
Abstract
We report a case of a concurrent reactivation of varicella zoster virus and herpes simplex virus in an immunocompromised patient unaware of her longstanding human immunodeficiency virus (HIV) infection. Despite being a rare event, concurrent reactivation of the two alphaherpesvirinae has been reported in various conditions, either in immunocompetent or immunocompromised patients. However, a reactivation in the same anatomical location in a person living with HIV seems to be an extremely rare event.
Introduction
Varicella zoster virus (VZV) and herpes simplex virus (HSV) are two herpes viruses belonging to the same subfamily of alphaherpesvirinae. Although they share many similar characteristics such as neurotropism and latency, differences include recurrence rate, age of reactivation, mechanism of reactivation and latency. Contrary to VZV, HSV is associated with complete transcriptional repression of the virus genome. We present a case of concomitant HSV and VZV reactivation that is reported to be a rare event, especially if it concerns the same anatomic site. 1 The diagnosis in our patient was made from the swab of the base of an unroofed skin vesicle, this a presenting sign of human immunodeficiency virus (HIV) infection. Implications for clinical practice, specifically the indication for HIV testing in the setting of shingles, together with herpes virus typology and disease management are discussed.
Materials and methods
We report the case of a patient who presented in December 2017 to the emergency department of our institution (Jules-Gonin Eye Hospital, University of Lausanne) with a right ophthalmic zoster. Complete ophthalmic examination at first and subsequent visits included visual acuity (Snellen chart), slit-lamp examination, intraocular pressure measurement and fundus examination. A swab of a single skin vesicle was obtained at initial presentation from vigorous swabbing of the base of an unroofed vesicle. This was analyzed using qualitative isothermal helicase-dependent amplification, and later confirmed by real-time polymerase chain reaction in a reference laboratory. Serology was positive for HIV with negative p24 antigen, confirmed by immunoblot (HIV-1 positive) and nucleic acid amplification test for RNA virus quantification.
The patient was treated in collaboration with the infectious diseases division of the Lausanne University Hospital (CHUV) for the HIV infection. A review of the literature was performed on PubMed and Google Scholar in the search for similar cases with concomitant herpetic reactivation.
Results/case report
A 54-year-old woman presented at the emergency department of Jules-Gonin Eye Hospital with a right ophthalmic zoster of onset five days previously. Prior ophthalmic history was unremarkable. Her medical history revealed an unclear pulmonary shadowing in the chest X-ray, currently under investigation. For this reason an HIV test was performed.
On presentation, there were multiple vesicles of her right V1 dermatome and crusts. Visual acuity was reduced to 0.7 in the affected eye. Slit-lamp examination showed an injected conjunctiva, dendritic lesions on the cornea but no anterior chamber flare or cells. Fundus examination was normal. The left eye was normal. An oral antiviral treatment of 1 g valaciclovir TID with a local lubricant six times a day was initiated.
One day later, the patient presented with minor anterior chamber cells and flare, followed on day 5 by granulomatous anterior uveitis. Treatment with 1% prednisolone acetate five times a day with 0.25% scopolamine TID was started and the vesicular eruption and uveitis resolved after 10 and 16 days, respectively. The treatment with 1 g valaciclovir TID was continued until complete resolution of the uveitis and skin eruption.
The HIV test was positive for HIV-1 with a viral load of 51,000 copies/ml in the context of a CD4 cell count of 557 cells/mm3. An antiretroviral regimen with emtricitabine, tenofovir alafenamide and dolutegravir was initiated by the infectiologists. Analysis of the skin vesicle sample was highly positive for HSV type 1 with 663,000,000 copies/ml and VZV with 44,400,000 copies/ml.
Discussion
We describe a case of concomitant reactivation with two different alphaherpesvirinae in a patient with a previously undiagnosed HIV infection. Although this is a rare event, especially if it concerns the same anatomical region, the literature reports cases of concomitant reactivation of Herpesviridae under different conditions, which are reviewed in Table 1.
List of reported cases of herpetic coinfections.
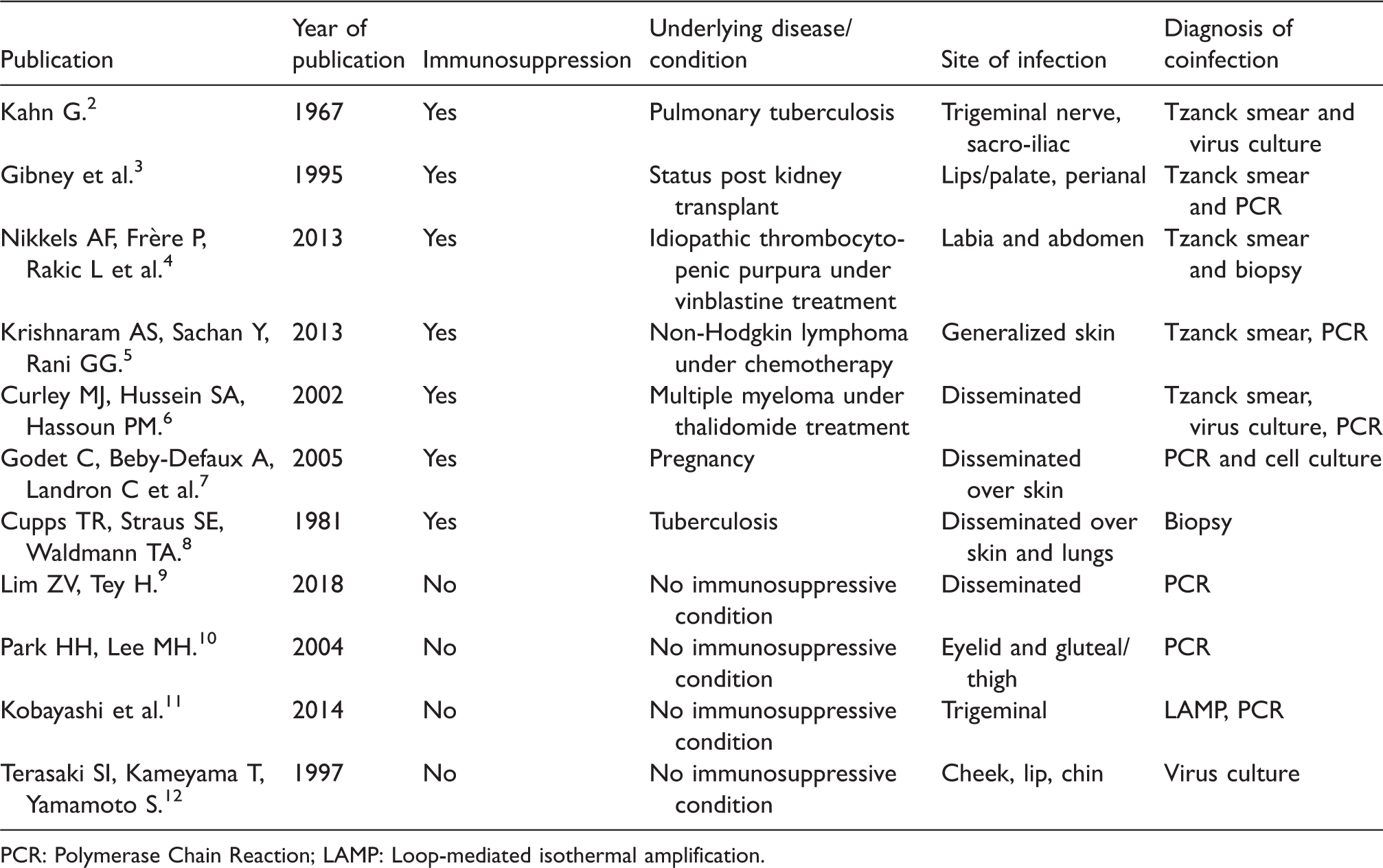
PCR: Polymerase Chain Reaction; LAMP: Loop-mediated isothermal amplification.
In our patient, the immune status of the host presenting an immunodeficiency infection due to HIV-1 could be a risk factor for simultaneous HSV and VZV reactivation, since the HIV targets the cellular-mediated immune system. However, we could not find a reported case of a concomitant HSV and VZV reactivation in the context of HIV or AIDS.
According to the literature, concomitant reactivation of Herpesviridae is not exclusively seen in immunocompromised patients, but also occurs in immunocompetent patients, where it frequently involves the same dermatome. A retrospective study by Giehl et al. identified 20 cases (1.2%) of concomitant VZV and HSV infection at the same body site of 1718 patients with suspicious skin lesions by polymerase chain reaction (PCR) analysis. Remarkably, all patients were immunocompetent.
Cadaveric studies confirm the presence of latent HSV and VZV in the same neuron in human trigeminal ganglia. 13 To better understand the process of dual infection, a recently published study by Sloutskin et al. 14 tried to reproduce VZV and HSV-1 co- and superinfection in an experimental laboratory setting on human foreskin fibroblasts and human neurons. They demonstrated that co-infection with HSV-1 or VZV, either with itself or the other virus, is more likely in neurons than in human foreskin fibroblasts. Similarly, superinfection of VZV and HSV-1 by the virus itself or the other virus is more efficient in neurons than in human foreskin fibroblasts. Co-infection and superinfection of a single neuron with two alphas Herpesviridae alphaherpesvirinae is thus possible, according to their study.
Although HSV and VZV belong to the same herpes family of the alphaherpesvirinae and share similar characteristics such as latency and neuro- and epidermotropism, they can be distinguished by different biological and clinical properties. Firstly, the two alphaherpesvirinae have markedly different reactivation frequencies. 15 HSV reactivation may occur symptomatically and/or produce asymptomatic virus shedding hundreds of times over a lifetime. The frequency is especially high in the period after primary infection, which usually occurs at a young age. 15 The frequency of VZV reactivating as herpes zoster is much lower and increases with age. This suggests that the immunity for HSV increases with the number of episodes of reactivation, whereas the increase in herpes zoster reactivation is thought to be associated with decreased VZV-specific T-lymphocyte proliferation.16,17 Secondly, it is suspected that different mechanisms trigger reactivations, which explains why a concomitant reactivation is rare. 3 , 15 , 18 HSV reactivation is associated with predisposing factors such as UV-light exposure, trauma, fever, immunosuppression, physical and emotional stress, 19 whereas VZV does not necessarily reactivate after a stimulus. 20
A mechanistic model to explain the different behaviors of the two Herpesviridae was provided by Meier and Straus: they postulated that in HSV the viruses remain latent in the neuronal nuclei, whereas in VZV they reside in nonneuronal satellite cell nuclei. Therefore, in HSV a neuronal stimulus could act on the neuron leading to a localized mucocutaneous eruption. In VZV, however, the satellite cells where the virus resides could be less influenced by neuronal stimuli, but once activated yield a more extensive response due to cell-to-cell transmission of the virus, with increased neuralgia. Although the mechanisms of herpes latency and reactivation are not clearly understood, Lungu et al. propose a different molecular mechanism to maintain latency for herpes simplex and VZV. They postulate that whereas latency in HSV is associated with almost complete transcriptional repression of the virus genome, VZV latency results from the absence of nuclear import of virus proteins responsible for regulation of gene expression and/or DNA replication. 22 These different molecular mechanisms could explain why a concomitant reactivation is a rare event, as different triggers might be required to move a latency state to an active infection. Reactivation of a latent virus could be related to depressed cellular immunity because of a primary infection with another herpes virus. 2 However, there is no proven concept to date.
The diagnosis of a concomitant reactivation can nowadays be made with a PCR analysis, or even more easily with a loop-mediated isothermal amplification assay from a skin vesicle swab, as suggested by Kobayashi et al. 11 The likelihood of diagnosing a concomitant infection is much greater with these techniques than with the previously used culture-based approaches, since HSV destroys cell monolayers and often makes VZV diagnosis impossible.
Our case is remarkable and unique because it showed acute simultaneous reactivation of HSV-1 and VZV, with a very high viral load as the presenting sign of HIV in a patient aged over 50 years. HIV testing is indicated in patients less than 50 years of age presenting with shingles but, as our case shows, it should also be considered in older patients if a concomitant infection is present (in our case a pulmonary lesion). 23 Concomitant reactivation of different alphaherpesvirinae is rare and can be diagnosed by a skin vesicle swab. 24 Virus typology can be important in the context of HIV as atypical infections and resistance to antiviral treatment are more likely.16,17,25,26 The treatment depends on the CD4 cell count and the clinical severity (restricted to one dermatome or extended). In restricted infections, oral antiviral agents are indicated, whereas in the case of extensive involvement, intravenous treatment should be given until the eruption clearly resolves. 27
Footnotes
Authors’ contribution
All authors were substantially involved in conception and design. All authors contributed in drafting or revising the article and approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.