchanged for protection, economic, social standing, or other reasons.31–33
In our sample, the low number of participants reporting symptoms potentially indicative of an STI could mean that women were not willing to report these symptoms or that they may have been asymptomatic. While a comprehensive syndromic assessment was not undertaken, our findings suggest that without aetiologic testing, a syndromic management approach could increase the likelihood of missed STIs for some women.
We observed an increased risk of acquiring STI/BV for those with age of ≤13 years at first sex. Other studies have likewise shown that women who experience first sex at an early age are more likely to have STIs and engage in risky sexual behaviour (e.g. having multiple partners, low use of condoms, and inconsistent or incorrect contraceptive use). 34 Early age at first sex is associated with a variety of biological, sociocultural, behavioural, and structural factors that act separately and together to increase poor sexual and reproductive health outcomes for adolescent girls, including unintended pregnancy as well as HIV or other STIs. 35 An immature genital tract has been shown to have larger areas of cervical ectopy and trauma during sexual intercourse thereby facilitating infections. 36 Moreover, contextual factors (e.g. poverty, gender norms, power relations, menstrual care issues, sexual scripts, relationships with boyfriends) may undervalue the education of females and drive adolescent girls and young women to drop out of school, which then has implications for sexual activity as well as early marriage. 35
Lastly, our study suggests that sexual partners were important factors for having STI/BV. Among women in our study, self-reported sexual activity with one lifetime partner presented a 30% less likelihood of testing positive for any STI compared with women with four or more lifetime partners. Other studies have also correlated STI prevalence with sexual practices such as having many lifetime sexual partners.37–39 A systematic review found that BV was significantly associated with an increased number of male sex partners or having a recent change of male partner. 40 Moreover, this systematic review indicated that observational data suggest that epidemiologic profile of BV was similar with other STIs. 40
Prior SSA studies proposed that exchange sex, which may be characterized by transactional sex, plays a key role in women’s risk of acquiring HIV and other STIs. 41 History of intimate partner violence, alcohol use, multiple and concurrent partnerships, and non-use of condoms are plausible documented mechanisms linking transactional sex as well as sex work with HIV and STIs.42–45 While a recent definition of transactional sex as ‘non-commercial, non-marital sexual relationships motivated by the implicit assumption that sex will be exchanged for material support or other benefits’ 46 is helpful from a research perspective, the motivational, behavioural, and sociocultural complexities associated with it require greater attention. Additional information is needed to understand better the contribution of cultural practices that endorse resource redistribution and reciprocity within the context of courtship to exchange dynamics within a sexual relationship. 47
Strengths and limitations
Our analysis enabled us to examine demographic, behavioural, and biological correlates of the prevalent STIs. There were several limitations associated with our study. First, our sample size and recruitment approach did not permit generalization of the findings. The limited sample, particularly, restricted the power for assessing factors’ association with STI/BV prevalence among subgroups. Because we targeted women in the general community by behaviour (i.e. use of injectable and oral contraception), rather than by risk category, findings may also not be generalizable to particular risk groups. Nonetheless, our findings suggest that high prevalence of STI/BV is not restricted to key populations and possibly should be of broader public health concern in this setting. Second, while ACASI may have helped reduce the possibility of social desirability and other response bias shown with self-reported sexual risk behaviours, under-reporting may still have occurred. Third, our analysis was cross-sectional, so the direction of associations cannot be determined, and STI incidence information for our sample is absent. Fourth, the HIV, SYP, and HSV-2 serological tests did not distinguish between recent and past infections. Fifth, lack of specificity in our screening questions regarding diagnosis and treatment of BV or any STIs in the past does not permit us to examine whether treatment of primary infections reduces immunity to subsequent secondary infections. Last, correlates of STI/BV provide no evidence in terms of interventions that are likely to be effective in preventing these infections.
Conclusion
STIs are under-addressed diseases in settings with high HIV prevalence, especially among women in the general population. In general, most STIs among women may be asymptomatic; therefore, there is an increased likelihood that they will go untreated. Combination prevention approaches (biomedical, behavioural, social, and structural) tailored to women with diverse risk profiles may help mitigate STI prevalence in this setting. Syndromic management of STIs (prevailing in resource-poor settings) addresses symptomatic manifestations; yet, to alleviate burden of highly prevalent STIs, especially those associated with increased risk of HIV infection, a routine screening with high-quality diagnostics is warranted. Development of reliable, user-friendly, affordable STI point-of-care tests for use in resource-limited countries is needed.
Footnotes
Authors’ contribution
VOO, MAD, EML, RG, BN, VA, GO, and MM contributed substantially to the conceptualization and development of the research study and its implementation.VOO, EML, GO, RG, DAG, and MAD were involved significantly in the analysis and interpretation of data.MM and BN were involved substantially in the acquisition of data and clinical management of the study.All authors have substantially contributed to drafting and revising this work for important intellectual content, approved the final version, and bear responsibility for its accuracy and integrity.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.